
Abstract
Abstract
Background:
To analyze treatment modalities and results in patients with severe odontogenic maxillofacial infections during a 10-y period.
Methods:
Medical records of 1,077 patients hospitalized because of severe odontogenic maxillofacial infections during 2003–2012 were reviewed. The sample consisted of the records that matched inclusion criteria. For each patient the following data were collected: Age, gender, presence of systemic diseases, length of hospital stay, causal tooth, location of inflammation, treatment, results of bacteriologic sampling, and anti-bacterial susceptibility.
Results:
Male to female ratio was 1.4:1. Two or more anatomic spaces were involved in 42.9% of cases, 37.3% of which involved the floor of the mouth. Penicillin in combination with gentamicin or metronidazole was prescribed in 69% of cases. Sixty-two different micro-organism species were identified with predominance of Streptococcus haemolyticus (42.9%). The microbial analysis showed the highest susceptibility of predominant micro-organisms to penicillin was 76.9% and the highest resistance was to metronidazole (27.9%).
Conclusions:
The frequency of odontogenic maxillofacial infection remained almost unchanged during a 10-y period. Single-space infections were more common (57.1%) than infections involving two or more spaces. Susceptibility to penicillin remains relatively high; therefore, penicillin can remain part of the armamentarium for treatment of odontogenic maxillofacial infections.
D
There is no consensus regarding antibiotic use, as evidenced by the variety of treatment protocols for treating odontogenic infections [6,7]. Different countries, even different hospitals, prescribe diverse antibiotics but the antibiotic treatments used most commonly include intravenous penicillin G, metronidazole, clindamycin, amoxicillin–clavulanic acid, or amoxicillin–sulbactam [5,8,9]. It is important to note that frequent antibiotic use may lead to antibiotic resistance, which in turn may result in treatment problems in the future.
During the last 10 y, there were no detailed studies about odontogenic maxillofacial infections in Lithuania. However, severe maxillofacial odontogenic infections are prevalent and are treated at three central specialized hospitals. The hospital-related cost for treating these severe infections is covered by medical insurance, thus patients do not have any out-of-pocket costs. After treatments are completed, all related documentation is archived centrally. This central accumulation information allows for the study of time trends in disease incidence as well as examination of risk factors and different aspects of disease management. Having this considerable amount of data available presents a unique opportunity for retrospective analysis, which has scientific value as well as clinical implications. The aim of the present study was to analyze treatment modalities and results in patients with severe odontogenic maxillofacial infections treated in the Department of Oral and Maxillofacial Surgery during a 10-y period.
Patients and Methods
The study was approved by the National Lithuanian Ethics Board (#158200-02-281-66). A total of 3,215 medical records were reviewed of maxillofacial infections from the Department of Oral and Maxillofacial Surgery from January 2003 to December 2012. Of these, 2,182 were maxillofacial infections of odontogenic origin. In Lithuania, hospitalization for dental treatment is reimbursed from public funds; this requires thorough documentation by the dental professionals involved. Consequently, the medical charts from the University Hospital comprised the information necessary for the present study. However, given the retrospective nature of the present study, there was no standardization regarding the prescription of antibiotics. General criteria for a hospital admission for patients with odontogenic maxillofacial infections were: Impaired function including limited mouth opening less than 40 mm, dysphagia, dyspnea, temperature greater than 38°C, soft tissue inflammation that spread into contiguous anatomic spaces, and serious general condition. All patients underwent surgical treatment such as drainage of underlying infiltrates and extraction of a causal tooth either under local or general anesthesia. In addition, the following data were also collected: Age, gender, presence of systemic diseases, smoking history, and treatment-related information such as time of first appointment, length of hospital stay, causal tooth, type of treatment provided, and microbiology including susceptibility testing to penicillin, metronidazole, cefasolin, and gentamicin. According to cited criteria 1,077 medical records were included in the study. The SPSS 20.0 software (IBM, Inc., Armonk, NY) was used for all statistical analyses, with a threshold for statistical significance set at p<0.05. Only the information available for all patients with acute odontogenic infections was included in the bivariate and multivariable analysis. The bivariate analysis (Spearman correlation) was used to explore the inter-relationships among the potential predictors for length of hospitalization such as the involvement of multiple teeth in such infections, multiple spaces infected, presence of systemic diseases, type of antibiotics used for treatment, change in treatment, and whether or not bacteria growth was observed.
The variables that were statistically significant in the bivariate analysis were selected for inclusion in the multivariable model. For the multivariable analysis, binary logistic regression analysis was chosen and the outcome was 7 d or less of hospitalization versus more than 1 wk of hospitalization. In order to explore the age-related effects on the length of hospitalization, regression analyses were used separately for those younger than 18 y, for the 18–64 y age group, and for patients 65 y or older. To enable direct comparisons of the predictors' role regarding the length of hospitalization in different age groups, the “enter” method was chosen for variable selection into the logistic regression models.
Results
Medical records of 1,077 patients with maxillofacial odontogenic infections were included in the study. Incidence of all odontogenic infection was 218±17 cases each year, with a maximum of 250 cases and minimum of 190 cases per year. Distribution of odontogenic maxillofacial infections during the 10-y period is shown in Figure 1. On average, maxillofacial odontogenic infections accounted for 7% of all Department of Oral and Maxillofacial Surgery patients who were hospitalized each year. Male-to-female ratio was 1.4:1. The mean age range was 37.0±16.9 y with the youngest patient being 4 y and the oldest 93 y old. Mean age of males was 38.8±16.3 y; mean age of females was 41.5±17.6 y. Sixty-three patients (5.8%) were younger than 18 y. The mean length of hospital stay was 8.7±5.5 d with the shortest treatment lasting 1 d and the longest treatment lasting 44 d; 37.2% of the patients were hospitalized for for more than 8 d. Only 15% of patients had a first appointment within the first 48 h after onset of symptoms; 85% delayed their visit; mean waiting time was 5.5 d. Approximately 40% of patients self-treated with mouth rinses and analgesics. All surgical procedures were performed within the first 6 h after hospital admittance and all patients received surgical treatment: An intra-oral incision was made in 45 cases (4.1%), extra-oral incisions were needed in 974 cases (90.4%), and an intra-oral incision combined with an extra-oral incision was made in 58 cases (5.3%). A causal tooth was removed in 85% of cases including 13% of cases in which teeth were removed prior to hospital admission. Only 2% of cases received an endodontic treatment after surgical incision. Systemic antibiotic therapy and nonsteroidal anti-inflammatory medications (e.g., nimesulide 100 mg twice daily) were used commonly and in 95% of cases systemic antibiotic therapy was combined with dexamethasone therapy. Intra-muscular dexamethasone was given over 48 h twice daily (4–12 mg according to patient's weight). Complications occurred in 1.8% (19) of cases: 11 patients had mediastinitis and had to be moved to the department of thoracic surgery, three patients had necrotizing fasciitis, four patients had major bleeding after an artery usuration in the post-operative period, and one patient had a cardiovascular complication.

Incidence of maxillofacial infection.
The most frequent causal tooth was a left second molar, which caused infections in 189 cases (17.5%). A single tooth as a cause of infection was diagnosed in 797 cases (74.0%).
Of all patients, 379 (36.1%) were smokers; 128 were females (33.7%) and 251 were males (66.2%). Thirty patients (2.7%) had diabetes mellitus, 59 (5.4%) had arterial hypertension, and 41(3.8%) had hepatitis B or C. Patients with diabetes mellitus had longer hospital stays than patients without systemic conditions (p<0.001). Inflammation spread most commonly into three or more anatomic spaces with the floor of the mouth involved in 401 cases (37.2%): In 35 cases (8.7%) inflammation had spread to a parapharyngeal space and in 37 cases (9.2%) infection reached the deep neck regions. The frequency of involvement of the different spaces is shown in Figure 2. Involvement of the floor of the mouth bilaterally (Ludwig angina) was found in 68 cases (6%). The main complaints according to the spaces involved included: Limited mouth opening in 376 cases (35.0%), dysphagia in 255 cases (23.6%), limited mouth opening and dysphagia in 112 cases (10.4%), with all patients reporting pain. When more than three anatomic spaces were involved the hospital stay was 18 d or more (p<0.001).
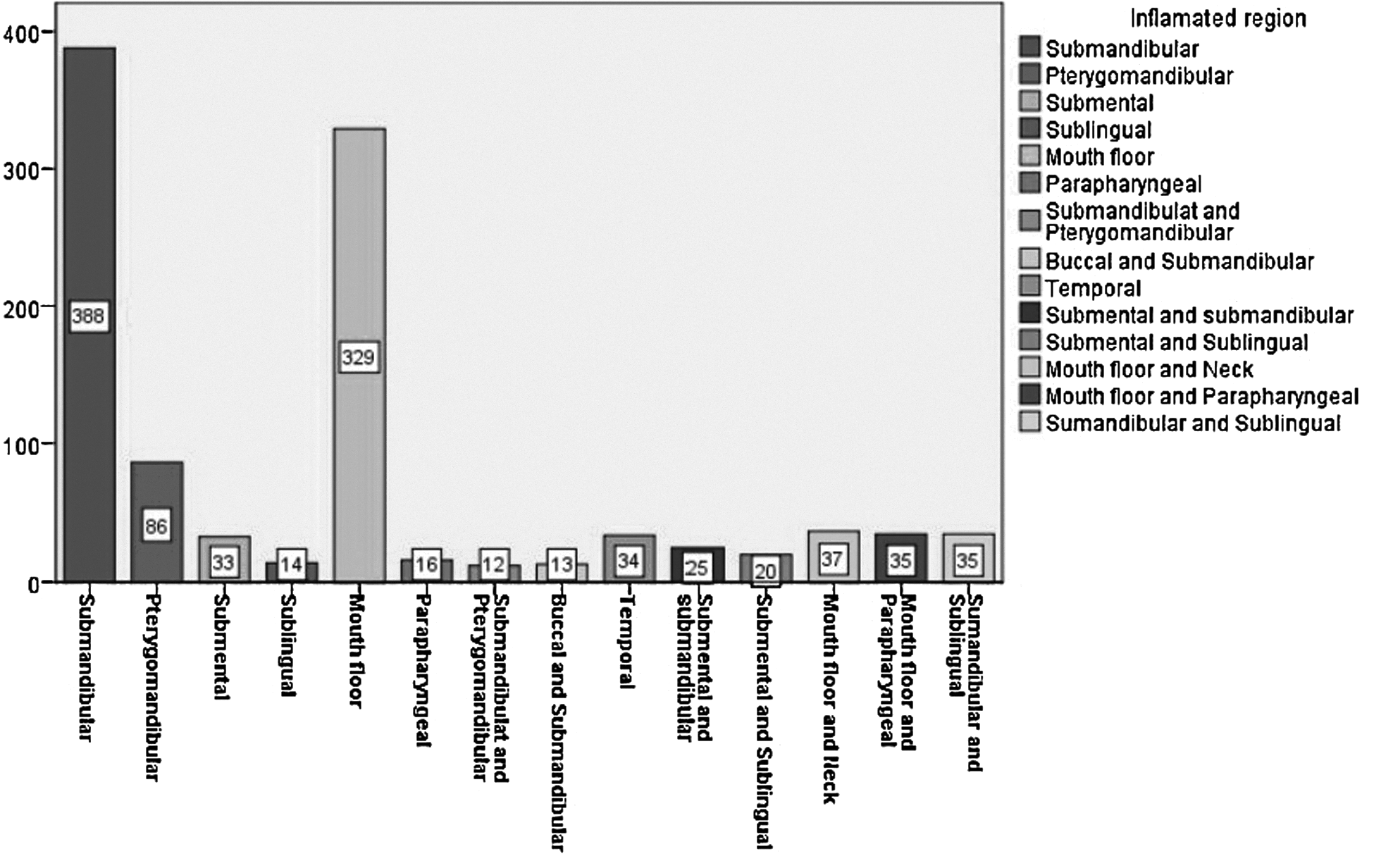
Different spaces involved in maxillofacial and neck odontogenic inflammations.
Table 1 presents the results of bivariate testing of associations among different variables to be further tested as predictors of the length of hospitalization. Results of three correlation analyses (Spearman correlation) are presented, one for each age group. Overall, all correlation coefficients were relatively low (<0.300).
Spearman's correlation coefficient (significance).
Prescription of penicillin group versus the prescription of non-penicillin group antibiotics or antibiotic combinations.
Empirical antibiotic treatment changed after microbiologic assessment.
In the group of patients younger than 18 y, only two statistically significant associations were observed: Between presence of systemic diseases and bacteria growth (p=0.045) and between bacteria growth and use of non-penicillin group antibiotics or antibiotic combinations (p=0.050). In the group of adult patients, four significant associations were identified: Between multiple space involvement and the prescription of non-penicillin group antibiotics or antibiotic combinations (p=0.001); between systemic diseases and multiple infected spaces (p=0.001); between the prescription of non-penicillin group antibiotics or antibiotic combinations and multiple infected spaces; and between a change in treatment and the prescription of non-penicillin group antibiotics or antibiotic combinations.
In order to examine which of the variables explained best or predict longer length of hospitalization, binary logistic regression analyses was performed (Table 2), where the binary outcome was 7 d or less of hospitalization versus more than 1 wk of hospitalization. The logistic regression model was significant (p<0.001) and the following significant predictors for the longer hospitalization were found: More severe infections as indicated by multiple tooth involvement and multiple infected spaces, prescription of non-penicillin group antibiotics or antibiotic combinations, and change in treatment (empiric anti-bacterial treatment changed after microbiologic assessment).
Binary logistic regression: outcome: ≤7 d vs. >7 d of hospitalization.
Predictor selection in all models: enter.
Model: (n=1,077):≤7 d (n=604) and >7 days (n=473).
Model summary: −2 log likelihood=1319, p<0.001, Nagelkerke R2=0.183.
Hosmer-Lemeshow test (χ2=13.37, df=7, p=0.064), c-statistic (AUC)=0.716.
Prescription of penicillin group versus the prescription of non-penicillin group antibiotics or antibiotic combinations.
Empirical antibiotic treatment changed after microbiologic assessment.
OR=odds ratio; CI=confidence interval; AUC=area under the curve.
Overall, the types of micro-organisms cultured were similar during the 10-y follow-up period. A total of 62 different micro-organisms were found. In 795 cases (73.8%) micro-organisms were cultured and in 282 cases (26.2%) no bacteria growth was found. In 569 cases (52.8%) one micro-organism was cultured, whereas in 202 cases (18.8%) there were two micro-organisms and in 24 cases (2.2%) three or more micro-organisms were cultured. The most common micro-organisms found were: Streptococcus haemolyticus in 341 (42.9%) samples, Gamma-hemolytic Streptococcus spp. anaerobic in 224 samples (30.0%), and coagulase negative Staphylococcus in 162 (20.4%) samples. Anaerobic strains such as Bacteroides and Prevotella were found in 104 samples and Streptococcus pyogenes were found in 101 (12.8%) samples.
Treatments according to the spaces involved are shown in Figure 3. Intravenous penicillin alone or in a combination with gentamicin or metronidazole was prescribed in 69% of cases, and a second-generation cephalosporins alone or in combination with gentamicin were prescribed in 24.7% of cases. Temporal trends of antibacterial treatment are shown in Figure 4. Treatment was changed because of microbiologic test results in 153 cases (14.2%); change was associated with a longer hospital stay (Fig. 5). The results of susceptibility testing to penicillin, celfasolin, gentamicin, and metronidazole are shown in Table 3. The tests showed that Streptococcus haemoliticus was resistant to penicilin in 56 cases (16.4%), γ Streptococcus spp. were resistant to penicilin in 46 cases (20.1%), and Staphylococcus epidermidis was resistant to penicillin in 72 (44.0%) cases. Gamma Streptococcus was resistant to metronidazole in 130 cases (58%) and Streptococcus haemoliticus was resistant to metronidazole in 86 (25.2%) cases.
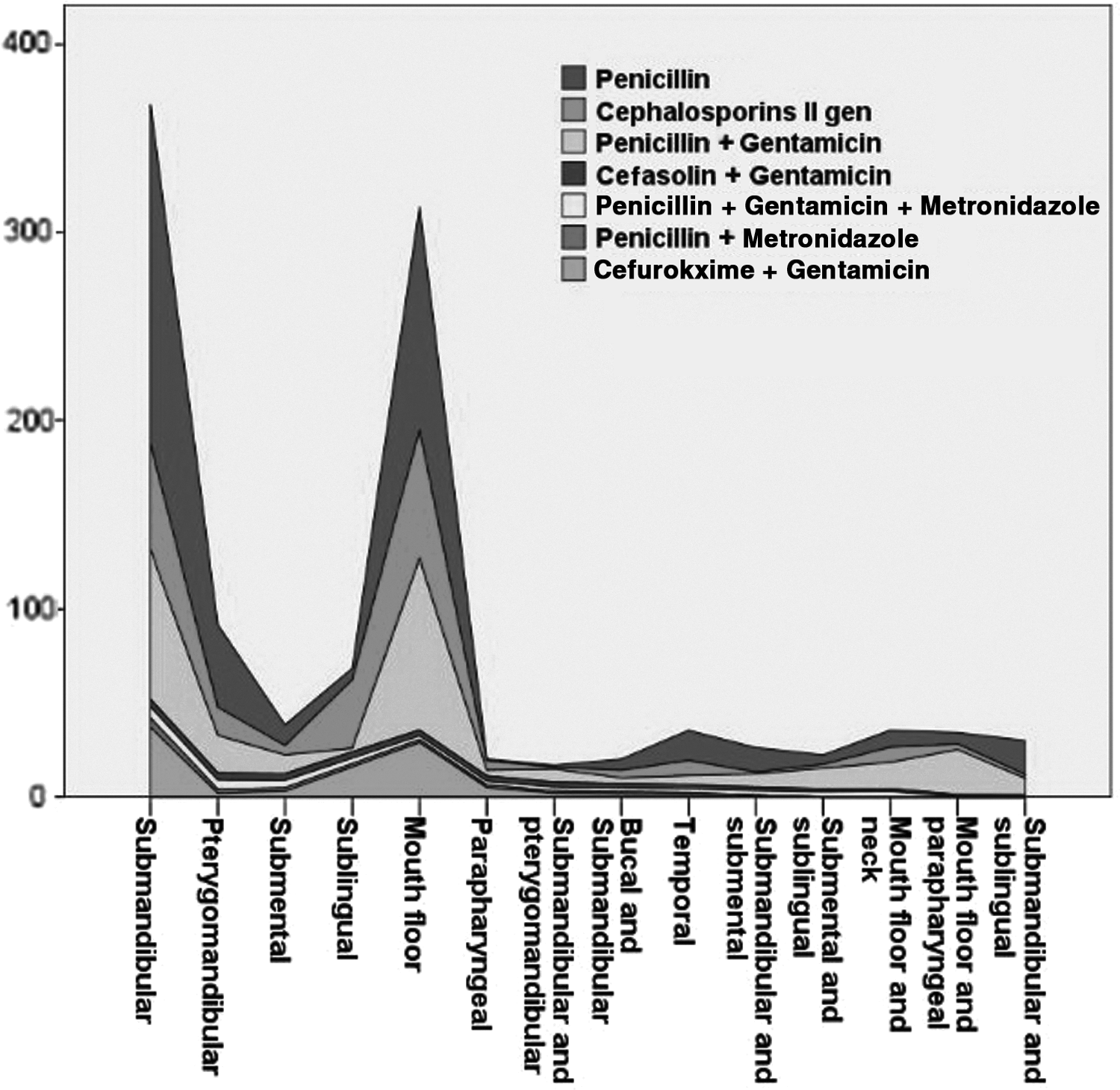
Antibiotic treatment according to the spaces involved.
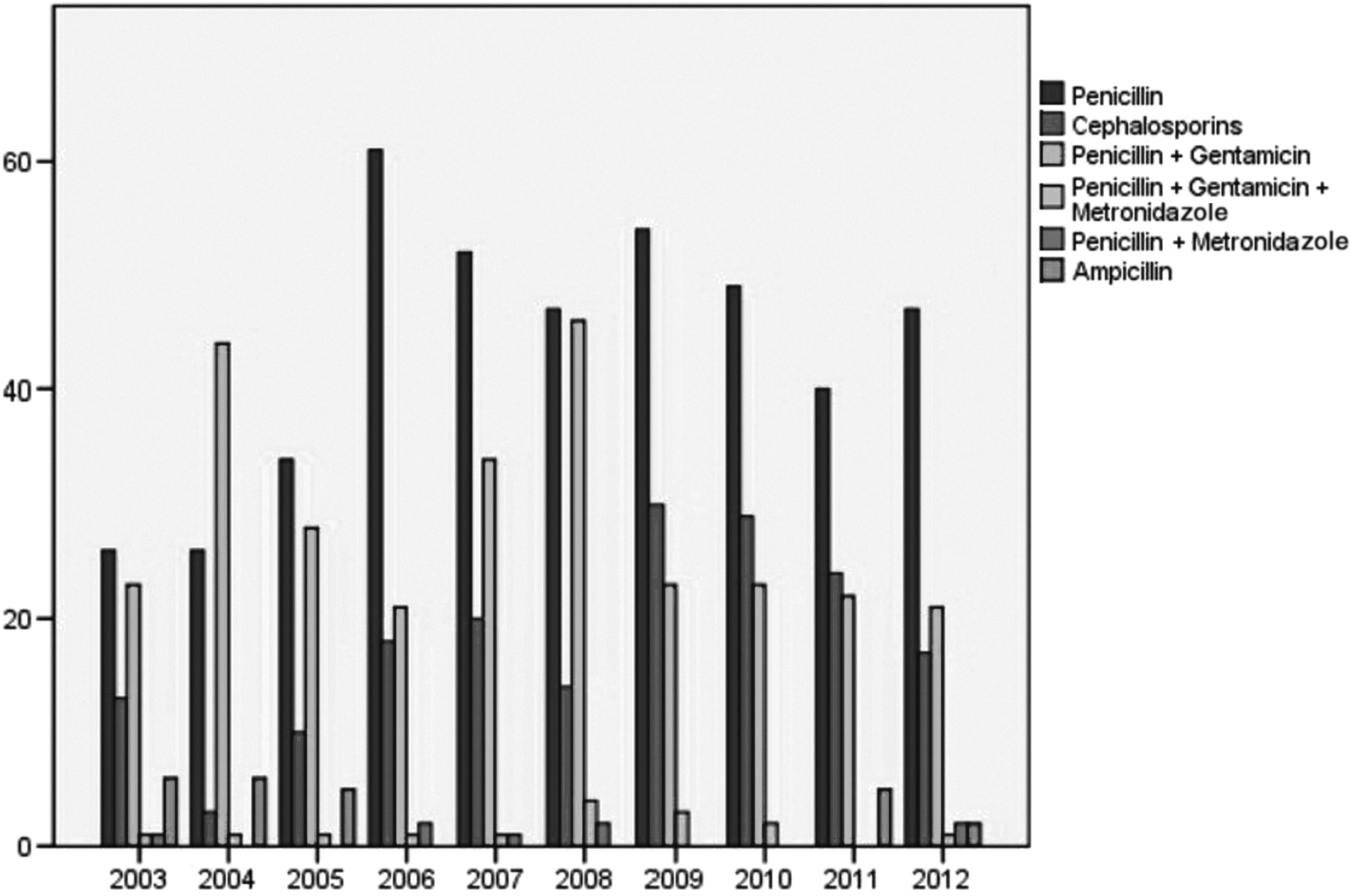
Time trends of antibiotic treatment during 2003–2012.

The length of hospital stay and antibiotic treatment change.
Discussion
Severe odontogenic infections constitute a substantial proportion of maxillofacial surgeons' clinical work, and these infections can be life-threatening if not treated adequately [9–13]. After treatments are completed, all related documentation is archived centrally. This accumulated information allows for the study of time trends in disease incidence as well as examination of risk factors and different aspects of disease management. The present retrospective analysis showed similar incidences of odontogenic infections throughout a 10-y follow-up period. In the present study, the main complications of maxillofacial infections were mediastinitis, airway obstruction, necrotizing fasciitis, and bleeding but the overall complication rate was relatively low (1.8%). It is important to consider that odontogenic infection-related complications vary among countries and range from 1.4% to 46.3% [5,14–17]. Early surgical drainage and adequate antimicrobial treatment remain the most effective treatment for maxillofacial infections [18]. The relatively low complication rate in Lithuania may be explained by timely professional care, in which surgical procedures are performed within the first 6 h after hospital admittance. Early diagnosis and timely referral to maxillofacial surgeons can save patients' lives but only 15% of patients first encounters was during the first 48 h after symptom onset. The vast majority delayed their presentation; mean waiting time was 5.5 days. Approximately 40% of our patients self-treated with mouth rinses and analgesics instead of seeking timely professional help. Delayed presentation, neglected dental pain in patients with maxillofacial infections, and self-treatment with mouth rinses, hot compresses, non-prescription drugs such as herbal medicaments, and analgesics are well-known concerns [3,4,18,16]. According to the present study, delayed presentation was associated with more serious infections, longer hospital stay, and need for antibacterial treatment change, with resulting higher treatment cost.
As in other studies, more males than females were affected by maxillofacial infections [2,5,11,15]. This pattern has been explained by the observation that men tend to care less about their oral health than women [18] and that males were twice as likely to have been smokers according to the present study. Smoking as a predisposing factor for oral health disorders is well documented [19]. The mean patient age was 37±16.9 y, which is in accordance with other studies in which patients with odontogenic infections had a mean age of 31–47 y [1,5,9,15]. No significant age difference between males and females was found. In the present study, 26.7% of patients were older than 50 years and 6.5% of patients were 18 y or younger. In 72 cases more than three spaces were involved and the patient's hospital stay was longer than 18 d. The multivariable analysis showed a number of potential predictors explaining the length of hospitalization and there seems to be multiple variables contributing to a longer hospitalization. Seemingly, a longer hospitalization relates to different direct and indirect indicators related to the severity of such infections such as involvement of more than one tooth, spread of infections into multiple spaces, need to prescribe non-penicillin group or antibiotic combinations, and treatment of infections that required a change in treatments. The change in treatment (different antibiotic/combination of antibiotics needed to be prescribed) was initiated after the microbiologic assessment of infections including the microbial susceptibility to antibiotics analysis.
The most frequently implicated teeth were posterior mandible segments with molars involved in 79.2% of cases. This finding is in agreement with other studies reporting that lower molars are most frequently found to be the causal teeth in maxillofacial infections. This predominance of lower molars in maxillofacial infections has been explained by deficient oral hygiene and the technical difficulty of restorative treatments in these posterior locations [8,18]. According to the present study, in 280 cases more than one tooth was a causal tooth. This is because of difficulty in identification of the main cause, inflammation, pain, and spreading of the infection. In those cases all teeth with periapical destruction were considered as possibly causal.
Our study also showed that infections involving one anatomic space were more common (57.1%). The majority of patients customarily delay a visit to the dentist despite complicated oral health status. Sometimes this delay becomes life-threatening: Patients present with high fever, decreased respiratory function, and mal nutrition due to limited mouth opening and impaired swallowing. Delayed presentation is a general reason for longer hospital stay, treatment and need for additional incisions. Infections involving several spaces and require immediate professional attention. Longer hospital stay was associated with multi-space infections.
Our microbiologic results identified a total of 62 different micro-organism species with Streptococcus haemoliticus and anaerobic Streptococcus being the most predominant bacteria and Bacteroides and Prevottela being rather common micro-organisms responsible for odontogenic infections. The streptococci and obligate anaerobes were predominant micro-organisms in primary infection and Enterococcus faecalis dominated in cases of secondary infection [20]. Any interpretation of microbiologic results should take into consideration that the microbiologic tests of the present study focused on identification of the most aggressive and abundant micro-organisms. In 282 cases (26.2%) with expressed purulent infection, no bacteria growth was found; this may be associated with incorrect sample technique or presence of a capricious micro-organisms in a sample. Different microbial patterns such as polymicrobial facultative anaerobes, viridans group streptococci, anaerobic streptococci Prevotella and Fusobacterium species were reported elsewhere [21]. Most importantly, there is no consensus about standard antibacterial treatment for odontogenic infections as evidenced by a variety of endodontic or surgical protocols including variations in antibiotic prescription [2,15,16,22,23]. The present study found that penicillin alone or in combination with gentamicin was chosen for treating severe odontogenic single-space infections, whereas second-generation cephalosporins or penicillin in combination with gentamicin were used for treating multi-space infections. Although other studies recommend metronidazole as additional antibiotic for treatment of anaerobic odontogenic infections [5,24], in the present study microbial susceptibility analysis showed the high resistance of Streptococcus haemoliticus (26.9%) and Bacteroides (35.6%) to metronidazole.
The trend of increasing micro-organism resistance to simple antibiotics, e.g., penicillin, has been reported in other studies [7,8,11]. Our main concern relates to self-treatment with diverse antibiotics as in our study: 22% of Lithuanians with severe odontogenic infections used antibiotics without consulting their physicians [25]. This finding is surprising because the Lithuanian Health Care policy has prohibited selling antibiotics without prescriptions for the last 8 y. Therefore, it is important to increase the public and professional knowledge about the hazardous use of antibiotics and the health implications this use may have.
Conclusions
Frequency of odontogenic widespread inflammations remains almost unchanged during a 10-y period. Single-space infections were more common (57.1%) than infections involving two or more spaces. The sensitivity of a micro-organism to penicillin remains high, therefore, penicillin can be the drug of first choice for treatment of odontogenic maxillofacial infections.
Footnotes
Author Disclosure Statement
No competing financial interests exist.