
Abstract
Abstract
Purpose:
To evaluate the effectiveness of prophylactic antibiotic therapy in reducing the incidence of post-ureteroscopic lithotripsy (URL) infections.
Methods:
A systemic search of PubMED® was performed to identify all randomized trials that compared the incidence of post-operative infections in patients without pre-operative urinary tract infections who underwent URL with and without a single dose of prophylactic antibiotics. The data were analyzed using Cochrane Collaboration Review Manager (RevMan®, version 5.2). The endpoints of the analysis were pyuria (>10 white blood cells/high-power field), bacteriuria (urine culture with bacteria >105 colony-forming units/mL), and febrile urinary tract infections (fUTIs), defined as a body temperature of >38°C with pyuria or meaningful bacteriuria within 1 wk after the operation.
Results:
In total, four trials enrolling 500 patients met the inclusion criteria and were subjected to meta-analysis. Prophylactic antibiotics significantly reduced post-URL pyuria (risk ratios [RR] 0.65; 95% confidence interval [CI] 0.51–0.82) and bacteriuria (RR 0.26; 95% CI 0.12–0.60; p=0.001). Patients who received prophylactic antibiotics tended to have lower rates of fUTI, although the difference was not statistically significant.
Conclusion:
Prophylactic antibiotic therapy can reduce the incidence of pyuria and bacteriuria after URL. However, because of the low incidence of post-URL fUTIs, we failed to show that a single dose of prophylactic antibiotics can reduce the rate of such infections significantly.
U
Pre-operative antibiotics play an important role in reducing surgical site infections in endourologic surgery such as transurethral resection of the prostate and percutaneous nephrolithotripsy (PCNL) [3]. However, the results of previous studies have been inconclusive with regard to whether prophylactic antibiotics reduce the rate of post-URL infections [1,4–7]. Given the small number of randomized trials, the guidelines on the regimen and duration of antibiotics differ among urologic associations. That is, the revised American Urological Association (AUA) best practice guidelines, published in 2014 [8], suggest that all patients undergoing URL should receive a prophylactic fluoroquinolone or trimethoprim-sulfamethoxazole. The updated European Association of Urology (EAU) guidelines, also published in 2014 [9] and based on a panel consensus, recommend that short-term antibiotic prophylaxis be administered. The Japanese Urological Association (JUA) guidelines [10] recommend that a first- or second-generation cephalosporin or fluoroquinolone be given for 24 to 72 h to all patients undergoing URL.
Large-scale randomized studies to determine the effectiveness of prophylactic antibiotics in reducing URL-related infections are lacking. Therefore, we systematically reviewed the literature and used meta-analysis to evaluate the effectiveness of prophylactic antibiotics in reducing post-URL infections, including pyuria, bacteriuria, and febrile urinary tract infections (fUTIs).
Patients and Methods
Review protocol
We used the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement to report our findings.
Search methods
Studies published from January 1990 to December 2013 were identified by computer searches of PubMed®, the Cochrane Central Register of Controlled Trials, and the Cochrane Database of Systematic Reviews. We used the following keywords: Ureteral stone, ureter stone, upper urinary tract stone, urolithiasis, antibiotic prophylaxis, prophylactic antibiotics, infectious complications, ureterocopic lithotripsy, and ureterorenoscopic lithotripsy. We then excluded studies of percutaneous nephrostomy, percutaneous nephrolithotripsy, and shockwave lithotripsy. To avoid missing important data, we performed a search for the following key words: Ureterorenoscopy or ureteroscopy and antibiotic prophylaxis or prophylactic antibiotics or infectious complication. We also searched the reference lists of the AUA, EAU, and JUA guidelines manually. Two authors (CWL and SJC) searched and reviewed the articles independently for inclusion. When discrepancies occurred, discussions were held with a third author (SSY) to reach a consensus.
The following criteria were used to filter studies for analysis: Randomized trials or comparative studies of patients who received either a single dose of intravenous or oral prophylactic antibiotics vs. a control group (without antibiotics) with follow-up data on post-operative urinalysis, urine culture, and fever. Patients with pre-operative urinary tract infections (UTIs) (pyuria or bacteriuria) were excluded. Studies without a control group also were excluded from our analysis.
Data extraction and quality assessment
We extracted the following information from each study: Population characteristics, study design, inclusion and exclusion criteria, experimental drug administration, follow-up period, and assessment of UTIs and fever episodes. The quality of the studies was evaluated by two authors. To assess the risk of bias in the trials that were included, we took account of the following aspects: Allocation concealment, blinding of participants and personnel, blinding of outcome assessment, completeness of outcome data, selective reporting, and random sequence generation.
Data synthesis and analysis
We compared the endpoints, namely pyuria, bacteriuria, and fUTIs, in patients who underwent URL with and without antibiotic therapy. Important bacteriuria was defined as >105 colony-forming units/mL and pyuria as >10 white blood cells/high-power field in follow-up urinalysis. An fUTI was defined as a body temperature of >38°C with pyuria or important bacteriuria within 1 wk after the operation.
All analyses were performed using Review Manager® statistical software (Version 5.2; Cochrane Collaboration, Oxford, United Kingdom). The meta-analysis was done with the fixed-effect method or with the random-effect method when statistically significant heterogeneity was present. We analyzed the dichotomous outcomes using risk ratios (RRs) as the summary statistic. Chi-square statistical tests (Q statistics) and the I2 test were used to test heterogeneity between trials. The number of patients that needed to be treated to prevent one infection was calculated from the RRs and the background risk of fUTIs in the control group.
Results
Characteristics of the trials
Figure 1 shows the flow chart of how the trials were selected. The initial search strategy yielded 399 abstracts. When we used other key words (Fig. 1), an additional 185 abstracts were identified. A total of 555 abstracts were included for evaluation after duplicates were removed. After excluding irrelevant abstracts, we retrieved the full text of 14 studies for evaluation. Case reports, review articles, and meta-analysis studies then were excluded. One retrospective comparative study evaluated patients with pre-operative UTIs and did not clearly define the prophylactic antibiotics that were used, so this study was excluded. In total, four randomized trials were analyzed. The demographic data of the patients in these trials are shown in Table 1, and the assessment of the quality of the studies is shown in Figure 2.

Flowchart for selection of trials
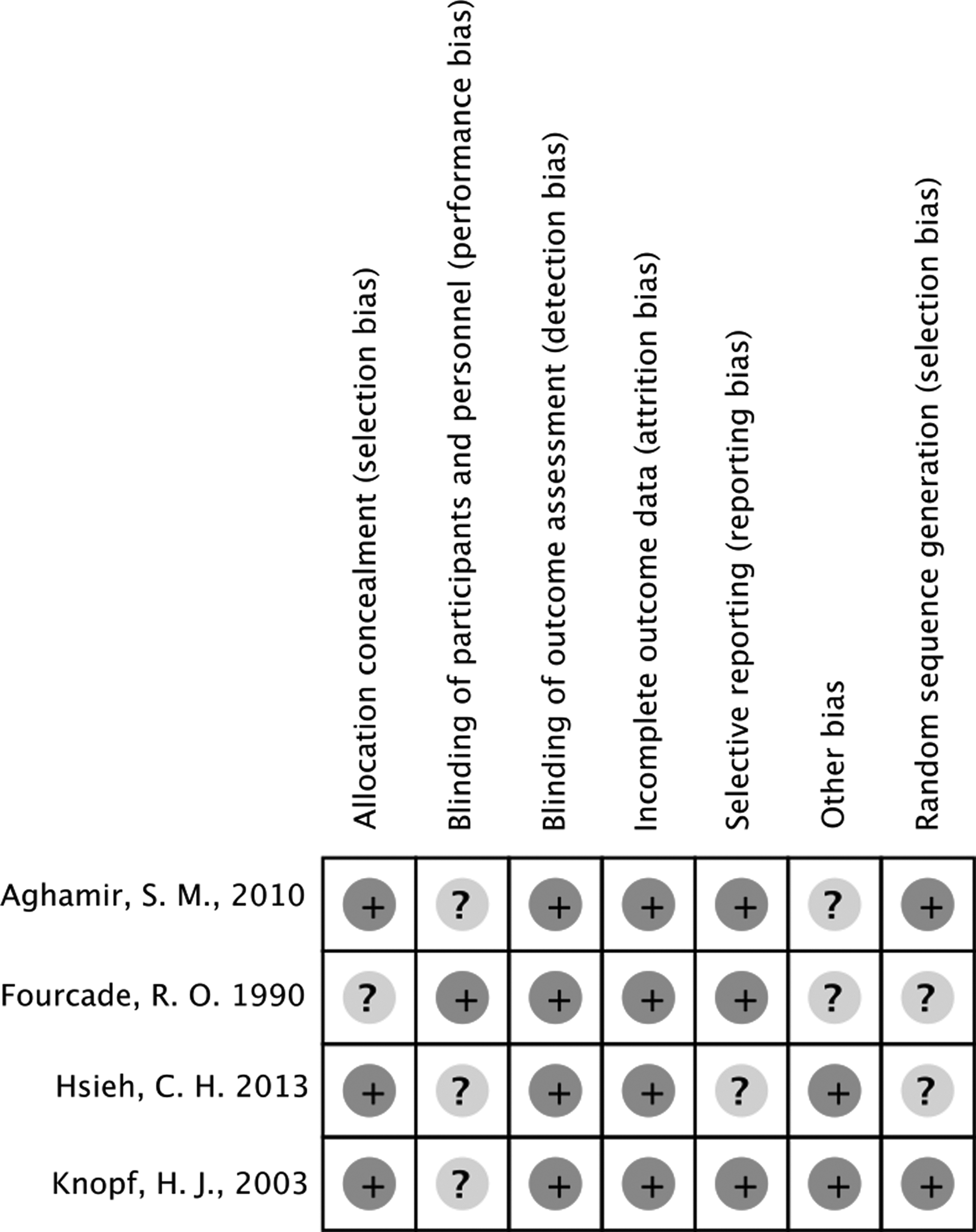
Risk of bias summary: Review authors' judgments about each risk of bias item for each study.
Incidence of post-operative infections
Incidence of pyuria
The results of post-URL pyuria were reported in only two studies. The incidence of pyuria in patients who received prophylactic antibiotics was 22.8% and 48.4% in the treatment groups and 49.1% and 64.7% in the placebo groups. Meta-analysis (Fig. 3A) showed that prophylactic antibiotics were associated with a significant reduction in the risk of post-URL pyuria compared with the control group (RR 0.65; 95% confidence interval [CI] 0.51–0.82; p=0.0005).
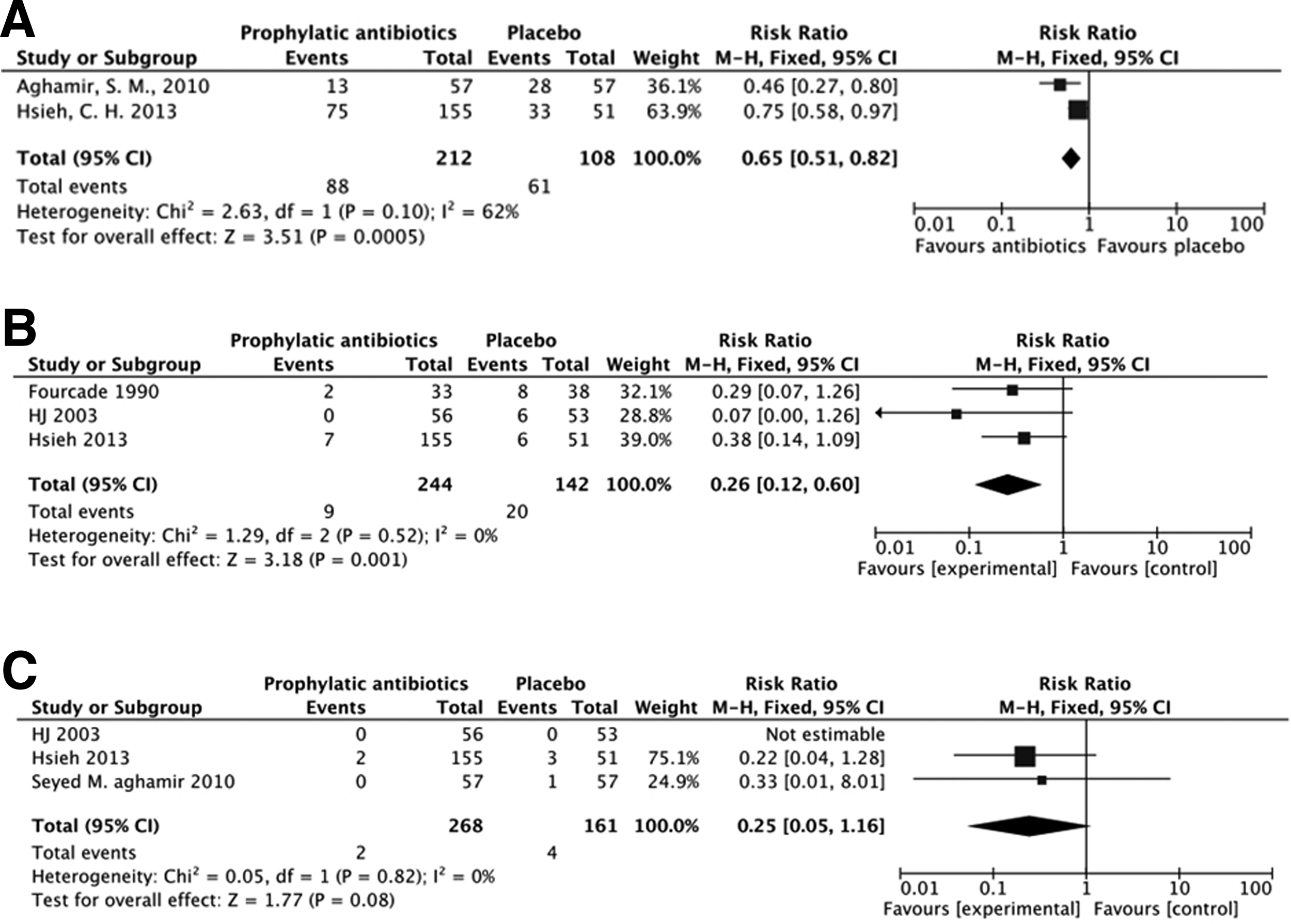
Forest plots of outcome comparisons: Antibiotic prophylaxis vs. no prophylaxis. (
Incidence of bacteriuria
Four trials reported results associated with bacteriuria. However, the report by Aghamir et al. [5] did not provide data specifically on bacteriuria. In addition, the study by Fourcade [4] enrolled patients undergoing either PCNL or URL. Therefore, we excluded the irrelevant data from both of these studies from analysis. Among the other trials, the reported rates of bacteriuria ranged from zero to 6% in the prophylactic antibiotic groups and 11.3% to 21.1% in the placebo groups. Meta-analysis showed that prophylactic antibiotics reduced the risk of post-URL bacteriuria significantly (RR 0.26; 95% CI 0.12–0.60; p=0.001) (Fig. 3B). The number of patients who had to be prophylaxed to prevent one case of bacteriuria was 9.6.
Incidence of febrile urinary tract infections
Three studies reported fUTIs. The study by Fourcade [4] enrolled patients undergoing PCNL or URL, and they did not include data on the rate of post-operative fever in the URL group. Therefore, we excluded this study from our meta-analysis for post-operative fUTIs. The incidence of post-URL fUTIs ranged from zero to 1.3% in the patients who received pre-operative antibiotic prophylaxis and zero to 5.9% in the placebo group. There was no statistically significant difference in the risk of post-URL fUTIs in patients who did and did not receive antibiotic prophylaxis (RR 0.25; 95% CI 0.05–1.16; p=0.08) (Fig. 3C). The number of patients that had to be administered prophylactic antibiotics to prevent one fUTI was 57.
Discussion
Ureteroscopic lithotripsy is a common clean-contaminated procedure for the treatment of ureteral stones. The role of prophylactic antibiotics in preventing surgical site infections has been well established in clean-contaminated surgery [7–12]. However, there is a lack of an accepted consensus on the routine use of prophylactic antibiotics in patients without pre-operative UTIs. According to the results of our meta-analysis of pooled data, prophylactic antibiotics can reduce post-URL pyuria and bacteriuria significantly (RR 0.65; 95% CI 0.51–0.82; p=0.0005 and RR 0.26; 95% CI 0.12–0.60, respectively). The results also suggested that prophylactic antibiotics may reduce post-URL fUTIs (RR 0.25; 95% CI 0.05–1.16; p=0.08). However, the difference was not statistically significant because the incidence of infection was low. The number of patients that had to receive single dose of prophylactic antibiotics to prevent one fUTI was 57. The rate of post-URL fUTIs was 2.5% in the non-prophylaxis group and 0.75% in the prophylaxis group. A randomized trial to detect a 1.75% reduction in the fUTI rate with an α of 0.05 and a β of 0.2 would require enrollment of 1,858 participants, which is difficult to achieve at a single center.
Through the systemic literature review and meta-analysis, we did not find enough evidence to support the current guidelines of the AUA, EAU, or JUA with regard to which type of prophylactic antibiotic is the optimum regimen to prevent post-URL UTIs cost-effectively. Only multicenter studies with a large number of participants would be able to elucidate this issue.
Our meta-analysis used three endpoints, namely pyuria, bacteriuria, and fUTI, to evaluate infections after URL. Prophylactic antibiotics reduced significantly the rate of post-URL pyuria and bacteriuria. Although pyuria may be a poor indicator of post-URL infections, it reflects the degree of inflammation. Bacteriuria is an important indicator of post-URL infections, so we included it in the analysis. The meta-analysis showed that the RR of bacteriuria was 0.26 (95% CI 0.26–0.60) with a necessary treatment number of approximately 10, although febrile or symptomatic UTI represented the ultimate arbiter of whether one should give antibiotic prophylaxis. Our meta-analysis did not show that prophylactic antibiotics can reduce rate of post-URL febrile UTI significantly. The reason was the low incidence of post-URL fUTI and the small number of participants. Despite the fact that there was no statistically significant decrease in post-URL fUTIs in our meta-analysis, the results showed a significantly lower post-URL bacteriuria rate and a trend toward a lower rate of post-URL fUTIs in the patients who received antibiotic prophylaxis. Therefore, we used surrogate endpoints for post-URL UTI and suggest that prophylactic antibiotics be used despite the lack of strong supporting evidence of their value.
We included four studies in our meta-analysis. All of the investigators administered the antibiotics within 60 min before the operation. Fourcade [4] compared cefotaxime with a placebo. Although this study enrolled patients who received either URL or PCNL, only the data with regard to URL were retrieved for our meta-analysis. However, Fourcade did not report separately the fUTIs in the patients who underwent URL. In addition, the author did not mention the reason for performing URL vs. PCNL in these patients, which may have caused bias. Knopf et al. [1] conducted a randomized study to compare oral levofloxacin (250 mg) with a placebo and clearly described post-URL pyuria, bacteriuria, and fever. Aghamir et al. [5] conducted a randomized trial that enrolled 114 patients and compared cefazolin (1 g) with a placebo. However, the results of post-URL fever and bacteriuria were not described clearly. There were two episodes of fever in the control group, which included one fUTI and one episode without evidence of UTI. Hsieh et al. [6] performed a randomized four-arm study to compare the effectiveness of different antibiotic regimens with control groups. Although the trial listed post-URL pyuria, bacteriuria, and fUTI, the number of patients enrolled was small; and therefore, the differences in antibiotic effects against post-URL fUTIs were not statistically significant.
Which antibiotic regimen is optimal to protect against infections, including a low incidence of resistance and low cost, has yet to be identified. The four studies in our analysis used different antibiotic regimens, including cefazolin (Aghamir et al. [5] and Hsieh et al. [6]), third-generation cephalosporins (cefotaxime by Fourcade [4] and ceftriaxone by Hsieh et al. [6]), and levofloxacin (Knopf et al. [1] and Hsieh el al. [6]); and the results of our meta-analysis cannot show which regimen is the best. Christiano et al. [13] compared oral ciprofloxacin with intravenous cefazolin and concluded that the drugs had equal effectiveness in preventing post-operative UTIs. Similarly, Hsieh et al. [6] did not show any significant difference between antibiotics. However, these two studies enrolled only small numbers of participants, so we cannot come to a definite conclusion.
There also exists controversy over the dosage and duration of antibiotic prophylaxis. Knopf et al. [1] used 250 mg of oral levofloxacin, which is a relatively low dose compared with current recommendations for this drug. Further studies are needed to elucidate whether the dose of levofloxacin (250 mg, 500 mg, or more) affects the utility of prophylaxis.
It is believed that the risk factors for post-URL infections include stone size, stone location, post-URL ureteral stenting, and the duration of surgery. However, conclusive evidence is still lacking for most of these factors [14]. The EAU guidelines published in 2010 [12] suggested that in patients with a proximal ureteral stone, a second- or third-generation cephalosporin should be given as prophylactic treatment because of the longer operative time and higher urinary-tract pressure during the procedure [2]. However, this suggestion was revised in the 2014 edition on the basis of panel discussions, which concluded that short-term antibiotic prophylaxis should be administered to all patients undergoing URL. In our meta-analysis, subgroup analysis was not performed because of the small amount of data. Only the study by Hsieh et al. [6] compared the rates of UTIs with different locations of ureteral stones. Although the efficacy of URL in the treatment of ureteral calculi has been demonstrated, the need for post-URL ureteral stenting is controversial. Two meta-analyses indicated that ureteral stenting did not lead to significant increases in post-ureterorenoscopy and post-URL UTIs [15,16]. We did not perform this subgroup analysis because of the limited amount of data available.
There were several limitations to this study. First, the studies we included spanned two decades, and this may have led to publication bias. The review by Grabe in 2004 [2] concluded that the rate of post-URL bacteriuria is less than 38%, and that the rate of fUTIs ranges from 4% to 25%. Overall, the four trials had a relatively lower post-operative infection rate than in a historical review. This may be secondary to patient selection, in that we enrolled only patients without pre-operative UTIs. Also, advances in ureterorenoscopic devices (the smaller ureterorenoscopes and introduction of the holmium yttrium-aluminum-garnet (Ho:YAG) laser could shorten the operation time and reduce the complication rate) [17], and improvement in sterilization methods [18,19] may reduce risks. Second, the number of patients enrolled was small, and the incidence of fUTIs after URL was low. Despite the fact that there was a trend toward a lower rate of post-URL fUTIs, the benefits of prophylactic antibiotics are not clear. More studies are needed to establish the efficacy of prophylactic antibiotics in reducing infections after URL. Lastly, subgroup analysis for other risk factors, including stone size, duration of surgery, and the location of the stones, was not performed because of the small amount of data available.
Conclusion
Our meta-analysis revealed that a single dose of prophylactic antibiotics is beneficial in reducing the rate of post-operative pyuria and bacteriuria, although there was no statistically significant benefit in reducing post-operative fUTIs. Prophylactic antibiotics may be helpful in patients undergoing URL even if they have sterile urine before surgery. However, large-scale multi-center studies are required to elucidate this issue.
Footnotes
Acknowledgment
The study is founded by Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation (TCRD-TPE-103-RT-7).
Author Disclosure Statement
No competing financial interests exist.