
Abstract
Abstract
Background:
Necrotizing pancreatitis is a challenging condition that requires surgical treatment commonly and is associated with substantial morbidity and mortality. Over the past decade, new definitions have been developed for standardization of severity of acute and necrotizing pancreatitis, and new management techniques have emerged based on prospective, randomized clinical trials.
Methods:
Review of English-language literature.
Results:
A new international classification of acute pancreatitis has been developed by PANCREA (Pancreatitis Across Nations Clinical Research and Education Alliance) to replace the Atlanta Classification. It is based on the actual local (whether pancreatic necrosis is present or not, whether it is sterile or infected) and systemic determinants (whether organ failure is present or not, whether it is transient or persistent) of severity. Early management requires goal-directed fluid resuscitation (with avoidance of over-resuscitation and abdominal compartment syndrome), assessment of severity of pancreatitis, diagnostic computed tomography (CT) imaging to assess for necrotizing pancreatitis, consideration of endoscopic retrograde cholangiopancreatography (ERCP) for biliary pancreatitis and early enteral nutrition support. Antibiotic prophylaxis is not recommended. Therapeutic antibiotics are required for treatment of documented infected pancreatic necrosis. The initial treatment of infected pancreatic necrosis is percutaneous catheter or endoscopic (transgastric/transduodenal) drainage with a second drain placement as required. Lack of clinical improvement after these initial procedures warrants consideration of minimally invasive techniques for pancreatic necrosectomy including video-assisted retroperitoneal debridement (VARD), minimally invasive retroperitoneal pancreatectomy (MIRP), or transluminal direct endoscopic necrosectomy (DEN). Open necrosectomy is associated with substantial morbidity, but to date no randomized trial has documented superiority of either minimally invasive or open surgical technique. Additional trials are underway to address this.
Conclusions:
Severe acute and necrotizing pancreatitis requires a multi-disciplinary treatment strategy that must be individualized for each patient. Optimal treatment of necrotizing pancreatitis now requires a staged, multi-disciplinary, minimally invasive “step-up” approach that includes a team of interventional radiologists, therapeutic endoscopists, and surgeons.
N
Substantial changes in the management of necrotizing pancreatitis have emerged in the last decade. Non-operative management is recommended for sterile pancreatic necrosis. Antibiotic prophylaxis is not indicated in the initial management of pancreatic necrosis. Antimicrobial management is indicated for the treatment of infected pancreatic necrosis. Randomized trials confirm that treatment with open necrosectomy results in greater morbidity than conservative surgical approaches. Percutaneous drainage is now the preferred initial technique for treatment of infected pancreatic necrosis. Both endoscopic transluminal drainage and minimally invasive necrosectomy have emerged as secondary techniques for treating infected pancreatic necrosis. Optimal treatment of necrotizing pancreatitis now requires a staged, multi-disciplinary, minimally invasive “step-up” approach which includes a team of interventional radiologists, therapeutic endoscopists, and surgeons. In this comprehensive review, we provide evidence-based treatment recommendations for necrotizing pancreatitis management and highlight a clinical case to illustrate this treatment algorithm.
Clinical Case
A 38-year-old female presented to an outside hospital with acute onset of abdominal pain, anorexia, nausea, and vomiting 9 d after a 2-d hospital stay for gallstone pancreatitis. During her previous hospitalization she underwent endoscopic retrograde cholangiopancreatography (ERCP) for choledocholithiasis and was discharged home with a plan for delayed cholecystectomy. Upon arrival to the emergency department, a non-contrast abdominal computed tomography (CT) scan demonstrated a pancreatic phlegmon with retroperitoneal air, concerning for infected necrotizing pancreatitis and possible duodenal perforation. Given these findings, she was transferred to the University of Michigan Medical Center for further management.
The patient's past medical history was notable for hypertension, hyperlipidemia, and recent supraventricular tachycardia. On initial physical examination she was afebrile and found to have diffuse abdominal tenderness without evidence of peritonitis. A pancreatic protocol intravenous contrast abdominal CT scan demonstrated extensive pancreatic necrosis, with a large pancreatic abscess (Fig. 1). Empiric, broad-spectrum antibiotic therapy (meropenem) was initiated.
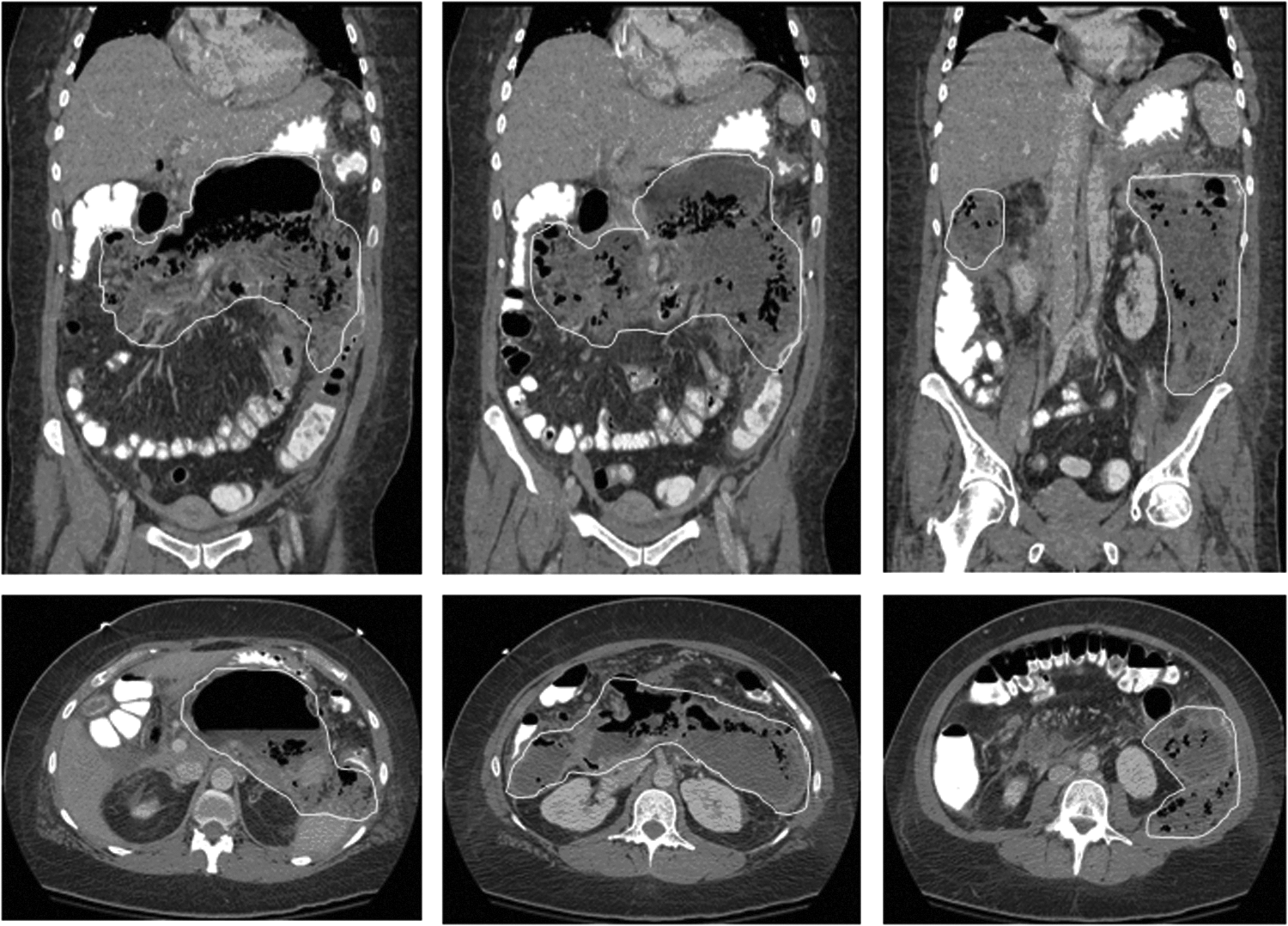
Admission computed tomography (CT) scan of the abdomen and pelvis with oral and intravenous contrast. No normal pancreatic tissue is identified. There is extensive pancreatic necrosis with large collections of fluid and gas throughout the pancreatic bed, extending caudally in the retroperitoneum, left greater than right. These collections show broad contact with the descending colon and there is adjacent mild thickening of the wall of the descending colon.
Considering her clinical status, vital signs, physical examination, and laboratory studies, the patient was managed with percutaneous drainage in an attempt to avoid the morbidity associated with early necrosectomy. Percutaneous drain placement by interventional radiology was performed without complication. Cultures of the pancreatic abscess grew multiple organisms including Enterococcus sp., Klebsiella pneumoniae, and Pantoea sp. for which a 3-wk course of intravenous piperacillin-tazobactam was initiated.
During the course of her hospitalization, a CT angiogram demonstrated a small splenic artery aneurysm. She underwent celiac, splenic, common hepatic, gastroduodenal artery, and superior mesenteric artery arteriography with embolization of the aneurysm at the splenic hilum. She was discharged home with continued antibiotic therapy and drain care. On outpatient follow-up the patient presented without complaints. Repeat CT scan imaging 4 wks later confirmed complete resolution of infected pancreatic necrosis (Fig. 2) and the percutaneous drainage catheter was removed. She underwent uncomplicated laparoscopic cholecystectomy 4 wks later. Final pathology showed evidence of cholelithiasis and lymphocytic cholecystitis. This case illustrates the efficacy of percutaneous drainage for treatment of infected pancreatic necrosis, even in a patient with extensive peri-pancreatic infected necrosis.
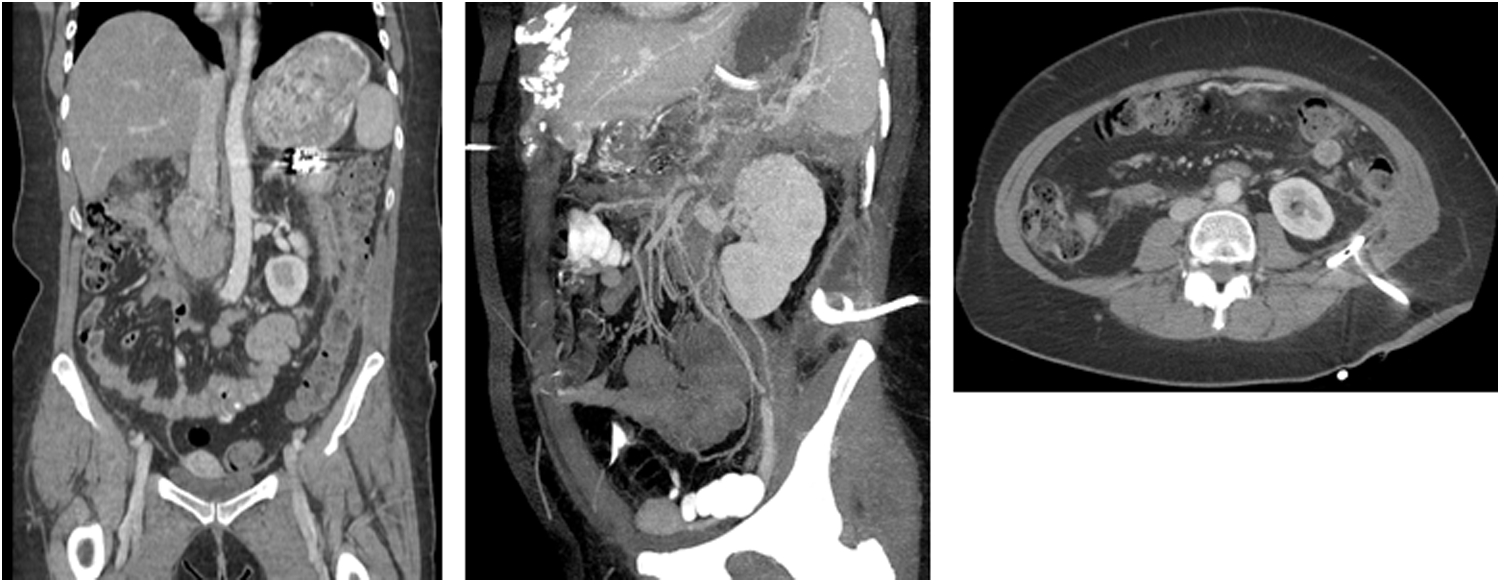
Repeat computed tomography (CT) scan (4 wks after admission) of the abdomen and pelvis with oral and intravenous contrast. After radiologic image-guided percutaneous drain placement at outpatient follow-up: Near resolution of the previously noted collections with a marked improvement in inflammation.
Diagnosis
Presentation
Acute pancreatitis most often presents as the sudden onset of upper abdominal or epigastric pain, many times radiating to the back. The pain may be accompanied by nausea, vomiting, fever, or elevated white blood cell count [1–3]. More severe cases can present with manifestations of respiratory distress and organ failure, as well as shock. The differential diagnosis for acute pancreatitis includes acute coronary syndrome, acute cholecystitis, perforated gastroduodenal ulcer, mesenteric ischemia, bowel obstruction, and bowel perforation.
Physical examination may be largely unremarkable with only minimal epigastric tenderness in patients with mild disease. More severe illnesses may present with diffuse abdominal tenderness, distention from ileus, and signs of systemic inflammation including tachycardia, tachypnea, and hypotension. Ecchymosis within the umbilical region (Cullen sign) or the flank (Grey-Turner sign) although non-specific, may represent retroperitoneal hemorrhage associated with severe necrotizing pancreatitis [4]. Other signs such as icterus and jaundice, hepatomegaly, or xanthomas or other skin lesions, may help aide in identifying the underlying etiology.
Diagnostic assays
Several key diagnostic assays assist in the differentiation of acute pancreatitis from the disease processes mentioned previously. Serum amylase or lipase concentrations greater than three times the upper limit of normal, especially in severe abdominal pain, are suggestive of acute pancreatitis. Although both enzymes can be measured readily, lipase is as sensitive as, and more specific than, amylase [5]. Furthermore, amylase concentrations tend to decrease more quickly and thus a patient with any delay in presentation or diagnosis may be out of the diagnostic window [6].
Markers suggestive of increased trypsinogen activation (trypsinogen activation peptide, trypsinogen-2) are less sensitive in acute pancreatitis but may be helpful in confirming the diagnosis. A 2001 report on serum markers to address the severity of acute pancreatitis noted that procalcitonin concentrations are elevated in patients with acute infected pancreatic necrosis. Furthermore, a rapid test strip test for procalcitonin (PCT-Q, B.R.A.H.M.S., Thermo Fisher Scientific, Waltham, MA) was described as an effective screening test (sensitivity 92%–95%, negative predictive value 97%) for detecting severe acute pancreatitis at 24 h post-admission, compared with other commonly used predictors of severity (C-reactive protein concentrations, Ranson scores, and Acute Physiology and Chronic Health Evaluation [APACHE] II scores) [7].
Diagnostic imaging
Contrast-enhanced computed tomography (CECT) is a key tool in differentiating severe acute pancreatitis from other sources of upper abdominal pain, and should be performed within 72 h of symptom onset [8]. Contrast-enhanced computed tomography is also the gold standard for diagnosis of pancreatic necrosis in acute pancreatitis and a new, more standardized definition for radiologic terminology is being sought to classify findings better [9]. Pancreatic necrosis appears as areas of low- to no-enhancement on CECT due to disruptions in the pancreatic microcirculation. If the pancreas is greater than 30% necrotic, the accuracy of CECT in diagnosing necrotizing pancreatitis reaches 90%. The amount of necrotic glandular tissue by CECT is also a predictive factor for the severity of the disease and is stratified into three categories: less than 30%, 30%–50%, and greater than 50% necrosis. Infection of the necrotic tissue is diagnosed via CT or ultrasound-guided, fine-needle aspiration of the tissue, followed by culture and gram stain. Of the available options, CT-guided aspiration is preferred because it has a higher sensitivity and specificity versus other modalities.
Evolving Definitions
1992 Atlanta Classification
Severe acute pancreatitis was described initially in 1992 on the basis of the Atlanta Classification [10]. It defined acute pancreatitis as “an acute inflammatory process of the pancreas with variable involvement of other regional tissues or remote organ systems.” Furthermore, severe acute pancreatitis was defined as “acute pancreatitis associated with organ failure or local complications such as necrosis, abscess or pseudocyst” (Tables 1 and 2). Although non-specific, this represented the first true attempt at creating a standardized definition of the pancreatitis disease process.
Adapted from: Bradley EL 3rd. A clinically based classification system for acute pancreatitis. Summary of the International Symposium on Acute Pancreatitis, Atlanta, GA, September 11–13, 1992. Arch Surg. 1993;128:586–589 and Bollen TL, van Santvoort HC, Besselink MG, et al. The Atlanta Classification of AP revisited. Br J Surg 2008;95:6–21.
CECT=contrast-enhanced computed tomography; SIRS=systemic inflammatory response syndrome; BMI=body mass index; WBC=white blood cell count.
CECT=contrast-enhanced computed tomography; APFC=acute peri-pancreatic fluid collections; PNPFC=post-necrotic pancreatic/peri-pancreatic fluid collections; WOPN=walled-off pancreatic necrosis.
2008 Acute Pancreatitis Working Group
A 2008 evaluation of the Atlanta Classification suggested that the definitions outlined in 1992 were used infrequently, inconsistently, and inappropriately [11]. Furthermore, a better understanding of the disease process, enhanced imaging modalities, and new intervention strategies had all been developed since the Atlanta Classification's inception. The Atlanta Classification has several limitations. It does not account for the length of time since inception of the disease, it fails to distinguish between peri-pancreatic and pancreatic parenchymal necrosis, it relies too heavily on only modestly accurate severity predictors on an individual patient level, and it fails to establish exact radiologic criteria regarding local complications. The 2008 Acute Pancreatitis Working Group wanted to update, clarify, and improve clinical assessment, and standardize the definitions described by the Atlanta Classification. These distinctions are summarized in Tables 1 and 2.
2011 World Congress
Although the 2008 Atlanta Classification represents an improvement over the 1992 classification, in 2011 the World Congress of the International Association of Pancreatology suggested an expansion of the classification system to incorporate better the risks associated with multiple organ dysfunction syndrome. They argued that a binary classification system did not stratify patients sufficiently with respect to their mortality risk.
A new international classification of severity of acute pancreatitis based on the actual local (whether pancreatic necrosis is present or not, whether it is sterile or infected) and systemic determinants (whether organ failure is present or not, whether it is transient or persistent) of severity (Table 3) was developed by PANCREA (Pancreatitis Across Nations Clinical Research and Education Alliance) to replace the Atlanta Classification. The new system uses local and systemic determinants of severity to categorize acute pancreatitis into four subcategories: mild, moderate, severe, and critical (Table 4) [12]. It is hoped that this new definition and classification system will standardize patient severity for all future clinical trials of acute and necrotizing pancreatitis.
SOFA=Sepsis-related Organ Failure Assessment score; CT=computed tomography.
Adapted from: Dellinger EP, Forsmark CE, Layer P, et al; Pancreatitis Across Nations Clinical Research and Education Alliance (PANCREA). Determinant-based classification of acute pancreatitis severity: An international multidisciplinary consultation. Ann Surg 2012;256:875–880.
AP=acute pancreatitis.
Adapted from: Dellinger EP, Forsmark CE, Layer P, et al. Pancreatitis Across Nations Clinical Research and Education Alliance (PANCREA). Determinant-based classification of acute pancreatitis severity: An international multidisciplinary consultation. Ann Surg 2012;256:875–880.
Epidemiology
Acute pancreatitis is a common and often self-limiting inflammatory process involving the pancreas and surrounding tissues. Although substantial limitations exist in determining the true incidence, it is believed to be between 4.9 and 35 per 100,000 persons each year [13] with an annual cost of more than $2 billion [14]. Chronic ethanol abuse and cholelithiasis are the two most common etiologies, accounting for nearly 220,000 hospital admissions annually [15]. Approximately 15%–20% of these patients progress to severe acute pancreatitis, a less common self-limiting disease process, with a mortality rate of 10%–30%.
Severe acute pancreatitis progresses to necrotizing pancreatitis in approximately 15% of patients. Infected pancreatic necrosis occurs in 30% to 70% of patients with necrotizing pancreatitis and is associated with a high mortality rate (19%–24%) compared with sterile necrotizing pancreatitis (7%–11%). Within all of these categories, multiple organ dysfunction syndrome is a major prognostic factor for mortality as well as infection [16,17] and early surgical intervention [18]. Long-term outcomes associated with necrotizing pancreatitis include compromised endocrine and exocrine function, with the severity of these outcomes related to the amount of necrotic pancreatic tissue and degree of infection.
Pathophysiology
Activation of zymogens
A cornerstone of the development of acute pancreatitis is an inciting event that causes abnormal activation or accumulation of trypsinogen. Normally, active trypsin is stored in acinar vacuoles. In acute pancreatitis these vacuoles become overwhelmed and eventually rupture, releasing active trypsin. Active trypsin then activates free trypsinogen and other pancreatic zymogens that are capable of pancreatic tissue digestion and activation of the complement cascade. These enzymes can also cause damage to the local microvasculature, resulting in vasoconstriction and decreased oxygen perfusion that can lead to progressive ischemia [19].
Inflammatory cell response
Cellular injury leads to complement activation and subsequent macrophage and polymorphonuclear leukocyte recruitment. Activation of these cells leads to the release of a number of mediators that can worsen pancreatic injury by acting as proinflammatory mediators or by causing further activation of pancreatic zymogens.
Once a cell is damaged beyond the point of repair, it undergoes either apoptosis or necrosis depending on the environment. Apoptosis is a highly structured process of planned cell death that requires an abundance of energy. Macrophage recognition of apoptotic cell-associated molecular patterns (ACAMPs) produces anti-inflammatory effects. Mild forms of acute pancreatitis tend to be associated with acinar apoptosis, leading to pancreatic atrophy and subsequent resolution of symptoms. Furthermore, in severe acute pancreatitis, apoptosis has been found not only within the pancreas itself, but also in other organs, possibly contributing to the systemic effects associated with the disease process [20].
Necrosis
Necrosis is less energy-dependent and more chaotic than apoptosis. Necrotic debris is recognized by macrophages as a pathogen-associated molecular pattern (PAMP). The interaction of PAMPs with macrophage toll-like receptors activates nuclear factor-κB (NF-κB), an inhibitor of apoptosis as well as an indirect promoter of necrosis, and an important transcription factor for multiple proinflammatory mediators. Animal studies have demonstrated a relationship between NF-κB and mechanisms of cellular inflammation and apoptosis in acute pancreatitis [21].
Necrotic pancreatic tissue is found in more severe forms of acute pancreatitis and can lead to complications such as acute necrotic collection (ANC), walled-off pancreatic necrosis (WOPN), or pseudocyst formation [22]. Infection of the necrotic tissue most often occurs secondary to a compromise in the normal gut-pancreas barrier, allowing normal enteric flora to translocate from the gastrointestinal system into the pancreas. Infected pancreatic tissue may lead to local or systemic effects including sepsis and multiple organ dysfunction syndrome.
Management
Antibiotics
Historically, the use of prophylactic antibiotics in sterile necrotizing pancreatitis has been controversial. Early trials tested the efficacy of ampicillin, whereas later trials included antimicrobial agents such as carbapenems, fluoroquinolones, or cephalosporins. Although initial small studies demonstrated some benefit [23], this was not confirmed in three major randomized controlled trials [24–26]. Multiple meta-analyses confirmed no significant infection reduction or mortality benefit in patients with pancreatic necrosis with prophylactic antibiotics [27–29]. Current evidence-based recommendations do not support the use of prophylactic antibiotics for ANP.
Evidence of infected pancreatic tissue, sepsis, and systemic inflammatory response syndrome (SIRS) are indicators for therapeutic antimicrobial agent use in acute pancreatitis [30]. Furthermore, factors such as an elevated lactate dehydrogenase cocentrations, low PaO2, higher CT severity index, and delayed fluid resuscitation have been associated with an increased risk of infection [31]. Pathogens spread easily from the non-encapsulated pancreas to other abdominal organs. Most commonly gram-negative in bacteriology, an increase in gram-positive organisms, has been noted [32,33]. In sepsis, early empiric broad-spectrum antibiotics are recommended to reduce mortality, as inappropriate antimicrobial administration results in a five-fold increase in mortality in septic shock [34]. Broad-spectrum antibiotics should be adjusted and narrowed based on final culture and susceptibility results. Failure to do so has resulted in an increased incidence of multi-drug resistant organisms [35] as well as fungal infections [36] within the pancreatic tissue. Fine-needle aspiration (FNA) may be useful in patients with signs of sepsis but equivocal findings of infected pancreatic necrosis on diagnostic imaging and is particularly helpful in pathogen identification and appropriate de-escalation of antimicrobial therapy for infected pancreatic necrosis [37].
Resuscitation
Fluid losses are of major concern in acute pancreatitis and are increasingly important in severe cases. Goal-directed resuscitation with intravenous fluids is recommended to correct for potential volume depletion-related complications with an aim to maintain a heart rate under 100 beats/min and systolic blood pressure >90 mm Hg [38,39]. After initial bolus fluid therapy to achieve hemodynamic stability is completed [28], a continuous infusion should be initiated at approximately 3 mL/kg/h [40]. Fluid rates should then be titrated and adjusted such that blood urea nitrogen (BUN) concentrations decrease to less than 22 mg/dL or at the very least begin to decrease [41]. A 2009 retrospective study suggested that there may be an early therapeutic window for aggressive fluid resuscitation. Furthermore, substantial third-space losses may be associated with increased complications such as worsening necrosis and organ dysfunction [42].
Given the importance of early, adequate fluid resuscitation, we have developed an online tool to help guide this initial phase. Termed “PancMap,” this resource provides an algorithm for establishing the diagnosis and severity of disease using the Bedside Index for Severity in Acute Pancreatitis (BISAP) score (Table 5), as well as calculations of initial intravenous fluid requirements and end points per goal-directed resuscitation. The BISAP score was chosen as a quick, easy method to assess severity of acute pancreatitis; multiple studies have confirmed that the BISAP predicts severity, death, and organ failure in acute pancreatitis as well as APACHE II does and better than Ranson criteria, CT severity index, and other scoring systems [43–45].
Score≥3 predicts severe disease (1 point for each variable within first 24 h).
Composite score ranges 0–5 and directly correlates with mortality.
From: Wu BU, Johannes RS, Sun X, et al. The early prediction of mortality in acute pancreatitis: A large population-based study. Gut 2008;57:1698–1703.
Current proposed end points for fluid resuscitation in acute pancreatitis include hemodynamic stability, urine output ≥0.5 mL/kg/h2, and a BUN concentration that is decreasing at 24 h. We have demonstrated that the use of an early, automated paging alert system and an intuitive Web-based point-of-care instrument that guides clinicians with early management of acute pancreatitis was associated with improved early fluid resuscitation and resulted in decreased length of hospital stay [46].
Appropriate fluid resuscitation is desired, but there is also risk with over-resuscitation with the potential for development of abdominal hypertension and subsequently abdominal compartment syndrome [47,48]. A recent systematic review reported that 38% of acute pancreatitis patients developed abdominal compartment syndrome which was associated with higher mortality (49% vs. 11% without abdominal compartment syndrome) [49]. If abdominal compartment syndrome does develop, decompressive laparotomy may be required. An ongoing randomized clinical trial aims to compare percutaneous drainage versus laparotomy for decompression (DECOMPRESS trial; ClinicalTrials.gov NCT00793715) [50]. Thus a balance must be reached between providing sufficient intravascular volume for end organ perfusion and avoidance of over-resuscitation to prevent these potential complications. The specific type of fluid (crystalloid or colloid) for optimal resuscitation in acute pancreatitis is unknown and may be moot as a systematic review found no significant differences [51].
Nutrition
In patients with mild acute pancreatitis, regular oral intake may resume with symptom improvement [52] or when patients are subjectively hungry [53]. By contrast, patients with moderate or severe pancreatitis may not be able to tolerate sufficient oral nutrition for a protracted period. Therefore, after initial resuscitation, early nutritional support should be provided to patients with an expected period of inadequate nutrition of at least 5 to 7 d [54].
Although parenteral nutrition was considered historically the route of choice, current evidence now demonstrates enteral nutrition to be superior when able to be tolerated. Several studies comparing the two methods of administration have been undertaken demonstrating improved outcomes with enteral nutrition for organ dysfunction, infectious complications [55,56], and mortality [57]. These benefits were emphasized further on meta-analysis [58,59] and a Cochrane review [60] demonstrated substantially improved morbidity and mortality with enteral nutrition. Furthermore, early initiation of parenteral nutrition (within 48 h) increases complications versus delayed (after 8 d) in critically ill patients [61]. Considering the above, parenteral nutrition should be limited to those patients who are unable to tolerate the enteral route due to ileus or worsening symptoms, with its initiation occurring after the initial severe inflammatory response [62,63].
In regards to the optimal location to administer enteral feeding, there is little evidence to differentiate between the efficacy of gastric versus jejunal enteral nutrition. No significant differences in complications of worsening organ dysfunction or mortality have been found [64,65]. Concerns for aspiration, worsening of abdominal pain, or diarrhea have all been raised, yet by meta-analysis were not more common with gastric feeding [66]. However, in patients with evidence of gastric outlet obstruction or in those who do not tolerate gastric feeding there may be benefit from jejunal access for enteral nutrition delivery. An ongoing multi-center trial (pancreatitis, very early compared with normal start of enteral feeding [PYTHON trial]) is comparing very early nasojejunal feeding within 24 h of acute pancreatitis onset to standard practice (oral nutrition on demand or enteral feeding after 72 h of acute pancreatitis onset) [67].
Debridement
The question of if and when to pursue surgical intervention in patients with necrotizing pancreatitis has become defined increasingly and trends have shifted toward reserving operative management to specific indications. In patients without evidence of infection, continued supportive therapy is recommended even in the setting of other organ dysfunction [68]. However, when evidence of infected necrosis is present, this may necessitate more invasive measures. Numerous studies support a reduction in morbidity and mortality when intervention is postponed. Waiting at least two [69] and ideally 4–6 wks, results in less associated complications and death versus early intervention [70–72]. However, in patients with worsening septic shock and clinical deterioration, early intervention may be warranted.
Open necrosectomy has been the traditional surgical intervention for infected pancreatic necrosis with the goal of removing all infected tissue to provide adequate source control of sepsis. It is an effective procedure that is largely responsible for the decrease in mortality from necrotizing pancreatitis in the past decades. However, open necrosectomy is associated with high morbidity and mortality (20%) rates, as well as risk of infection spread due to a lack of intra-abdominal compartmentalization [73]. Other complications associated with open necrosectomy include fascial dehiscence, incision complications, hemorrhage, gastrointestinal fistula, and incisional hernia.
Minimally invasive techniques have been developed to replace open necrosectomy for the treatment of infected pancreatitic necrosis. Percutaneous catheter drainage alone is an effective alternative to open necrosectomy and is associated with reduced morbidity and mortality in selected patients. However, it is a slow process and may be labor-intensive, may require multiple percutaneous drains, and frequent lavage and drain exchanges may be required. Although feasible in stable patients in a system with appropriate resources, this approach may not be adequate for optimal source control in patients who are critically ill [74]. Transluminal endoscopic drainage is also effective.
Video-assisted retroperitoneal debridement (VARD) or minimally invasive retroperitoneal pancreatectomy (MIRP) utilize the tract created by percutaneous drainage catheters as a guide for placement of a laparoscope into the retroperitoneum such that debridement and lavage can be undertaken under direct visualization [76]. Compared with open necrosectomy, improvement in morbidity and mortality has been demonstrated [76–78].
Transluminal direct endoscopic necrosectomy (DEN) involves placement of an endoscope (most commonly transgastric or transduodenal optimally with endoscopic ultrasound guidance), followed by transmural puncture with access to the adjacent peri-pancreatic collections. Subsequently, necrotic debris can be debrided and removed via numerous endoscopic techniques. By meta-analysis, the DEN procedure appears to be well tolerated with a resolution rate of 76% and relatively low morbidity (30%) and mortality (5%) in a select patient population [79]. A more recent systematic review confirmed 81% definitive successful treatment, 6% mortality and 36% morbidity with DEN [80]. Results from a U.S. multi-center series from six tertiary medical centers documented that successful resolution of WOPN was achieved with DEN in 91% of patients [81]. Best utilized with WOPN and performed by skilled endoscopists, DEN has been shown to be a viable option in the treatment of infected necrosis [82].
The “step-up” approach
Combining several of the above techniques, the “step-up” approach to management of infected pancreatic necrosis aims to utilize the least invasive technique first, with progressive escalation for treatment failure. Most commonly, percutaneous drain placement is the first modality, with some centers using endoscopic drainage as well. Stemming from the multi-center randomized controlled PANTER trial, if within 72 h of drain placement there was no clinical improvement (Fig. 3), a second drainage procedure was performed. If the patient fails to improve after the second drain placement, VARD is recommended as the next step in management. In the PANTER trial, fewer than two-thirds of the patients assigned to the step-up approach required VARD after percutaneous drainage failed. Compared with the patients randomized to open necrosectomy, the mortality rates were similar, however, those treated with the step-up approach experienced a significant reduction in new-onset organ dysfunction (12% vs. 40%, p=0.002) as well as long-term complications including the incidence of incisional hernia, new-onset of diabetes, and need for pancreatic enzyme replacement. A significantly lower rate of the composite end point of major morbidity or death was found in the step-up group (40% vs. 69%, p=0.006) [83]. When possible, intervention was delayed 4 wks after the onset of symptoms indicative of acute pancreatitis. This allowed ample time for potential resolution of the disease process or for the transformation of solid debris into liquefactive necrosis that could be managed with percutaneous drainage. The PANTER trial has added additional evidence to the recommendation that surgical intervention should be delayed as long as possible while less invasive medical and radiologic interventions are used [84,85].

Step-up approach to management of infected ancreatic necrosis. Adapted from: Besselink MG, van Santvoort HC, Nieuwenhuijs VB, et al. Dutch Acute Pancreatitis Study Group. Minimally invasive “step-up approach” versus maximal necrosectomy in patients with acute necrotizing pancreatitis (PANTER trial): Design and rationale of a randomized controlled multicenter trial [ISRCTN13975868]. BMC Surg 2006;6:6.
The initial PANTER trial compared open necrosectomy, a therapy with a well-documented high rate of complications, with the step-up approach. Because a promising minimally invasive alternative to the step-up approach is endoscopic transgastric necrosectomy, a randomized controlled trial (PENGUIN, Primary Necrosectomy in Patients With Infected Necrosis) examined endoscopic transgastric versus surgical necrosectomy in patients with infected pancreatic necrosis. Endoscopic transgastric necrosectomy was associated with a reduced inflammatory response as measured by serum interleukin (IL)-6 concentration and reduced composite end point of major complications (new-onset multiple organ dysfunction syndrome, intra-abdominal bleeding, enterocutaneous fistula, pancreatic fistula, or death [20% vs. 80%, p=0.03]), but the sample size was small (n=20) [86].
The endoscopic technique can also be applied in a step-up manner, consisting of endoscopic transluminal drainage followed, if necessary, by DEN for treatment of infected necrotizing pancreatitis. Comparison of the transluminal endoscopic step-up to the minimally invasive surgical step-up approach has been achieved with the recent completion of the TENSION trial. This trial is a randomized controlled parallel-group superiority multi-center trial that randomly assigned patients to either endoscopic or surgical step-up, with the hypothesis that the endoscopic approach would have a lower primary end point of mortality and major complication. Publication of results of this trial are still pending [87].
Optimal Necrotizing Pancreatitis Management: Staged Minimally Invasive Multidisciplinary Step-Up Approach
Based on the evidence available to date, patients with necrotizing pancreatitis require an individualized multi-disciplinary management approach for optimal treatment to achieve the best outcomes, reduce mortality, and prevent associated complications. Modern treatments for necrotizing pancreatitis, debridement, or necrosectomy have evolved into minimally invasive options (VARD, MIRP or DEN) rather than open surgical necrosectomy [88]. Current evidence-based treatment includes an initial step of drainage (either percutaneous catheter or transluminal endoscopic) and then frequent re-evaluation of the clinical success of this approach. Surgical or endoscopic transluminal debridement is now only required with lack of clinical resolution and is delayed until necrosis has become “walled off” (WOPN) [89]. Overall, considering the growing evidence to support minimally invasive techniques and delaying or even avoiding major surgical procedures with this algorithm, the step-up endoscopic and surgical approach is emerging as the standard of care in the appropriate necrotizing pancreatitis patient. Both endoscopic transluminal drainage and minimally invasive necrosectomy have emerged as secondary techniques for treating infected pancreatic necrosis after initial percutaneous catheter drainage or endoscopic transgastric or transduodenal drainage. Optimal treatment of necrotizing pancreatitis now requires a staged multi-disciplinary minimally invasive step-up approach that includes a team of interventional radiologists, therapeutic endoscopists, and surgeons.
Footnotes
Author Disclosure Statement
No competing financial interests exist.