
Abstract
Abstract
Background:
Chronic adenoid infection by β-lactam-resistant Haemophilus influenzae type b (Hib) and biofilm formation contribute to adenoid hyperplasia. Middle ear disease consequently remains a critical issue in the pediatric population. The aim of this study was to investigate the correlation of Hib biofilm formation with middle ear effusion with adenoid hyperplasia (MEE-AH) and with pediatric obstructive sleep apnea (OSA).
Methods:
A total of 384 patients with adenoidectomy from January 2008 to December 2012 were recruited in this investigation. Thirty-two patients (14 female and 18 male; age 4–13 years) who obtained routine adenoidectomy surgery had Hib-positive cultures were enrolled in a retrospective manner. By using polysomnography, 18 patients were diagnosed as having MEE-AH with chronic adenotonsillitis, and 14 patients were diagnosed as having pediatric OSA. The results of the Hib biofilm, antibiotic resistance profiles, and scanning electron microscopy observation, which correlated with the clinical diagnosis, were analyzed by the chi-square test and Fisher exact test.
Results:
Biofilm formation by Hib was significantly present in the patients with MEE-AH rather than patients with OSA. β-lactam-sensitive Hib were resistant to augmentin because of the adenoid biofilm formation. However, this finding was uncommon in the pediatric OSA group.
Conclusions:
Properly treating β-lactam-sensitive Hib infection may be an important issue in reducing MEE-AH and adenoid vegetation in the pediatric population. Further research is warranted to elucidate the association of Hib-related biofilm formation with treatment failure and the need to consider earlier surgical intervention.
A
Biofilms are structured communities of bacterial cells embedded in an extracellular polymeric substance comprising nucleic acids, proteins, and polysaccharides [5]. The architecture of biofilms may be highly resistant to host defense systems and have the ability to adhere to a mucosal surface in a host with impaired immune responses [6]. Bacterial biofilm formation may have an important role in many otolaryngologic infections (e.g., otitis media or otitis media with effusion, rhinosinusitis, and adenoiditis or tonsillitis), thereby resulting in persistent and difficult eradication of infections [1].
Haemophilus influenzae is an important pathogen that infects the upper respiratory tract of patients and may cause human illness. Six capsular types (a–f) influence the pathogenicity of this bacteria; H. influenzae type b (Hib) is a major cause of pneumonia, meningitis, and severe infections in children [7,8]. Previous studies report that otolaryngologic infection by H. influenzae may become more difficult to treat with antibiotic therapy [9,10]. There is evidence that otolaryngologic infections that are recalcitrant to antibiotic therapy are associated with bacterial biofilm formation [1,6,11].
H. influenzae infection is more prevalent in pediatric adenoiditis and middle ear infection problems, and it causes antibiotic resistance that leads to chronic upper airway infection and otitis media [8,12,13]. Much is known concerning antimicrobial resistance mechanisms, but the inherent resistance of a H. influenzae biofilm to antimicrobial agents needs further investigation. In this study, we investigated the correlation between Hib biofilm formation and antimicrobial resistance to the β-lactam drugs. The results of this study may offer clinicians a proper, quick, and efficient treatment for pediatric otitis media and adenoiditis condition.
Patients and Methods
Patient collection and tissue preparation
The adenoid tissues were obtained through routine adenoidectomy from patients with middle ear effusion with adenoid hyperplasia (MEE-AH) and obstructive sleep apnea (OSA) proved by polysomnography with major complaint of snoring, which was noted by parents and with affected daytime behavior problems or altered attention span. The patients (n=384) with OSA were checked to rule out middle ear infections or otolaryngologic infections and their apnea hypopnea index (AHI) more than five per hour during the period from January 2008 to December 2012 at China Medical University Hospital, Taichung, Taiwan. To analyze the correlation between Hib infection patterns and different disease entities, we excluded patients with combined OSA and MEE. The ear and sinuses of patients with OSA were examined, and none of these patients had signs of infection, such as fever, ear pain, sore throat, purulent rhinorrhea or otorrhea.
The tissues were prepared and streaked over Tryptic soy agar (Becton Dickinson, Franklin Lakes, NJ) and incubated at 37°C for 18–24 h. The microorganisms were identified using a BD Phoenix™ Automated Microbiology System (Becton Dickinson) as described previously [14]. This study was approved by the Ethic Committee of the China Medical University Hospital, Taichung, Taiwan (DMR101-IRB1-135).
Bacterial culture and antimicrobial susceptibility
All Hib isolates were routinely isolated and cultured in chocolate agar plates (Becton Dickinson). The antimicrobial susceptibility of the Hib isolates were determined by the BD Phoenix™ Automated Microbiology System as described previously [15].
Immunofluorescence analysis
The bacterial biofilm formation was analyzed based on bacterial size, morphology, and extracellular glycocalyx by using confocal laser scanning microscopic images as described previously [14]. Briefly, H. influenzae isolates were incubated at 37°C for 48 h with shaking at 150 rpm. The samples were fixed with 5% formaldehyde (Sigma-Aldrich, St Louis, MO) for 10 min and labeled with 15 mcmol/L propidium iodide (PI) (Sigma-Aldrich). The bacterial extracellular polysaccharide glycocalyx was stained with 50 mg/L fluorescein isothiocyanate–conjugated concanavalin A (ConA-FITC; Invitrogen, Grand Island, NY). Fluorescent images were observed and analyzed by confocal laser scanning microscope (CLSM) (Zeiss LSM 510; Zeiss, Göttingen,Germany).
Scanning electron microscopy
The morphology of microbial colonies on the surface was examined using scanning electron microscopy (SEM) as described previously [14]. Briefly, the specimens were fixed in 2.5% glutaraldehyde for 2 d at 4°C and then washed twice in PBS, followed by post-fixing treating in PBS with 1% osmium tetroxide for 1 h. The samples were dehydrated and dried by the critical point drying method (Critical Point Dryer; Hitachi, Tokyo, Japan), and then coated with gold (15-nm particles) by an ion coater (Giko Engineering Co., Tokyo, Japan). The prepared samples were examined by a scanning electron microscope (Hitachi, Japan).
Biofilm formation assay and biofilm criteria
Bacterial isolates were grown in fresh Brain Heart Infusion (BHI, Becton Dickinson) broth at 37°C for 18 h. After bacterial suspensions being diluted 100-fold with BHI, samples were seeded in 96-well plates and incubated at 37°C by shaking at 220 rpm for 18 h. The culture supernatants were removed, and the attached biofilms were stained with crystal violet for 15 min. Crystal violet dissolved in 95% ethanol, samples were measured by ELISA reader (Molecular Devices, MenloPark, CA) at 570 nm. In vitro biofilm formation activity was evaluated based on bacterial size, morphology, and extracellular glycocalyx using CLSM and SEM images, and crystal violet staining as described previously [14].
Statistical analysis
The relation of between-group comparisons was performed using the chi-square with Fisher exact test by SPSS 17.0 edition. p<0.01 was considered statistically significant.
Results
Demography of the patients
This study comprised of 384 patients with adenoidectomy. Thirty-four patients (14 females and 20 males) aged from 4 to 13 years with adenoid hyperplasia who obtained routine adenoidectomy surgery and tested positive for Hib were enrolled in this study. The incidence of Hib colonization was 8.9% (34/384). Two patients had Streptococcus pneumoniae and Escherichia coli coinfection, whereas the others harbored a single strain of Hib. Two patients with MEE combined with OSA were excluded from this study. Fourteen patients (mean age, 6.9±1.6 years) were diagnosed with pediatric OSA (Table 1), which was proven by polysomnography with apnea-hypopnea index (AHI) more than five per hour and had daytime sleepiness and snoring. The remaining 18 patients (mean age 7.4±2.3 years) had persistent MEE-AH with positive history of acute otitis media were prescribed amoxicillin-clavulanate for 10–14 d for treating the infection. Additional cefuroxime axetil (30 mg/kg/day, twice daily) was administered to patients with a poor clinical response for 7 d. None of them had diabetes mellitus or was on steroids before the surgical treatment.
Each subject number identifies a unique patient
Gender: M=male; F=female.
β-lactamase-positive Hib isolates.
Antimicrobial agent susceptibility: S=susceptible; R=resistance
Determination by bacterial biofilm assays including crystal violet staining, SEM and CLSM observations. +=presence; −=absence.
MEE-AH=middle ear effusion with adenoid hyperplasia; OSA=pediatric obstructive sleep apnea.
Biofilm formation assay
Biofilm formation activity was determined for all Hib isolates by using crystal violet staining and by using CLSM and SEM methods. Hib isolates from adenoid tissues were stained with PI and ConA-FITC to distinguish between bacterial cells and extracellular polysaccharide glycocalyx, respectively. After a 24-h incubation, CLSM images revealed an accumulation of Hib isolates (red) and extracellular polysaccharide glycocalyx (green) (Fig. 1). The biofilm formation activity (as evidenced by ConA-FITC) was much greater in Hib isolate (no. 14) than in the non-biofilm-forming isolate (no. 5) (Fig. 1). Bacterial colonies on the adenoid surface were then visualized by SEM. In patients with the non-biofilm-forming Hib isolate (no. 5), the bacterial colonies showed no promising biofilm structures (Fig. 2A). By contrast, SEM images of the biofilm-forming Hib isolate (no. 14) in the adenoid tissue revealed interconnected bacterial clusters with extracellular polysaccharide on the mucosal surface crypts (Fig. 2B).
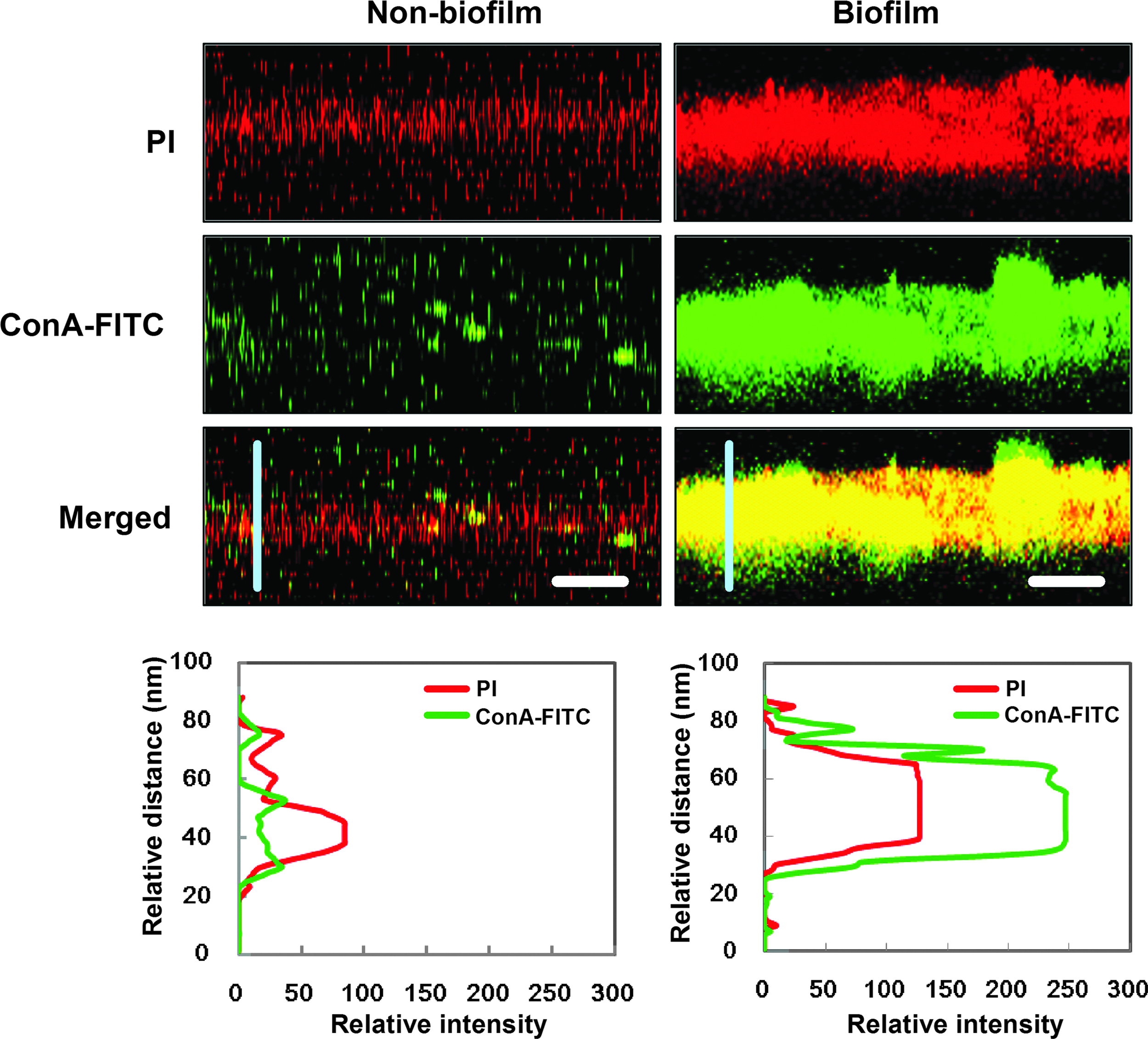
Biofilm formation of Hib isolates, as observed by confocal laser scanning microscope. The Hib isolates and extracellular polysaccharide glycocalyx are stained with PI (red) and ConA-FITC (green), respectively. The co-localization of bacteria and glycocalyx is indicated in yellow in the merged images. Left panel subject no. 5; right panel subject no. 14. A large amount of glycocalyx organized in clusters (merged, right panel) shows the biofilm formation by the Hib isolates. The scale bars represent 5 mcm. The distribution of fluorescence intensity for Hib (red) and extracellular glycocalyx (green) signals across the vertical blue lines were calculated and presented as line intensity histograms in the lower panels. ConA-FITC=fluorescein isothiocyanate-conjugated concanavalin A; PI=propidium iodide. Color image is available online at www.liebertpub.com/sur

Scanning electron microscope images of the mucosal surface of the adenoid tissues.
Association of Hib biofilm formation with MEE-AH
We compared the biofilm-forming activity of Hib isolated from patients with MEE-AH and from patients with OSA. As Table 2 shows, no Hib isolate from the OSA patients harbored biofilm-forming activity. However, in the MEE-AH patients, 44.4% (8 of 18) of the Hib isolates had biofilm-forming activity (p<0.01). This result indicated that Hib isolated from the adenoid tissues of patients with MEE-AH showed a greater rate of biofilm detection, compared with pediatric OSA patients.
MEE-AH=middle ear effusion with adenoid hyperplasia; OSA=obstructive sleep apnea
β-lactamase-negative Hib is correlated with biofilm formation
The antibiotic susceptibility of Hib isolates against chloramphenicol, ampicillin, and cefotaxime was further evaluated to determine whether bacterial biofilm formation affects antimicrobial resistance. As shown in Supplementary Table 1, Hib isolates—whether resistant or susceptible to chloramphenicol and cefotaxime—showed no difference in the concentration of biofilm-forming activity. By contrast, ampicillin-resistant Hib isolates had lower biofilm-forming activity (25.0%), compared with ampicillin-susceptible isolates (75.0%). In accordance with the finding of antimicrobial susceptibility to ampicillin, there was also a lower concentration of biofilm-forming activity in Hib isolates producing β-lactamase, compared with Hib isolates lacking β-lactamase (P<0.01). These results reveal that the β-lactamase-positive Hib isolates form significantly fewer biofilm-forming colonies.
Discussion
Pediatric chronic adenoiditis often cause chronic upper airway mucosal infection and easily leads to repeated episodes of sinusitis, tonsillitis, and otitis media with effusion [16–19]. Several studies confirm that chronic adenoiditis and MEE is caused by biofilm formation deep in the core of adenoid tissues, and that obstruction of the Eustachian tube may lead to MEE [12,19]. Previous studies indicate that adenoid biofilm formation by bacteria may cause adenoid hyperplasia and repeated acute otitis media and less biofilm-forming was found in patients with OSA [3,4]. In the adenoid tissues, biofilms are formed by several bacteria such as Staphylococcus aureus, S. pneumoniae, Pseudomonas aeruginosa, and H. influenzae [14,20–22]. Biofilm formation is a possible cause of pediatric adenoiditis and MEE [23]; however, there were few reports concerning the Hib biofilm to the MEE-AH. Additionally, the mechanism and the cause of pediatric chronic adenoiditis by Hib are not well understood.
In recent years, isolates resistant to antibiotics such as ampicillin and the β-lactam antibiotics are more prevalent in many cases of chronic adenoiditis, including MEE-AH and chronic rhinosinusitis; patients eventually need surgical treatment for infections that are intractable to treatment by antibiotics [24,25]. Despite the antimicrobial resistance of bacterial isolates, the biofilm also has a substantial role in antimicrobial resistance. A Korean nationwide cohort study found that H. influenzae infection by ampicillin-resistant, β-lactam-sensitive isolates were significantly prevalent in pediatric children [26]. In the past 10 years, studies in European and Western countries have also found a similar finding [23]. This has resulted in the increased dosage of Hib minimum inhibitory concentration (MIC) of augmentin (i.e., amoxicillin-clavulanate) to treat pediatric adenoiditis with MEE [19,24]. Biofilm formation may be the reason for these findings, even in β-lactam-sensitive Hib strains [25].
In this study, we found that β-lactam-sensitive isolates caused the formation of Hib biofilm, which then leads to the surgical treatment of patients with pediatric adenoiditis and otitis media. By contrast, the β-lactam-resistant Hib strain significantly reduced biofilm formation. This finding was supported by a previous study that found that β-lactamase-producing bacteria may affect peptidoglycan remodeling, which then inhibits bacterial biofilm formation [27]. In addition, our results may explain why surgical intervention may still be needed for β-lactam-sensitive strains in cases of pediatric adenoiditis and MEE. We also found less biofilm formation in the pediatric OSA group, but their adenoids still harbored β-lactam-sensitive Hib isolates. The effect of using augmentin (i.e., amoxicillin-clavulanate) for treating pediatric OSA caused by adenoid vegetation is unknown. However, this correlation could lead to new clinical trials in the future.
A previous study reports that the coinfection of Hib and S. pneumoniae caused LuxS (i.e., S-ribosylhomocysteinase) transmittance and induced β-lactam resistance [28]. The β-lactamase-positive Hib species may use quorum sensing to coordinate gene expression, based on the density of their local population [29]. Biofilm formation also induces the quorum sensing of β-lactam-sensitive strains to augmentin-resistant strains, even through they render a β-lactam-sensitive culture [30]. However, most of our patients' adenoids harbored a single strain of Hib; there were only two adenoids that contained S. pneumoniae and E. coli coinfection. Therefore, our survey could show a single strain of Hib in chronic adenoiditis with MEE that is correlated with β-lactam resistance or biofilm formation in pediatric chronic adenoiditis than in pediatric OSA. The results of this study suggest that patients with MEE-AH or OSA who harbor Hib and biofilm formation should be treated surgically because the bacterial pathogen is a continual threat [21,31].
In this study, out of the 384 patients who underwent an adenoidectomy, only 34 were infected with Hib. Two patients with MEE combined with OSA were excluded from this study. Biofilm formation was observed in 8/18 in the MEE group with Hib infection and 0/14 in the OSA group that harbored Hib. Because all cultures were obtained from surgical specimens, they did not respond to treatment with antibiotics and the patients presented persistent MEE. This lead to hearing handicap and the patients eventually underwent adenoidectomy and middle ear ventilation tube insertion. Additionally, patients with OSA presented with prominent adenoid hypertrophy and tonsillar enlargements underwent tonsillectomy and adenoidectomy and were not administered antibiotics before surgery in our study. On the other hand, patients with MEE harbored positive β-lactamase Hib, and amoxicillin-clavulanate was considered as the initial antibiotic treatment, followed by third generation cephalosporins if the patient showed no improvement. In contrast, patients with MEE harbored negative β-lactamase Hib were considered for early surgical intervention, if a poor response was exhibited to empirical antibiotic treatment because of a greater trend of biofilm formation. However, further clinical studies are warranted on Hib-related MEE-AH in pediatric patients.
Conclusions
H. influenzae type b sensitivity cannot solely be used to treat pediatric chronic adenoiditis and MEE disease in the current era. Frequent Hib-related biofilm formation may cause medication failure and lead to surgical treatment. Although it is generally believed that the patients with Hib-related biofilm formation may fail antibiotic therapy, and be more likely to require surgery, there is no data to support or refute this in the current study. The detailed data regarding previous treatment history, continued or progression of symptoms, and the association with biofilm formation or antimicrobial resistance should be included in the future study.
Footnotes
Acknowledgments
The authors thank Yun-Ju Sung (Departments of Laboratory Medicine, China Medical University Hospital) for clinical isolation and identification of bacterial strains; and Shu-Chen Shen (Scientific Instrument Center, Academia Sinica) for confocal microscopy analysis.
This work was supported by research grants from the Ministry of Science and Technology (101-2314-B-039-013-MY3 and 101-2313-B-039-004-MY3); Taiwan Ministry of Health and Welfare Clinical Trial and Research Center of Excellence (MOHW103-TDU-B-212-113002); the China Medical University and Hospital (CMU102-ASIA-21, DMR103-025); and the Tomorrow Medicine Foundation.
Author Disclosure Statement
No conflicting financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.