
Abstract
Abstract
Background:
Choice of empiric antibiotic(s) for early ventilator associated pneumonia (VAP) involves weighing the risks of potential infection with multi-drug resistant (MDR) pathogens against those of over-exposure to broad-spectrum agents. Although early VAP is believed to be rarely caused by MDR pathogens, the overall incidence of all methicillin resistant Staphylococcus aureus (MRSA) infections is increasing. We questioned if MRSA VAP is becoming more common and if these infections were occurring earlier in the patient's hospital course. We hypothesized that 1) early (2–4 d from intubation) VAP caused by MRSA is relatively uncommon and 2) those patients with early VAP because of MRSA had risk factors associated with a MDR organism infection.
Methods:
Bronchoscopies with lavage (BALs) from patients admitted to our SICU from 2010–2013 were reviewed. MRSA VAP was defined as growth of ≥105 cfu/mL from BAL. Multi-drug resistant risk factors included a previous MRSA infection or positive nasal swab, antibiotic use within 90 d, hospitalization for >5 d, hemodialysis, homelessness, intravenous drug use, and men having sex with men.
Results:
In the 3-y period, there were 438 cases of VAP. Forty-seven specimens from 43 patients had quantitative microbiologic confirmation of MRSA VAP for an overall prevalence of 10.7%. Of patients with early VAP, three of 106 (2.8%) were MRSA positive. Culture results were graphed according to ventilator days (Fig. 1). The median days ventilated at the time of MRSA VAP were 8 d (range 2–81). All of the early MRSA VAP patients had identifiable risk factors for MRSA infection. The negative predictive value for patients not having a risk factor was one.
Conclusions:
These data suggest that the incidence of MRSA VAP is stable. Those patients with early MRSA VAP demonstrated traditional MDR risk factors. Patients without risk factors in the early time period could effectively be ruled out from having MRSA VAP and likely do not require empiric MRSA coverage.
V
Recent epidemiological data have demonstrated that the prevalence of community acquired MRSA (CA-MRSA) skin and soft tissue infections has increased precipitously, as much as doubling in the last decade [4–6]. Some communities have reported a prevalence of CA-MRSA as high as 25% [7]. Certain risk factors for acquiring MRSA colonization or infection have also been recognized and these high-risk patients receive a more aggressive empiric antibiotic regimen. Our institution reported an early MRSA VAP rate of 2.2% during the 4-y period of 2004–2007 [8]. However, recent reports have documented an increasing incidence of this pathogen in the early VAP window [5].
The finding of similar rates of MRSA VAP in the early as compared with the late window may have profound clinical ramifications in terms of adding empiric MRSA coverage to all patients with suspected early VAP. Identification of risk factors for early VAP because of MRSA could help mitigate this change in practice by targeting a smaller subgroup of individuals for empiric MRSA therapy. We hypothesized that, in our surgical ICU: 1) MRSA VAP is less common in the early window and 2) early VAP because of MRSA can be predicted by either admission nasal culture or risk factors associated with a multi-drug resistant (MDR) organism infection.
Patients and Methods
This was a retrospective review of Denver Health Medical Center surgical ICU patients selected for lower respiratory culture between 2010 and 2013. Denver Health Medical Center is a State Certified, American College of Surgeons Verified Level I trauma center. Patients were selected for lower respiratory culture at the discretion of the attending surgical intensivist and based upon clinical suspicion of pneumonia including fever, elevated white blood cell count or bandemia, change in oxygen requirements, new infiltrate on chest X-ray or purulent sputum. All specimens were collected using directed bronchoscopy with lavage (BAL) or blind catheter pass with lavage (mini BAL). Exclusion criteria were 1) non-surgical patient, 2) ventilated for <48 h at the time of lower respiratory tract culture, 3) respiratory culture of either sputum or tracheal aspirate, and 4) respiratory culture not analyzed quantitatively. VAP was defined as growth of ≥105 colony forming units (cfu)/mL on final culture. This threshold was lowered to ≥104 if the patient was receiving antibiotics to which the pathogen was sensitive at the time of the culture. Early VAP was defined as occurring 2–4 d from intubation. Nasal swabs were obtained routinely on all patients. Parameters abstracted included time of specimen from intubation, time of specimen from hospital day, organism type and risk factors for MRSA including: Antibiotic therapy within 90 d; hospitalization greater than 5 d; prior MRSA infection or positive nasal swab culture; institutionalization in a prison, nursing facility, or military complex; undergoing hemodialysis at the time of admission [3]; homelessness [9]; intravenous drug abuse; or men who have sex with men (MSM) [10,11]. These risk factors were then evaluated in the medical record.
Statistical analyses were performed using SAS version 9.1 (SAS Inc., Carey, NC). Data are expressed as median (range). Differences between medians of continuous variables were compared using the Wilcoxin Rank Sum test. Differences between categorical variables were compared using the Chi Squared Test. This study was approved by the Colorado Multi-institution review Board (COMIRB#13-3062).
Results
There were 1013 specimens that comprised the database; 438 cases of VAP were identified (43.2%). MRSA was identified as a pathogen in 47 of the 438 cases of VAP (10.7%). The four patients with two episodes of MRSA VAP occurred in the late group. Table 1 provides demographics on the MRSA cohort versus the non-MRSA cohort. Furthermore, 106 (24.2%) of the cases with VAP occurred in the early period, whereas 332 (75.8%) were late VAP. In the early cohort, 86 patients had trauma diagnoses (81.9%), whereas 20 were surgical ICU patients (18.9%). All of the early MRSA VAP patients were trauma patients. The majority of VAP diagnoses were obtained using a mini BAL technique (64/106 or 60.4%), whereas the remainder (42/106) were obtained using a BAL (39.6%). None of the early VAP patients had a previous diagnosis of pneumonia prior to the VAP diagnosis. There were three of 106 patients with early VAP that grew MRSA (2.8%), whereas 41 of 332 patients with late VAP grew MRSA (12.3%), (p < 0.01). Figure 1 illustrates the incidence of MRSA VAP by ventilator day and also provides the ratio of patients with MRSA risk factors. The median ventilator day for MRSA VAP was day eight. The data were distributed similarly when analyzed by number of hospital days and the median hospital day for MRSA VAP was found to be at day eight.
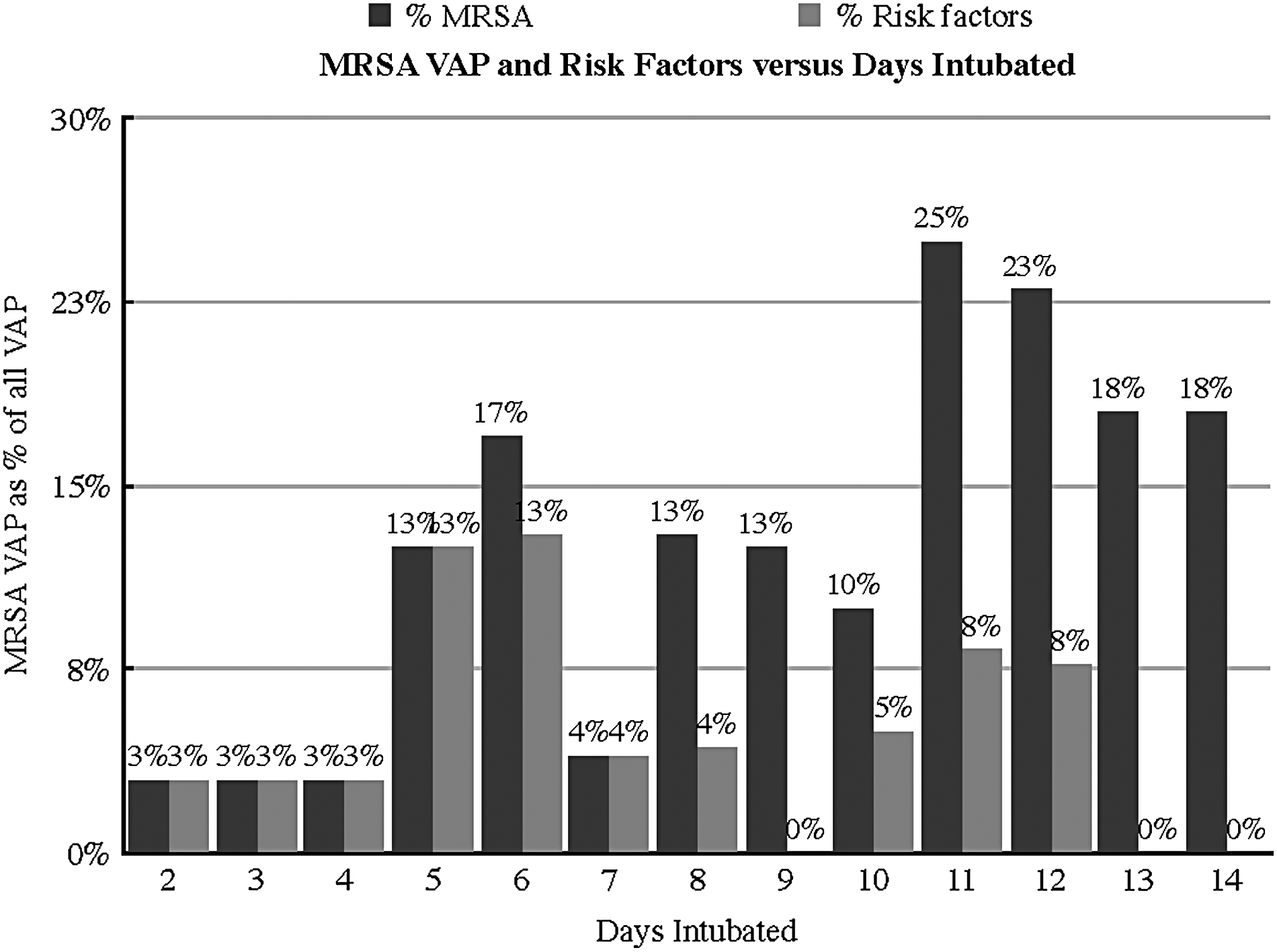
MRSA VAP incidence (dark gray) versus incidence of risk factors (light gray) as a percentage of all VAPs based on day of intubation.
MRSA = methicillin resistant Staphylococcus aureus; VAP = ventilator associated pneumonia; EGS = emergency general surgery; ICU = intensive care unit; LOS = length of stay.
When analyzed as a proportion of total early VAP, there was a substantial increase in the ratio of MRSA as a proportion of VAP starting at day five. Initially, the rate of MRSA was 2.8% (3/106) during days two to four and increased to almost 17% by day six (Fig. 1). Although there was one patient who developed MRSA VAP without risk factors on day six, the incidence of MRSA VAP in the absence of risk factors increased markedly on ventilator day eight.
Analysis of the patients with early VAP identified 32 patients with an MDR risk factor but developed an early VAP with an organism other than MRSA. Specifically, 15 patients (14.6%) were homeless, 14 (10.4%) used intravenous drugs, nine (8.7%) were institutionalized, three (2.9%) had a positive nasal swab, and two (1.9%) were undergoing hemodialysis. Nine patients had two or more risk factors. The sensitivity of having a positive MRSA risk factor was 100%, whereas the specificity was 68.6%. The positive predictive value (PPV) for a patient with an MRSA risk factor developing early MRSA pneumonia was low, at 8.6%. However, the negative predictive value (NPV) was strong at 100%, indicating patients without an MRSA risk factor were unlikely to develop MRSA pneumonia. Similarly, the positive likelihood ratio of 3.2 and the negative likelihood ratio of 0.0 are consistent with the chosen risk factors for MRSA VAP being an excellent screening tool (Table 2).
MRSA = methicillin resistant Staphylococcus aureus; VAP = ventilator associated pneumonia; PPV = positive predictive value; NPV = negative predictive value; LR = likelihood ratio; sens = sensitivity.
In further analysis of those with early MRSA VAP, we found that those three of three (100%) who developed MRSA VAP had a positive risk factor (Table 3). In terms of risk factors, two patients had a positive nasal swab (66.7%), one patient used intravenous drugs (33.3%), and one patient was homeless. One of the three patients had two risk factors.
Note one patient had two positive risk factors
MRSA = methicillin resistant Staphylococcus aureus; VAP = ventilator associated pneumonia; MSM = men who have sex with men.
Discussion
Our data demonstrate a rate of early MRSA VAP that is lower to that quoted in previous literature. Our rate of early MRSA VAP was 2.4%, within the previously reported rates ranging from 2.2% [8] to 24.5% [7] and close to the most recent report of 4.7% [12]. This data supports our hypothesis that the prevalence of MRSA in our trauma and surgical ICU population is not increasing.
We found that the incidence of MRSA VAP increased markedly starting at day five from intubation. This increase correlates with the transition from early to late VAP. However, the all patients except one between d 5 through d 7 continue to have risk factors for MRSA and therefore the increased MRSA VAP rate is predictable. After d 7, the rate of MRSA VAP in the absence of risk factors increases dramatically. In determining the best time period to broaden empiric antibiotic therapy to include MRSA coverage in the absence of risk factors, our data would suggest the optimal timing would be after d 7. At this point, only one patient would not receive empiric coverage who required it, whereas 62 patients would receive unnecessary MRSA coverage.
To help identify those patients who are at elevated risk of developing early MRSA VAP, we confirmed that the prescribed risk factors are accurate in predicting those who will develop MRSA VAP. Homelessness, intravenous drug use, and positive screening swab were present in our cohort of early MRSA VAP patients. Our data support our hypothesis that the absence of established MRSA risk factors effectively ruled out early MRSA VAP. We recommend screening practices be in place to help identify these high-risk patients so that patients without risk factors are spared the potential effects of unnecessarily broad antibiotic therapy.
Our study has several limitations, including the limitations of using a retrospective database. In particular, the risk factors that were examined may not have been complete. The chart review may not have identified less common risk factors, such as membership on a sports team or other clustering that would confer an increased risk of MRSA. Finally, the cohort of patients with early MRSA VAP was small (n = 3) and so conclusions about this group should be tempered.
In conclusion, our data indicate a stable rate of early MRSA VAP from prior studies. Additionally, we found that patients at high risk for early MRSA VAP could be successfully identified using MDR risk factors and MRSA swab data. We recommend starting empiric MRSA coverage after day seven for patients without risk factors or empirically upon suspicion of VAP in patients with recognized risk factors in the early window.
Footnotes
Author Disclosure Statement
The authors do not have any financial disclosures to declare.