
Abstract
Abstract
Background:
We report an outbreak of surgical site infections due to genetically related strains of Streptococcus pyogenes in a cardiovascular surgery department.
Methods:
The practices that were possibly related to the outbreak were investigated through direct observation and interviews with staff by an infection control team. Surveillance sampling from patients, health-care workers, and environment were done for the investigation of the source. Pulsed-field gel electrophoresis was used to investigate a clonal relationship among the S. pyogenes isolates.
Results:
Four patients operated on in the cardiovascular surgery department developed surgical site infection due to S. pyogenes. Molecular characterization of S. pyogenes done by pulsed-field gel electrophoresis revealed the same strain.
Conclusions:
Although a definite source for the outbreak could not be identified, probably lack of adherence to hand hygiene practices during surgical dressings, contamination, and cross contamination led to this outbreak.
L
Patients and Methods
The outbreak was identified in the cardiovascular surgery department of Türkiye Yüksek İhtisas Education and Research Hospital. The cardiovascular surgery department consists of three wards with 134 beds. The affected patients were from ward II, which consisted of eight rooms with 25 beds. There were eight operating rooms in the cardiovascular surgery department. Working staff in each operating room consisted of two anesthesiologists, two nurses, one perfusionist, and three surgeons. The outbreak period was defined as from identification of the first case to 30 d after the last case. At the outbreak period, the distribution of working staff at ward II was five resident physicians, seven surgeons, eight nurses, and five housekeeping staff. The surgeons and resident doctors were also performing the surgical interventions. The study population was composed of patients who were present in the ward when the outbreak was identified. All of the patients with surgical site infection due to S. pyogenes were accepted as cases, and each of the case-patients was compared with four controls. Controls were selected randomly from patients on ward II during the outbreak period. The practices that were possibly related to the outbreak were investigated through direct observation and interviews with staff by infection control team.
Streptococcus pyogenes strains isolated from surgical site cultures were identified by VITEK II automated system GP panel (BioMerieux, Marcy I'Etoile, France). The minimum inhibitory concentration (MIC) of penicillin was detected by E-test. Pulsed-field gel electrophoresis was used to investigate clonal relationships among the S. pyogenes isolates.
Data were analyzed using software package STATA 11 (StataCorp, LP, College Station, TX). Logistic regression analysis was performed. A p value of<0.05 was considered statistically significant.
Results
Description of the outbreak
On November 2, 2011, it was noticed that S. pyogenes were yielded from the cultures of both pus and blood in a patient from the cardiovascular surgery department.
Index Case
A 77-year-old diabetic male patient who was living at a long-term care facility underwent coronary artery bypass grafting (CABG) via median sternotomy on October 10, 2011. On the seventh post-operative day, the patient left the hospital without discharge authorization. Later, he was located by police at the city garbage site and was taken to the long-term care facility. He was re-admitted to the hospital on October 31, 2011, with fever and purulent foul-smelling discharge from the sternal surgical site. On physical examination the temperature was 38.6°C, he had hypotension (80/50 mm Hg) and tachypnea (30 breaths/min). White blood cell count was 14,310/mm3 (88% neutrophils), C-reactive protein concentration (CRP) was 198 mg/L (normal:<5 mg/L), and erythrocyte sedimentation rate (ESR) was 74 mm/h. Ampicilin–sulbactam was started with a dose of 8 g/day. Streptococcus pyogenes was isolated from the culture of both pus and blood. The patient was evaluated for possible transmission routes and isolated because of concerns about potential patient-to-patient transmission. There was not any evidence of S. pyogenes infection in other patients operated on since October 10, 2011, so it was concluded that the patient was infected at the long-term care facility.
Secondary Cases
Case 1: A 61-year-old male patient who underwent four-vessel CABG via median sternotomy on October 26, 2011, was discharged on November 2, 2011, and was re-admitted with fever and purulent discharge from the leg incision for saphenous vein harvesting on November 12, 2011. Streptococcus pyogenes was isolated from the culture of the pus.
Case 2: A 36-year-old diabetic female patient who underwent CABG via median sternotomy on October 27, 2011, was discharged on November 1, 2011, and was re-admitted with fever, chest pain, and purulent discharge from the sternal surgical site on November 14, 2011. Streptococcus pyogenes was isolated from the culture of the pus.
Tertiary Case
Case 3: A 70-year-old male patient who underwent aortobifemoral bypass graft surgery on November 14, 2011, was discharged on November 18, 2011. The patient was re-admitted with purulent discharge from the surgical site on November 25, 2011. Streptococcus pyogenes was isolated from the culture of the pus.
All S. pyogenes strains were susceptible to penicillin with a MIC value of 0.064 mcg/mL. All patients were treated with ampicilin–sulbactam with a dose of 8 g/day and recovered fully.
Outbreak Investigation
Following identification of the S. pyogenes in two secondary cases, an outbreak investigation was begun, which included epidemiologic evaluation of patients and all health care workers (HCWs) involved with these patients' care. All case patients were isolated promptly in private rooms with proper skin barrier techniques. Surveillance sampling from patients, HCWs, and environment were done for investigation of the source. All HCWs were asked about sore throat, skin lesions, dermatitis, eczema, vaginitis, and pruritis ani. Throat cultures were obtained from all HCWs who were identified in the epidemiologic investigation including surgeons, nurses, and other staff working in the operating room and cardiovascular surgery ward. Throat and wound cultures were also obtained from patients sharing the same room with case patients. Skin culture was taken from one resident physician with dermatitis of the hands. No positive culture was identified in either HCWs or other patients. Environmental cultures were negative for S. pyogenes. Two weeks after the recognization of secondary cases, another case was defined. At this point interviews with staff and throat cultures were repeated.
Because these four cases of invasive S. pyogenes infection occurred so closely in time to one another, the isolates from each of the cases were sent to the Molecular Microbiology Research and Application Laboratory of Turkish National Public Health Agency (Ankara) for pulsed-field gel electrophoresis (PFGE).
Hypothesis about the Outbreak
Molecular characterization of S. pyogenes revealed that the four patients were infected with the same strain (Fig. 1). During the outbreak period, 68 patients received followup at ward II. Index case and case 2 were operated at operating room 4, case 1 at operating room 2, and case 3 at operating room 1. One of the members of the surgical team was the same in the index case and secondary case 1; the surgeons were different for the other two patients. The nursing staff and anesthesiologists were different for each operating room. Exposure to one resident physician (RP-A) was associated strongly with infection (odds ratio=25.4; 95% confidence interval 1.2–551.6, p=0.039). It was noticed that the change of surgical dressings were done subsequently in the index case and secondary cases by RP-A. Later on, it was realized that the change of surgical dressings were done subsequently between the secondary cases and tertiary case by RP-A also Physician. RP-A confessed that he usually did not wash his hands or use alcohol-based hand rub between instances of contact with patients, and declared that he did not wear gloves during the dressings because of allergic contact dermatitis caused by latex gloves, and he usually did surgical dressings with naked hands.
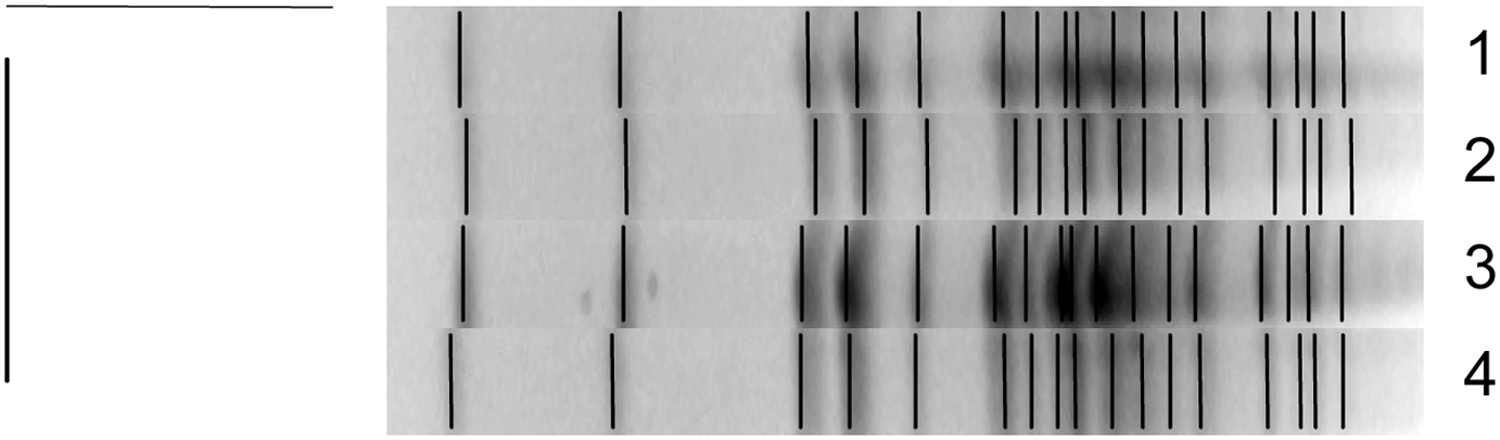
Pulsed-field gel electrophoresis profiles of Streptococcus pyogenes isolates after restriction with Spe I. Lane 1–4 corresponds to isolates of S. pyogenes from the wound cultures of the index case, cases 1, 2, and 3.
Discussion
Surgical site infections with S. pyogenes are observed rarely [8]. The throat and skin of the human host are the principal reservoirs for S. pyogenes [9]. Person-to-person spread of S. pyogenes occurs via respiratory droplets or by direct contact with throat secretions or dermal lesions in infected patients, so other patients, family members, HCWs, and the environment can play a role in transmission of the organism [10]. Surgical site infections may be acquired from the patient's pre-existing flora, during the operation itself, in the post-operative period on the ward, or later in the community. Hospital-acquired S. pyogenes infections can be transmitted via HCWs, the environment, or other patients. The HCWs most likely to have transmitted S. pyogenes are those with direct contact with the patient within seven days of the onset of the infection, which usually includes those present in the operating room and performing post-operative dressing changes [10]. Symptomatic HCWs account for 8.2% of outbreaks and colonized-asymptomatic HCWs for 34% [11]. When a suspected or confirmed outbreak of GAS has been identified, interventions to prevent further transmission and further cases should be put in place immediately. Healthcare workers must adhere to strict hand hygiene policy before and after contact with the patient or their environment, regardless of the use of gloves and other protective measures [8].
We reported an outbreak of surgical site infections due to genetically related strains of S. pyogenes in a cardiovascular surgery ward with low adherence to hand hygiene practices. We believe that the index case was probably infected at the long-term care facility, as GAS is an important cause of illness among elderly patients, particularly those individuals residing in long-term care facilities [12]. After the re-admission of the index case, lack of adherence to hand hygiene practices and cross-contamination probably led to this outbreak because basic infection control practices were not applied during surgical dressings. This hypothesis is supported by the disappearance of surgical site infections after reinforcement of hand hygiene techniques and procedures with the staff.
There are several limitations to our investigation. We could not identify definite source and definite transmission ways, although the identical isolates from the several patients suggests strongly the same source. Colonization and transmission of GAS from the anus, vagina, perineum, skin, and nose, is well documented without concurrent evidence of throat colonization [10,11]. Although we asked all HCWs about sore throat, skin lesions, dermatitis, eczema, vaginitis, and pruritis ani during the week prior to any of these cases, we only performed throat and skin screening of the HCWs and we were not able to identify definitively the original source. Another limitation is that, although molecular characterization by pulsed-field gel electrophoresis revealed that the patients were infected with the same S. pyogenes strain, we were not able to identify the M protein gene (emm) typing of the strains. The M protein has always been considered to be the major virulence factor of S. pyogenes infection. Therefore, most epidemiologic studies of GAS classify the organisms by M/emm type [2].
In conclusion, this outbreak highlights how epidemics may alert us to poor infection control practices. When a cluster of S. pyogenes cases has been identified, interventions to prevent further transmission and further cases should be put in place immediately. Adherence to infection control practices can prevent S. pyogenes outbreaks.
Footnotes
Author Disclosure Statement
No competing financial interests exist.