
Abstract
Abstract
Background:
The majority of aorto-caval fistulae occur spontaneously, either as a result of rupture of an existing atherosclerotic abdominal aortic aneurysm into the vena cava or secondary to iatrogenic injuries during peripheral angiography or surgery. Aorto-caval fistula from an infected aortic aneurysm is a rare scenario, but potentially lethal.
Methods:
Case report and review of the literature.
Case Report:
A 63-year-old female with diabetes mellitus and liver cirrhosis was admitted for intractable abdominal pain with rebound tenderness. A computed tomography scan demonstrated an abdominal aortic aneurysm and ill-defined peri-aortic fluid with air density and evidence of a fistula between the aorta and the inferior vena cava. Salmonella cholerasuis had been isolated from a blood culture at a previous admission. Urgent endovascular exclusion of the aorto-caval fistula was carried out, and the infra-renal abdominal aneurysm was repaired using a Cook Zenith TX2 aortic stent graft. She received parenteral ceftriaxone for four weeks.
Conclusions:
This case shows acceptable short-term results after endovascular repair of a Salmonella-infected aorto-caval fistula.
T
Case Report
A 63-year-old female with diabetes mellitus and hepatic cirrhosis was brought to our emergency department for intractable abdominal pain with rebound tenderness. Fever and chills had been treated in another hospital one week earlier. Physical examination revealed blood pressure of 80/40 mm Hg, heart rate of 110 beats/min, and marked pitting edema of both lower extremities extending posteriorly to the pre-sacral region. Laboratory findings consisted of anemia with leukocytosis of 12,200 cells/mm3, C-reactive protein concentration of 23.4 mg/dL.
An abdominal computed tomography scan demonstrated an aortic aneurysm and ill-defined peri-aortic fluid with air density (Figs. 1A, B) Some contrast opacificated the inferior vena cava during the arterial phase, which indicated a fistula between the aorta and inferior vena cava (Fig. 1C).
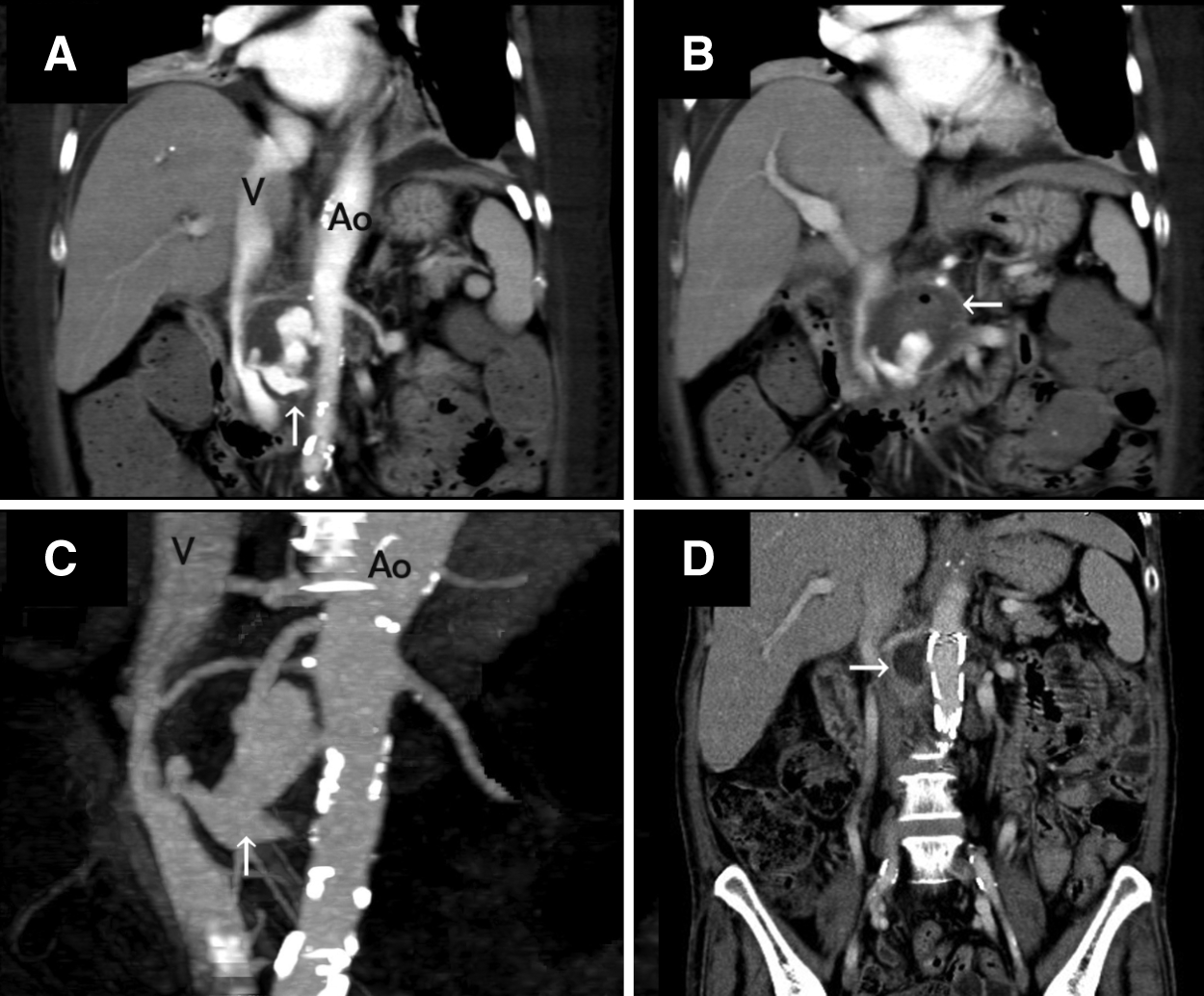
Images of patient with aorto-caval fistula and abdominal aortic aneurysm. (
Salmonella cholerasuis was recovered from a blood culture obtained during a previous admission. Urgent endovascular exclusion of the aorto-caval fistula was carried out via an open bifemoral approach because of the worsening abdominal pain. The infra-renal abdominal aneurysm was seen, along with a large aortocaval fistula, and was repaired using a Cook Zenith (Coole Medical, Bloomington, IN) TX2 aortic stent graft (22 mm in diameter and 80 mm in length). Completion angiography revealed an adequate seal of the aneurysm with endovascular occlusion of the aorto-caval fistula and no evidence of leakage after temporal dilation by a Coda® balloon (Coole Medical). She received parenteral ceftriaxone for four weeks and then was discharged uneventfully without oral antibiotics. Follow-up CT scanning at four wks showed good exclusion of the fistula (Fig. 1D).
Discussion
Aorto-caval fistula resulting from ruptured abdominal aortic aneurysm was first described by Syme in 1831. The present incidence ranges from 0.2% to 6% of all ruptured aortic aneurysms [1,2]. The classic triad of abdominal pain, pulsatile abdominal mass, and abdominal bruit is found in only 50% to 80% of cases [3]. As the aorto-caval fistula in our patient resulted from a ruptured, infected aortic aneurysm, producing a constellation of infection, and abdominal, cardiac, renal, and lower-extremity manifestations, the diagnosis could have been missed, resulting in delayed treatment. This is a common problem with such lesions.
Endovascular repair of an aorto-caval fistula has been a therapeutic option since 1998 [4]. However, the only case series describing endovascular treatment of aorto-caval fistulae showed a complicated clinical picture, with a mortality rate of 75% [5]. Among the patients in that series who died, all had delayed diagnosis, resulting in the poor response to the endovascular aortic repair.
Aorto-caval fistula caused by a Salmonella-infected abdominal aortic aneurysm is rare. As an increasing number of successful endovascular repairs of infected aortic aneurysms are being reported in the literature, our case illustrates the acceptable short-term results of endovascular repair for treating Salmonella-infected aorto-caval fistula, which could be a reasonable option in this difficult clinical entity.
Footnotes
Author Disclosure Statement
No competing financial interests exist.