
Abstract
Abstract
Background:
Obstructive sleep apnea (OSA) is associated with increased systemic oxidative stress, endothelial dysfunction, and activation of pro-inflammatory cascades, which increase host susceptibility to infection. OSA has not been evaluated as a risk factor for surgical site infection (SSI) following colectomy. We hypothesized that OSA increases the risk for SSI after colectomy.
Methods:
We performed a retrospective review of 507 colectomies that took place between August 2011 and September 2013. Forty-two patients carried the diagnosis of OSA prior to surgery. These 42 patients were matched to 68 patients with no OSA for age, body mass index (BMI), diabetes mellitus (DM), reason for surgery and surgical approach.
Results:
The rate of SSI was 28.6% (12 of 42) in the patients with and 10.3% (7 of 68) in the patients without OSA (p=0.03). Using logistic regression, the predictors of SSI following colectomy were found to be OSA (odds ratio [OR] of 3.98, 95% confidence interval [CI]=1.29–12.27), and DM (OR of 7.16, 95% CI=2.36–21.96). The average hospital stay after colectomy for patients with OSA complicated with SSI was 16.7 d whereas patients with OSA without SSI stayed 7.4 d (p<0.001). The rate of organ space infections was 9.5% (4 of 42) in the patients with OSA compared with 0 (p=0.02) in patients without OSA.
Conclusions:
OSA is an independent risk factor for SSI following colectomy. Patients with OSA have substantially greater rates of organ space SSI and longer hospital stay.
O
Patients and Methods
Patients
The study protocol was exempted from review as set forth in the Code of Federal Regulations, 45 CFR 46.101(b) by the University of Minnesota Institutional Review Board. Between August 2011 and September 2013, 507 colectomies were performed in adults at University of Minnesota Medical Center. Six patients had more than one procedure within 7 d and were excluded from analysis. Of the remaining 501 patients, 42 carried the diagnosis of OSA prior to surgery. These 42 patients were matched 1:1.5 to patients without OSA for major parameters that have been reported to be associated with SSI: Age, body mass index (BMI), DM, reason for surgery [cancer, infection, and inflammatory bowel disease (IBD)], and surgical approach (laparotomy or laparoscopy) [11–14]. Investigators were blinded to the study outcomes (SSI and hospital stay) during the selection process.
The diagnoses of OSA and DM, serum bicarbonate concentrations, and hospital length of stay after colectomy were extracted from the electronic medical record. More specifically, we extracted the OSA diagnosis from the anesthesia pre-operative records. In our institution, anesthesiologists screen for OSA although each staff uses a different screening tool. If the patient did not have OSA, the anesthesiologist recorded a “negative pulmonary history” in a mandatory field in our electronic medical records. Age, American Society of Anesthesiologists score (ASA), BMI, operational time, presence of SSI, reason for surgery, gender, surgical approach, and surgical site culture were extracted from our institutional SSI database. SSI diagnosis and classification to superficial incisional, deep incisional and organ space SSI were made according to CDC guidelines [15].
Primary and secondary outcomes
Primary outcome is the rate of SSI following colectomy. Secondary outcomes are length of stay in the hospital following operation, type (classification) of SSI, and isolated pathogens.
Statistics
Statistical analysis was performed using Epi info™ 7 (CDC, Atlanta, GA) and SAS v. 9.3. (SAS Institute Inc.,Cary, NC). Continuous data were compared using the anova or t test and ordinal data by the Chi-square test or Fisher exact test, as appropriate. Risk factors were evaluated separately for their association with SSI. The following variables were considered for the model: Age >65 years, female gender, ASA ≥3, serum bicarbonate concentrations (mEq/L), BMI (kg/m2), DM, cancer, IBD, infection of the colon, laparotomy, OSA, and procedure time >3 h. Table 2 gives the results for this analysis. Multivariable logistic regression models were created to evaluate the independent association of risk factors with SSI. Forward and backward stepwise regression was used to identify independent risk factors for SSI. The c-statistic was used to ascertain discrimination for the resultant parsimonious model. Model calibration was assessed using the Hosmer-Lemeshow goodness-of-fit statistic, with p>0.05 indicating acceptable model calibration. A p value of less than 0.05 signified statistical significance.
Results
Matching and patient demographics
We identified 42 patients with OSA undergoing colectomy. These were matched to 68 patients without documented OSA that underwent colectomy. The two groups had similar age, ASA score, BMI, rate of DM, reasons for surgery, surgical approaches, and duration of surgery. Demographic data from these groups are reported in Table 1.
Chi-square or t-test was performed between OSA and No OSA patients.
ASA=American Society of Anesthesiologists score; BMI=Body mass index; DM=diabetes mellitus; IBD=inflammatory bowel disease; OSA=obstructive sleep apnea.
Surgical site infection
The rate of SSI was 28.6% (12 of 42) in the patients with, and 10.3% (7 of 68) in the patients without OSA (p=0.03). Using logistic regression, the predictors of SSI following colectomy were found to be OSA (odds ratio [OR] of 3.98, 95% confidence interval [CI]=1.29–12.27), and DM (OR of 7.16, 95% CI=2.33–21.96) (Table 2).
ASA=American Society of Anesthesiologists score; BMI=Body mass index; DM=diabetes mellitus; IBD=inflammatory bowel disease; OSA=obstructive sleep apnea; DF=degrees of freedom.
Secondary endpoints
Interestingly, SSI prolonged hospital stay after colectomy only in patients with OSA (Fig. 1). The average hospital stay after colectomy for patients with OSA complicated with SSI was 16.7 d whereas patients with OSA without SSI stayed an average of 7.4 d (p<0.001). The average stay for patients without OSA complicated with SSI was 7.7 d whereas the average for patients without OSA that did not develop SSI following colectomy was 9.3 d (p=0.92). The mean length of hospital stay of patients with OSA complicated with organ space infection was 24±2.2 (SD) d whereas the mean hospital stay of total population in our cohort was 9.5±7 (SD) d.
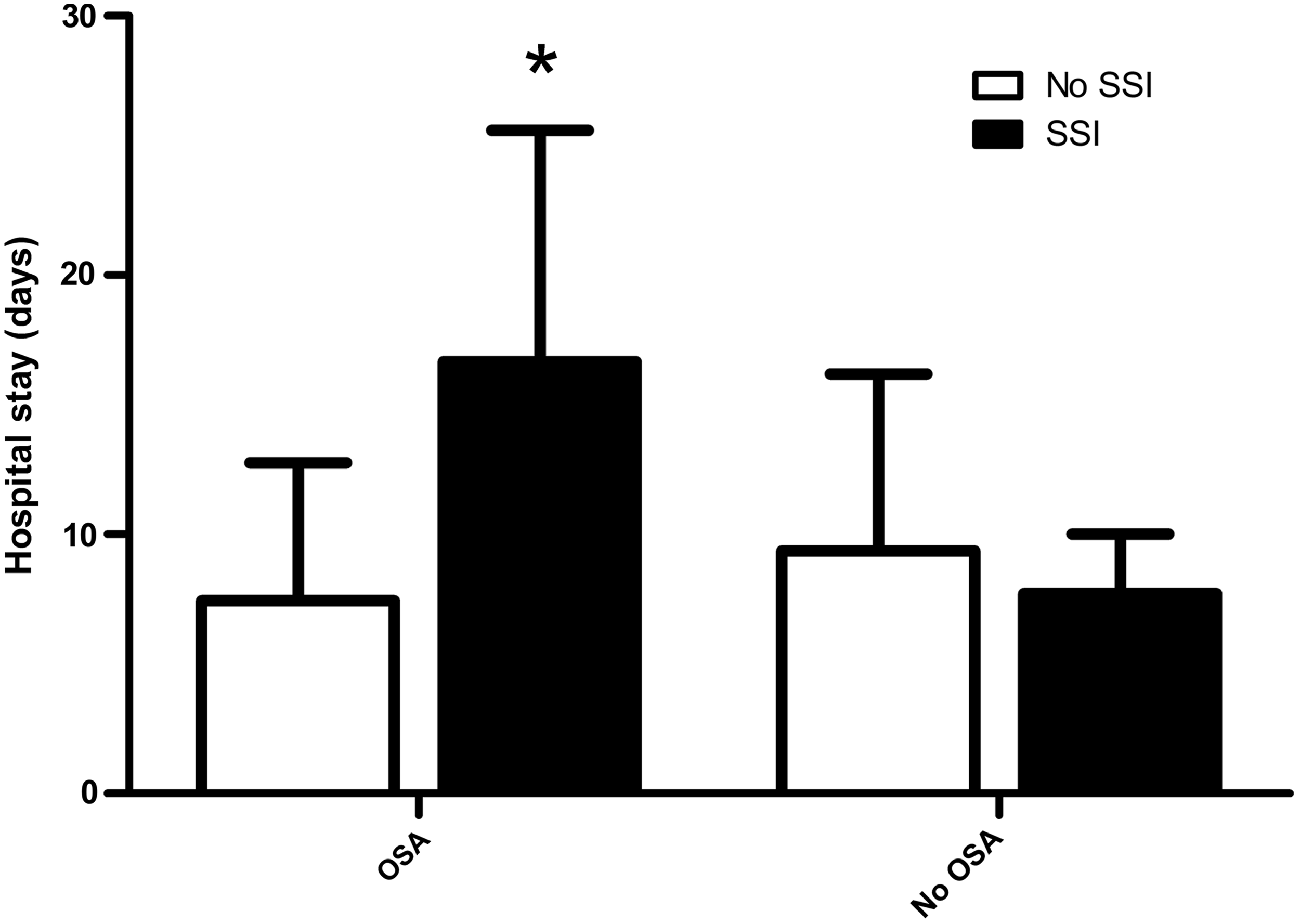
Hospital stay following colectomy of patients with (OSA) and without obstructive sleep apnea (No OSA) that were complicated with surgical site infection (SSI) and were not complicated with surgical site infection (No SSI). * p<0.05 patients with SSI and OSA vs rest of the groups.
The rate of organ space infections was 9.5% (4 of 42) in the patients with OSA compared with 0 (p=0.02) in patients without OSA. No patients had confirmed anastomotic leakage. The rate of deep incisional infections was 2.4% (1 of 42) in patients with OSA and 0 in patients without OSA (p=0.38). The rate of superficial SSIs in patients with OSA (17%; 7 of 42) was greater compared with patients without OSA (10.3%; 7 of 68) but not statistical substantially (p=0.38) (Fig. 2).
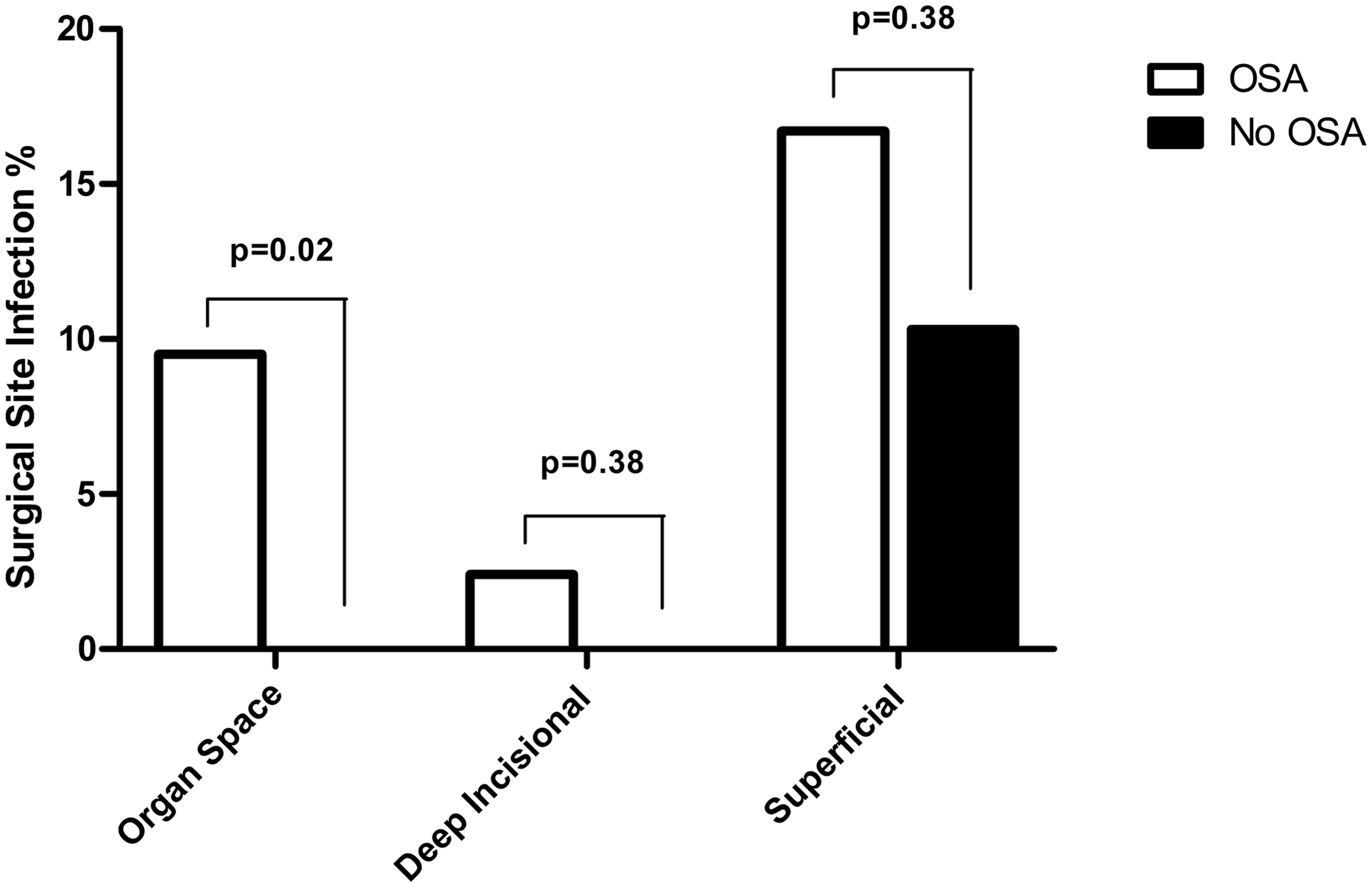
Rate of organ space, deep incisional, and superficial incisional surgical site infection in patients with (OSA) and without obstructive sleep apnea (No OSA).
Cultures were not performed in seven patients that developed post-operative SSI. One (5.3%) had negative culture and 11 of the 19 (57.9%) patients that developed post-operative SSI had positive cultures. Eight (42.1%) patients had polymicrobial infection and three (15.8%) of them had gram-positive bacteria in their culture (Fig. 3A). The most prevalent bacteria isolated from SSI of patients with OSA were Enterococcus, Klebsiella, and Streptococcus species, whereas in patients without OSA the most prevalent isolate was coagulase negative Staphylococcus (Figure 3B).

Discussion
Our study identifies OSA as a risk factor for development of SSI following colectomy. Adjusting for other confounders, OSA and DM are the only independent risk factors identified for SSI following colectomy in our study population. SSI is associated with longer hospital stay after colectomy only in patients with OSA. Organ space SSI is more common among OSA patients.
OSA is a well recognized risk factor for peri-operative pulmonary and cardiovascular complications [16,17]; however, little is known about its role in surgical incision healing and SSI. A study from the Cleveland Clinic showed that the rate of mediastinitis after cardiac surgery was five times greater in patients with OSA [18]. To our knowledge, that is the only study apart from the present one which has identified OSA as risk factor for SSI. We found that the rate of SSI in OSA patients is more than double (28.6%) the rate of patients with no OSA (10.3%). The overall SSI rate for both groups combined is 17.3%, which is similar to rate of SSI following colectomy (12.2% to 26%) reported by other authors [12,13,19,20].
OSA is a common disease, affecting 24% of men and 9% of women in the United States [21]. The prevalence of moderate and severe OSA, which requires treatment with positive airway pressure, is 9% and 4% for men and women, respectively [21]. OSA is associated with several conditions and diseases including DM [22] and obesity [23]. Additionally, OSA contributes to a greater ASA score [24], and is more common in older age [21]. All of these factors have been reported as risk factors for SSI [11,12,14]. Our study is the first that identifies OSA as an independent risk factor for SSI following a commonly performed general surgical procedure. Apart from OSA, we identified DM as another independent risk factor for SSI in our cohort. Age >65 years, ASA >3, bicarbonate concentrations, reason for colectomy, laparotomy, BMI, or procedure time >3 h are not associated with increased risk for infection in our study group, although these are frequently reported in the literature [11–13]. This discrepancy may result from the small sample size population of our cohort.
SSI increases length of hospital stay following several types of surgery, including colectomy [25,26]. OSA is also associated with longer hospitalizations mostly because of respiratory reasons [27]. In our cohort, the length of stay is similar among patients with OSA not complicated with SSI, patients without OSA not complicated with SSI, and patients without OSA complicated with SSI. A likely explanation of this observation is the small size of our cohort. SSI is associated with longer hospital stay after colectomy only in patients with OSA. Organ space infections are more common among OSA patients. The mean length of hospital stay of patients with OSA complicated with organ space infection is 24±2.2 (SD) d, which is much longer than the mean hospital stay of total population of our cohort (9.5±7 (SD) d) although we did not attempt a statistical analysis because of the small numbers. The greater rate of organ space infections in patients with OSA is most likely the reason for the longer hospital stay after colectomy in patients with OSA. This finding is consistent with the previously noted study by Kaw et al. [18], demonstrating an increased rate of mediastinitis after heart surgery in OSA patients. Although obesity is a risk factor for organ space and deep incisional SSI [14], the mean BMI of our groups is similar. This strongly suggests that OSA is an independent risk factor for SSI.
Most positive cultures from SSI in this study are polymicrobial, with the most prevalent microorganisms being gram-positive bacteria. Contrary to large SSI databases [28–30], Enterococcus and Streptococcus are the most common isolated microorganisms in this cohort. This finding may be the result of our small population sample and potentially because of the high frequency of polymicrobial cultures [31].
The etiology of increased SSI in patients with OSA cannot be determined in this retrospective study. Nevertheless, we can speculate regarding potential causes. OSA results in intermittent hypercapnia and hypoxia during sleep (apnea). At daytime, patients with OSA have no apnea and no hypercarpnia and that is the reason that their baseline bicarbonate are within the normal limits [32]. During the anesthesia and post-anesthesia period, patients with OSA have more frequent and longer episodes of apnea and thereby have worse and longer hypercapnia and hypoxemia. On the contrary, patients with obesity hypoventilation syndrome (OHS) have hypercapnia and/or hypoxemia at daytime [33]. Although the majority of patients with OHS have OSA, most patients with OSA do not have OHS [34]. OHS is an underdiagnosed condition and rarely reported, as most of the clinicians are not aware of the syndrome. In our cohort, patients with OSA have greater concentrations of serum bicarbonate than the non-OSA patients (26.9 vs 25.4, p=0.025) but this difference is not clinically significant. This finding argues against a clinically substantial difference in the baseline (daytime) carbon monoxide between the two groups. However, as we explained above, patients with OSA have worse and longer hypercapnia and hypoxemia post-operatively.
Hypoxemia and hypercapnia affect surgical site healing [35–37].Tissue hypoxia impairs surgical site healing and oxygen supplementation in colorectal surgery patients has been shown in some studies to reduce risk of SSI [38]. On the other hand, tissue hypercapnia appears to improve surgical site healing [37,39]. Increased CO2 concentrations in the tissue cause vasodilation and improved tissue perfusion, with resultant improved surgical site healing [40]. Perhaps the beneficial effect of hypercapnia on surgical site healing in patients with OSA is less notable because of the hypoxemia and increased systemic inflammation associated with OSA. OSA also results in increased systemic oxidative stress, endothelial dysfunction, and activation of pro-inflammatory cascades [5,41], all of which have been demonstrated to impair surgical site healing [6]. These factors may notably contribute to impaired anastomotic healing, with micro leaks of anastomosis resulting in increased rates of organ space SSI in the patients with OSA [42,43]. The pathogenesis of increased rate of SSIs in OSA population bears further investigation.
Moreover, micro leaks at the anastomosis in patients with OSA may be the reason of greater rate of organ space SSIs compared with patients without OSA whereas there is no difference in the superficial SSIs between the two groups. Kaw et al. reported that the rate of mediastinitis was 8.1% in OSA vs 1.08% in the non-OSA patients and the rate of other infections was 1.7% vs 0%, respectively [18]. Although this “paradoxical finding” could be the result of our small sample size, it is possible that OSA may result in more SSIs because of impaired healing of the anastomosis through the aforementioned suggested mechanism. Therefore, OSA increases primarily the organ space infection rather than superficial SSI. Such a differential effect of risk factors on each SSI type has been previously reported [14].
This study is limited by its retrospective and case-matching nature, which may introduce biases, although the investigators were blinded to the outcomes during the matching process. OSA diagnosis was retrieved from the anesthesia pre-operative records and was not confirmed by a sleep study. It is possible that some of the patients labeled as non-OSA may have OSA. Severity of OSA and compliance of OSA treatment, i.e., use of continuous positive airway pressure (CPAP) as directed, were also not included in analysis. We could not reliably document peri-operative use of CPAP in patients with OSA. However, it is the policy of our hospital to require central monitoring for at least 24 h after general anesthesia. In addition, the sample size was small, especially in regards to the microbial data. Nevertheless, we believe that this limitation does not undermine the importance of our findings, because OSA was associated with greater SSI rates even when adjusting for other known major risk factors for SSI. SSI does not only increase mortality and morbidity, but also prolongs hospital stay and increases cost [26]. Further studies are needed to elucidate the effect of OSA on SSI following other type of operations.
In conclusion, our study identifies OSA as an independent risk factor for SSI following colectomy. Patients with OSA have substantially greater rates of organ space SSI and longer stay. We recommend that patients with OSA be treated as a high risk population for SSI after a surgical procedure, especially following colectomy.
Footnotes
Author Disclosure Statement
The authors have no conflicts of interest in relation to this work.