A 55-year-old Caucasian male with a history of tobacco dependence, deep vein thrombosis (DVT), and Factor V Leiden deficiency presented to the emergency department with left-sided chest pain. Physical examination was remarkable for mild respiratory wheezing on the left side. Pulse oximetry was normal. Cardiac etiology was ruled out. A chest radiograph revealed a mass-like opacity in the left lower lung field. Computed tomographic angiography (CTA) of the chest (Fig. 1A) was negative for pulmonary thromboembolism but characterized the opacity further as a possible pneumonia and cautioned that a malignant neoplasm could not be ruled out. The patient was treated for pneumonia with antibiotics and sent home. Two weeks after initial presentation, the patient had a follow-up CT scan of the chest (Fig. 1B) that revealed a persistent density measuring 3.0 cm×2.6 cm. A subsequent positron emission tomography (PET) scan (Figs. 1C and 1D) showed the mass to have increased metabolic activity (standardized uptake value [SUV] 5.8), again consistent with malignant neoplasm. The patient was diagnosed as having probable T2 N0, stage IB lung cancer. The patient underwent resection of the mass. Microscopic examination of the tissue revealed preliminary findings of necrotizing granulomatous inflammation (Figs. 2A and 2B). The findings were consistent with an infectious process versus vasculitis; malignant neoplasm was ruled out. Further evaluation revealed a well-demarcated concentric region of necrosis bordered by a granulomatous reaction and a peripheral ring of organizing pneumonia with a prominent lymphoplasmacytic infiltrate. Additionally, the sample revealed a central vessel containing a worm consistent with Dirofilaria (Figs. 2C and 2D).
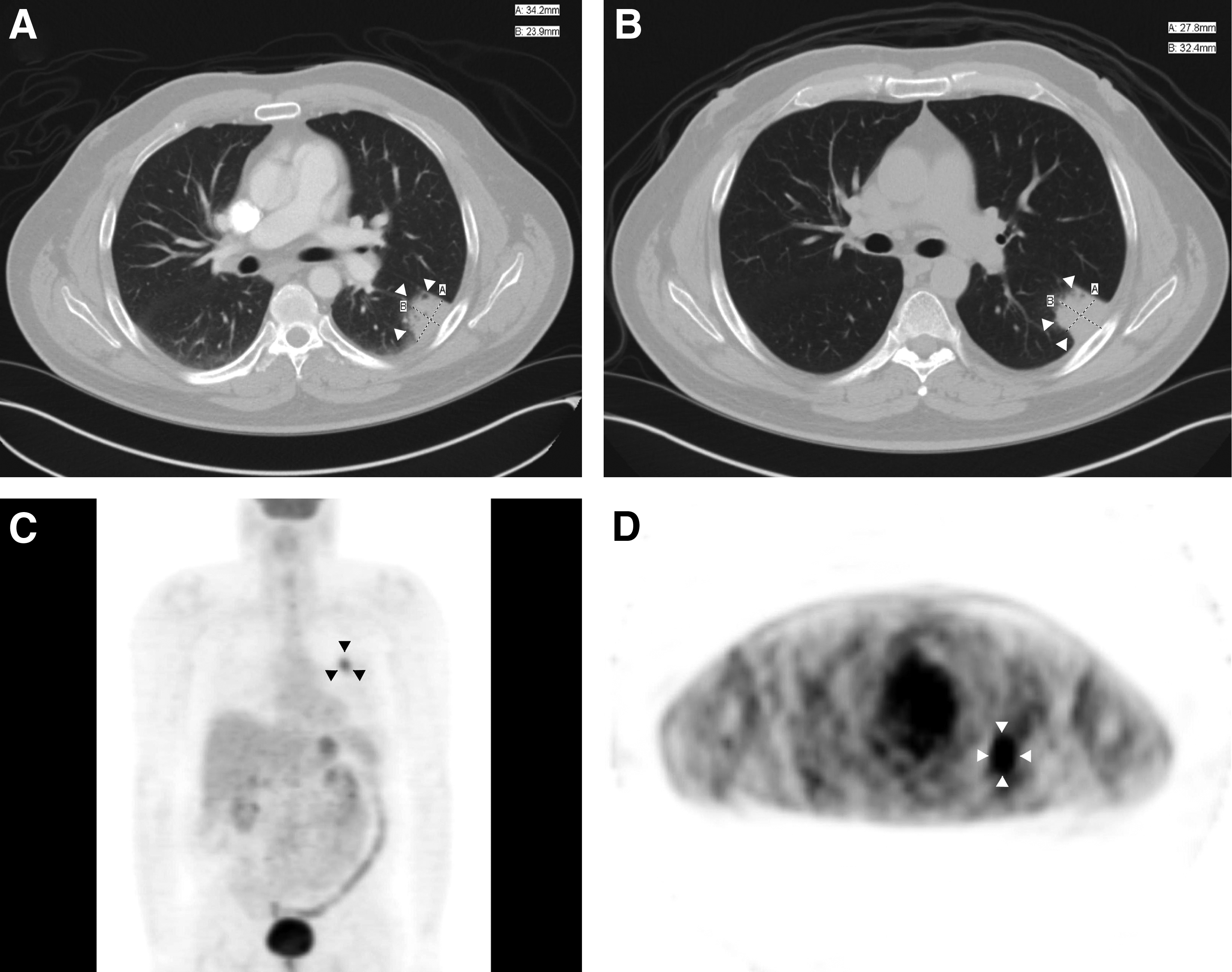
(A) Computed tomography angiography (CTA) of the chest viewed in lung window. The white arrowheads demarcate a 34.2×23.9 mm discrete solid mass. (B) Subsequent computed tomography (CT) of the chest viewed in lung window. The white arrowheads demarcate a persistent mass of roughly unchanged size compared with the image in (A). (C) Positron emission tomography (PET) of the chest in coronal view. The black arrowheads demarcate an area of increased metabolic activity consistent with malignant disease. Standardized uptake value score of 5.8. (D) PET of the chest presented in cross-sectional view. The mass is shown by the white arrowheads.
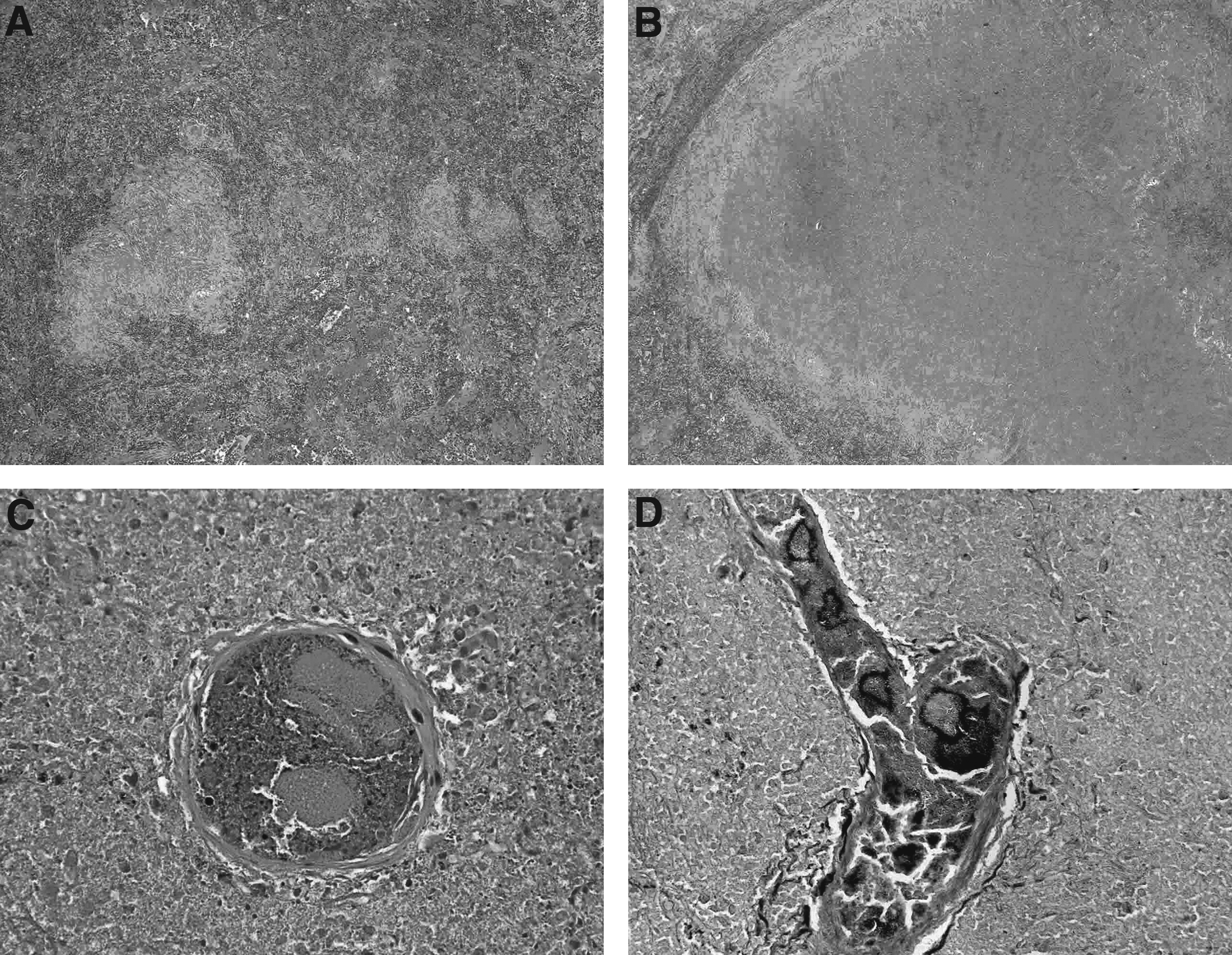
(A) Hematoxylin and eosin stain (magnification×20) showing a well-demarcated concentric region of necrosis bordered by granulomatous reaction and peripheral rim of organizing pneumonia. (B) Hematoxylin and eosin stain (magnification×40) showing lung parenchyma with granulomatous reaction, organizing pneumonia and lymphoplasmacytic infiltrate. (C) Hematoxylin and eosin stain (magnification×400) showing an arteriole that is filled with a degenerative worm consistent with Dirofilaria (degenerative eosinophilic cuticle and somatic musculature). There is associated thrombus and background necrosis. (D) Grocott methenamine silver (GMS) stain (magnification×200) showing a tangential section of branching arteriole filled with degenerative worm fragments on deeper concentrations consistent with Dirofilaria.
Dirofilaria is commonly known as heartworm and is identified most often in dogs. There have been more than 1,700 human cases reported worldwide but only a small number of these cases have been reported in the United States [1–3]. There are two species relevant to human beings: Dirofilaria immitis and Dirofilaria repens. Whereas D. repens presents most commonly with subcutaneous and ocular lesions, D. immitis presents most commonly as pulmonary nodules as observed in this case. The lifecycle of Dirofilaria in human beings has been described previously and consists of transfer of live organisms from dogs to humans via a mosquito vector [1]. Once in the human host, the organism travels to the heart where it usually dies and embolizes to the lung [4]. The radiographic findings are most often mistaken for malignant neoplasm. Increased metabolic activity on PET scan can complicate the diagnosis further as described in a similar case report [4] and as seen here. Laboratory tests are available to detect Dirofilaria in human beings including serology, cytology, and polymerase chain reaction [1], however, the practicality and cost of such testing could possibly result in delay of diagnosis the case of neoplasm. Unlike animals, the human immune response usually is sufficient to eradicate the organism and no further treatment is needed [1]. Nonetheless, because the lesions are most often mistaken for malignant disease, they are resected commonly.
In conclusion, Dirofilaria is a rare cause of pulmonary nodules in the United States but should be considered in the differential diagnosis. However, more research is needed to support the validity of using imaging and diagnostic testing to differentiate Dirofilaria from neoplastic disease and management should continue to be directed toward the latter [5].
References
1.
SimonF, Siles-LucasM, MorchonR, et al.Human and animal dirofilariasis: The emergence of a zoonotic mosaic. Clin Microbiol Rev, 2012; 25:507–544.