
Abstract

A43-
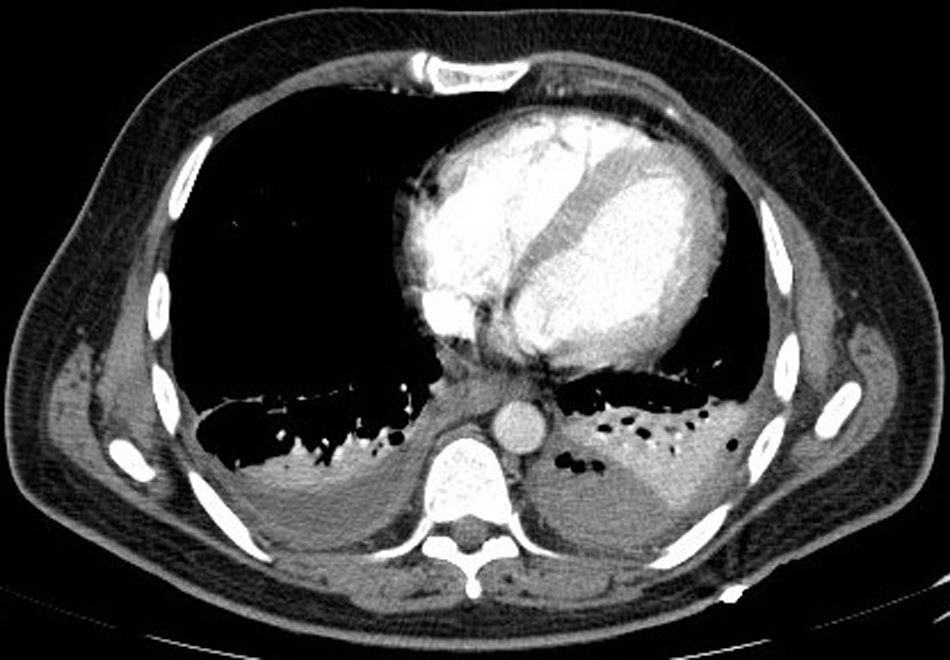
Computed tomography scan of the chest documenting a left-sided organized pyothorax.

Fluoroscopic imaging and drainage of the pleural empyema.
Blunt traumatic esophageal perforation is a rare event: approximately only 100 cases have been described as of 2013 [1]. The pathogenetic mechanism underlying this type of injury is still unclear: sudden increase of intra-esophageal pressure against a closed glottis, excessive traction secondary to uncoordinated hyperextension of the neck, compression exerted by associated cervical fractures, and blast effect combined with a tracheal injury represent the most accredited determinants [2]. This is a life-threatening condition in which morbidity and mortality remain high because of the spread of gastrointestinal content (fluid and bacteria) to the para-esophageal spaces and delays in diagnosis and treatment [2,3]. On the one hand, if pleura is intact, the discharge collects within the mediastinum where it triggers chemical inflammation along with bacterial infection (mediastinitis); on the other hand, when there is a concomitant pleural injury, it can flow into the pleural space and result in empyema thoracis, as found prior to our case [3]. The correlation between esophageal perforation and subsequent pleural empyema fed by strains of the genus Bacillus is exceptional, as only one description is present in the current literature dealing with Bacillus licheniformis and Bacillus subtilis [4]. Such a rarity is mostly because, except for Bacillus anthracis and Bacillus cereus, the other species of these aerobic gram-positive bacteria are normally non-pathogenic for the gut and skin of human beings [4]. Bacillus lentus also belongs to this group: to date, the only confirmed human infection caused by this germ is keratitis [5].