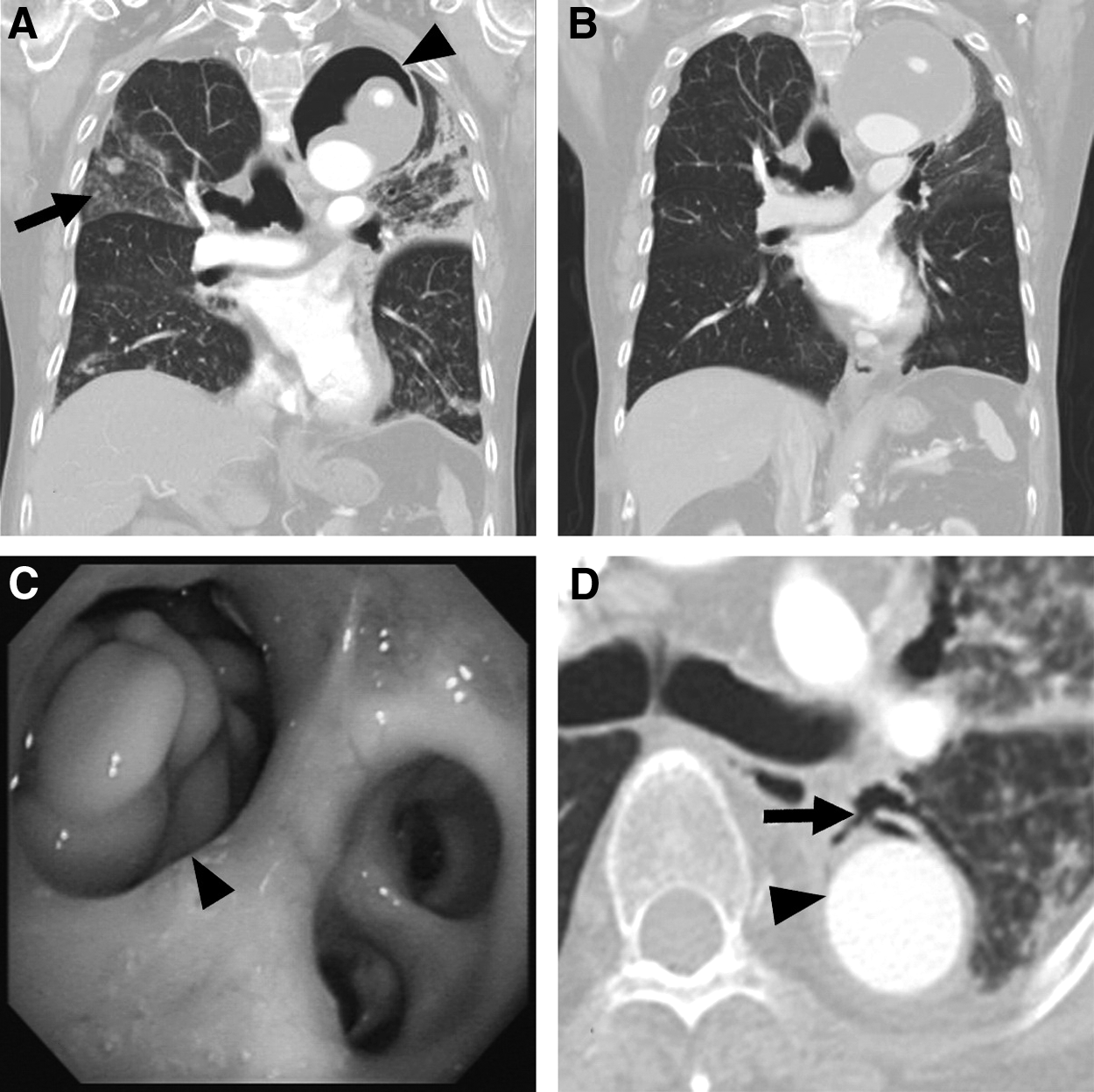
An 83-year-old male presented with blood-tinged sputum and 2-mo recurrent fever. He had hypertension and a Stanford type A aortic dissection that had been repaired by a Dacron® (Maquet, Rastatt, Germany) aortic graft repair operation 5 y prior. Chest radiograph and computed tomography (CT) scan revealed multiple pulmonary infiltrates and a giant cavity abutting the aortic graft (Fig. 1A) that had been absent on a previous CT conducted 1 y prior (Fig. 1B). The giant cavity was formed by an eroding thrombus and air (Fig. 1A). Fiberoptic bronchoscopy revealed a perforation in the apical segmental bronchus of the left lower lobe (Fig. 1C). The bronchoscope tip entered an empty space filled with whitish caseous tissue through the bronchial perforation. The bronchial perforation was observed to be connected to adjacent aortic graft on the chest CT scan (Fig. 1D). A Grocott-Gomori methenamine silver stain of the biopsy specimen obtained from caseous material beneath the bronchial perforation exhibited numerous septated hyphae. Positive Aspergillus flavus and Mycobacterium tuberculosis cultures were identified in sputum and bronchoalveolar lavage fluid but not in the blood. A culture of the biopsy specimen isolated only A. flavus. Polymerase chain reaction for identifying M. tuberculosis complex in the biopsy specimen yielded a negative result. In addition to active pulmonary tuberculosis, invasive pulmonary aspergillosis associated with an aortic graft infection was diagnosed. The patient exhibited clinical stability with prolonged anti-fungal and anti-tuberculous treatment. However, he died from aspiration pneumonia with respiratory failure 2 mo later.
(A) Chest computed tomography (CT) showing a giant cavity (arrowhead) abutting the aortic graft and multiple pulmonary infiltrates (arrow). (B) Comparison of previous chest CT recorded 1 y prior. (C) Bronchoscopic image showing whitish caseous material beneath a bronchial perforation (arrowhead). (D) The bronchial perforation (arrow) was connected to the adjacent aortic graft (arrowhead).
Prosthetic vascular graft infection caused by Aspergillus species is a rare condition. Perigraft air, fluid, soft tissue attenuation, and pseudoaneurysm can be observed by CT scans of patients with aortic graft infection [1]. This patient exhibited an unusual presentation of a cavity within the pre-existing perigraft thrombus. The bronchial perforation, an unusual bronchoscopy finding, has never before been observed in patients with invasive pulmonary aspergillosis [2]. Most cases of vascular graft infection caused by Aspergillus species are believed to originate from contamination by fungal spores during surgery [3–5]. However, surgical contamination was implausible in this patient because its onset was 5 y after surgery. Because Aspergillus species are angioinvasive, the patient could have had a bronchopleural fistula initially and developed the adjacent aortic graft infection subsequently caused by pulmonary aspergillosis. The unique radiologic findings observed in this patient provide new understanding for disease manifestations of invasive pulmonary aspergillosis.
Footnotes
Acknowledgments
H.C.L. and M.C.L. provided direct patient care. W.L.L. made the pathologic diagnosis. All authors wrote the report. Written consent for publication was obtained.
References
1.
OrtonDF, LeVeenRF, SaighJA, et al.Aortic prosthetic graft infections: Radiologic manifestations and implications for management. Radiographics, 2000; 20:977–993.
FusterRG, ClaraA, di StefanoS, et al.An unusual vascular graft infection by Aspergillus—A case report and literature review. Angiology, 1999; 50:169–173.
4.
CollazosJ, MayoJ, MartinezE, IbarraS. Prosthetic vascular graft infection due to Aspergillus species: Case report and literature review. Eur J Clin Microbiol Infect Dis, 2001; 20:414–417.
5.
PatersonDL. New clinical presentations of invasive aspergillosis in non-conventional hosts. Clin Microbiol Infect, 2004; 10(Suppl 1):24–30.