
Abstract
Abstract
Background:
Hysterectomy is one of the most common procedures performed in the United States. New techniques utilizing laparoscopic and robotic technology are becoming increasingly common. It is unknown if these minimally invasive surgical techniques alter the risk of surgical site infections (SSI).
Methods:
We performed a retrospective review of all patients undergoing abdominal hysterectomy at our institution between January 2011 and June 2013. International Classification of Diseases, Ninth edition (ICD-9) codes and chart review were used to identify patients undergoing hysterectomy by open, laparoscopic, or robotic approach and to identify patients who developed SSI subsequently. Chi-square and analysis of variance (ANOVA) tests were used to identify univariate risk factors and logistic regression was used to perform multivariable analysis.
Results:
During this time period, 986 patients were identified who had undergone abdominal hysterectomy, with 433 receiving open technique (44%), 116 laparoscopic (12%), 407 robotic (41%), and 30 cases that were converted from minimally invasive to open (3%). Patients undergoing laparoscopic-assisted hysterectomy were significantly younger and had lower body mass index (BMI) and American Society of Anesthesiologists (ASA) scores than those undergoing open or robotic hysterectomy. There were no significant differences between patients undergoing open versus robotic hysterectomy. The post-operative hospital stay was significantly longer for open procedures compared with those using laparoscopic or robotic techniques (5.1, 1.7, and 1.6 d, respectively; p<0.0001). The overall rate of SSI after all hysterectomy procedures was 4.2%. More SSI occurred in open cases (6.5%) than laparoscopic (0%) or robotic (2.2%) (p<0.0001). Cases converted to open also had an increased rate of SSI (13.3%). In both univariate and multivariable analyses, open technique, wound class of III/IV, age greater than 75 y, and morbid obesity were all associated with increased risk of SSI.
Conclusion:
Laparoscopic and robotic hysterectomies were associated with a significantly lower risk of SSI and shorter hospital stays. Body mass index, advanced age, and wound class were also independent risk factors for SSI.
S
Hysterectomy is one of the most common surgical procedures performed in the United States; it is estimated that one in nine women will undergo hysterectomy in their lifetimes [4]. As with many surgical procedures, there has been an increasing trend toward minimally invasive techniques, including laparoscopic and robotic procedures. Numerous studies have been conducted comparing the safety and cost of open or minimally invasive procedures, however, there is a paucity of data studying the effect that these approaches have on rates of SSI after total abdominal hysterectomy. We hypothesized that hysterectomies performed with minimally invasive techniques would be associated with decreased SSI.
Patients and Methods
After approval by our Institutional Review Board, a retrospective review was performed on all patients undergoing hysterectomy at our institution between January 2011 and June 2013. International Classification of Disease-9 (ICD-9) codes were used to identify patients undergoing hysterectomy and chart review verified the procedures performed. Our hospital uses a protocolized SSI surveillance system to identify patients who develop SSI, with patients followed for 30 d post-operatively based on the U.S. Centers for Disease Control and Prevention (CDC) definition [5]. This system uses microbiology reports, physician surveys, SafetySurveillor® (Premier Inc., Charlotte, NC), an established software for surveillance of infections, referral calls from area hospitals, and ICD-9 codes reported by the hospital to identify SSI.
Demographic data were collected for all patients including: Patient age, gender, body mass index (BMI), wound class, the American Society of Anesthesiologists (ASA) score, procedure duration, whether the procedure was performed for a benign or malignant disease, hospital length of stay, and procedure technique (open, laparoscopic, robotic, or converted to open). Surgical site infections were categorized as superficial incisional, deep incisional, or organ/space infections. Culture results, if obtained, were recorded for each patient.
Statistical analysis was performed using SPSS (version 22, IBM Corp., Armonk, NY). Univariate analysis was performed to compare the rates of infection to demographics. Analysis of variance and χ2 tests were used to compare groups and identify univariate risk factors associated with development of SSI. Logistic regression was used to perform multivariable analysis. A p value of 0.05 or less was considered significant.
Results
Patient characteristics
A total of 986 patients underwent hysterectomy at our institution during the study period. Over this time, 44% of the hysterectomies were performed using an open technique, 41% using a robotic technique, 12% using laparoscopic technique, and 3% were converted from a minimally invasive technique to an open technique. The conversion rate for robotic approach was 4% (16/407 patients), which was significantly lower than the conversion rate of 12% (14 of 116 patients) for the laparoscopic approach (odds ratio [OR]: 0.29, 95% confidence interval [CI]: 0.16–0.65). Patients undergoing open hysterectomy and robotic hysterectomy had no significant differences in any of the evaluated patient characteristics (Table 1), whereas the patients undergoing laparoscopic procedures were significantly younger, with lower BMI, lower ASA scores, and fewer procedures performed for cancers than the patients undergoing open or robotic techniques.
p<0.05 compared with all other groups.
p<0.05 compared with robotic and laparoscopic techniques.
All variables are reported as the mean with standard deviation.
Patients undergoing open and robotic hysterectomy were similar. Patients undergoing laparoscopic hysterectomy were significantly younger, thinner, with lower ASA scores, and fewer procedures performed for oncologic reasons. Hospital length of stay was significantly shorter following robotic and laparoscopic hysterectomy.
BMI=body mass index; ASA=American Society of Anesthesiologists.
During the 3 y of study, the rate of open procedures steadily declined (Fig. 1). Procedure time was not different between open, robotic, or laparoscopic approaches, however, cases that required conversion to open technique were significantly longer. Procedure time did not differ over the years (Fig. 2), however, mean procedure time for both open and robotic techniques significantly decreased in 2013 compared with 2011 (141±87 min versus 185±125 for open; p=0.038; and 175±85 min versus 201±99 min for robotic; p=0.041). Hospital length of stay was significantly shorter in laparoscopic and robotic groups than in either group using an open approach.
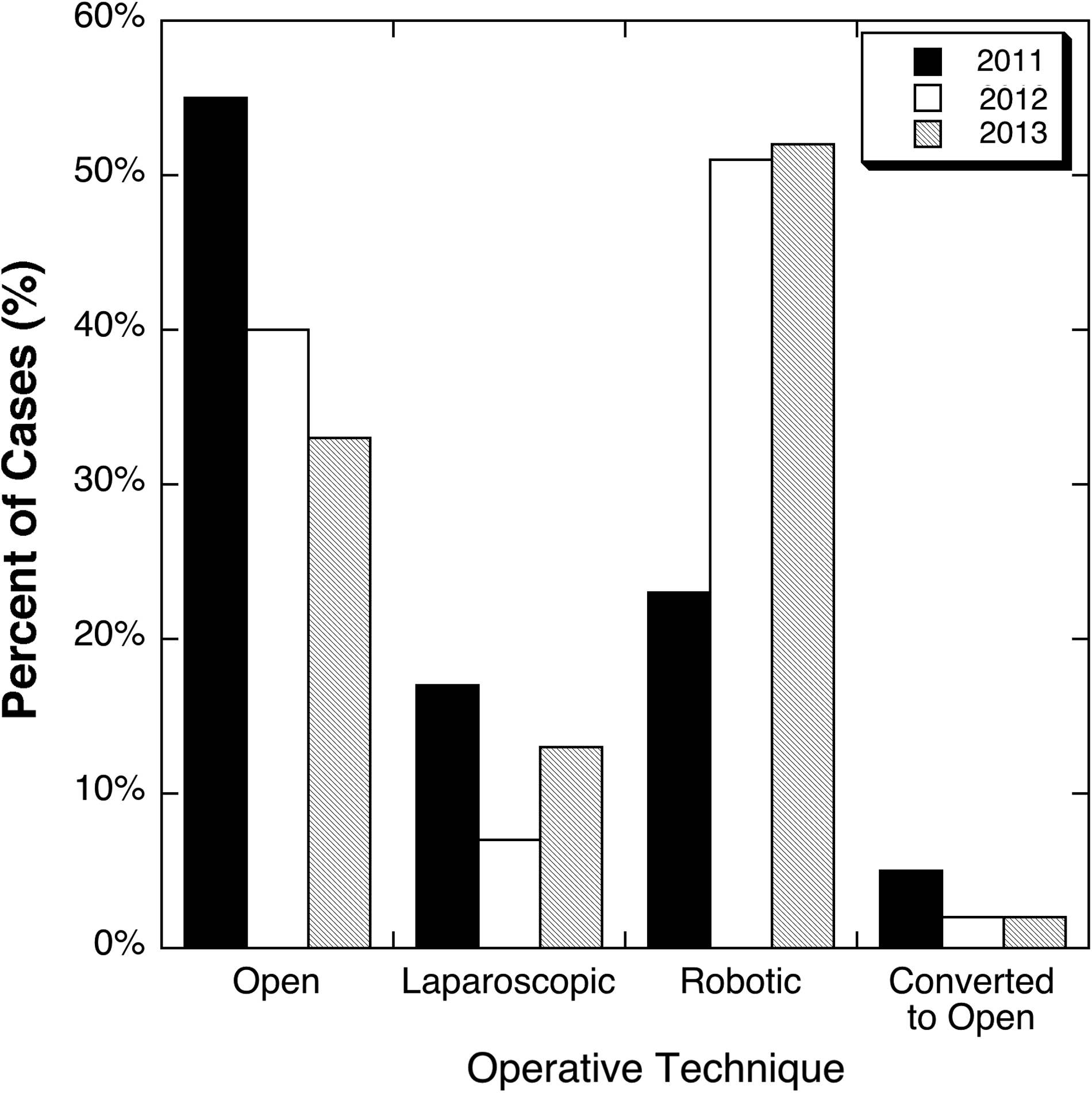
Operative technique by year. Open procedures declined over the 3-y study period, whereas robotic procedures increased.
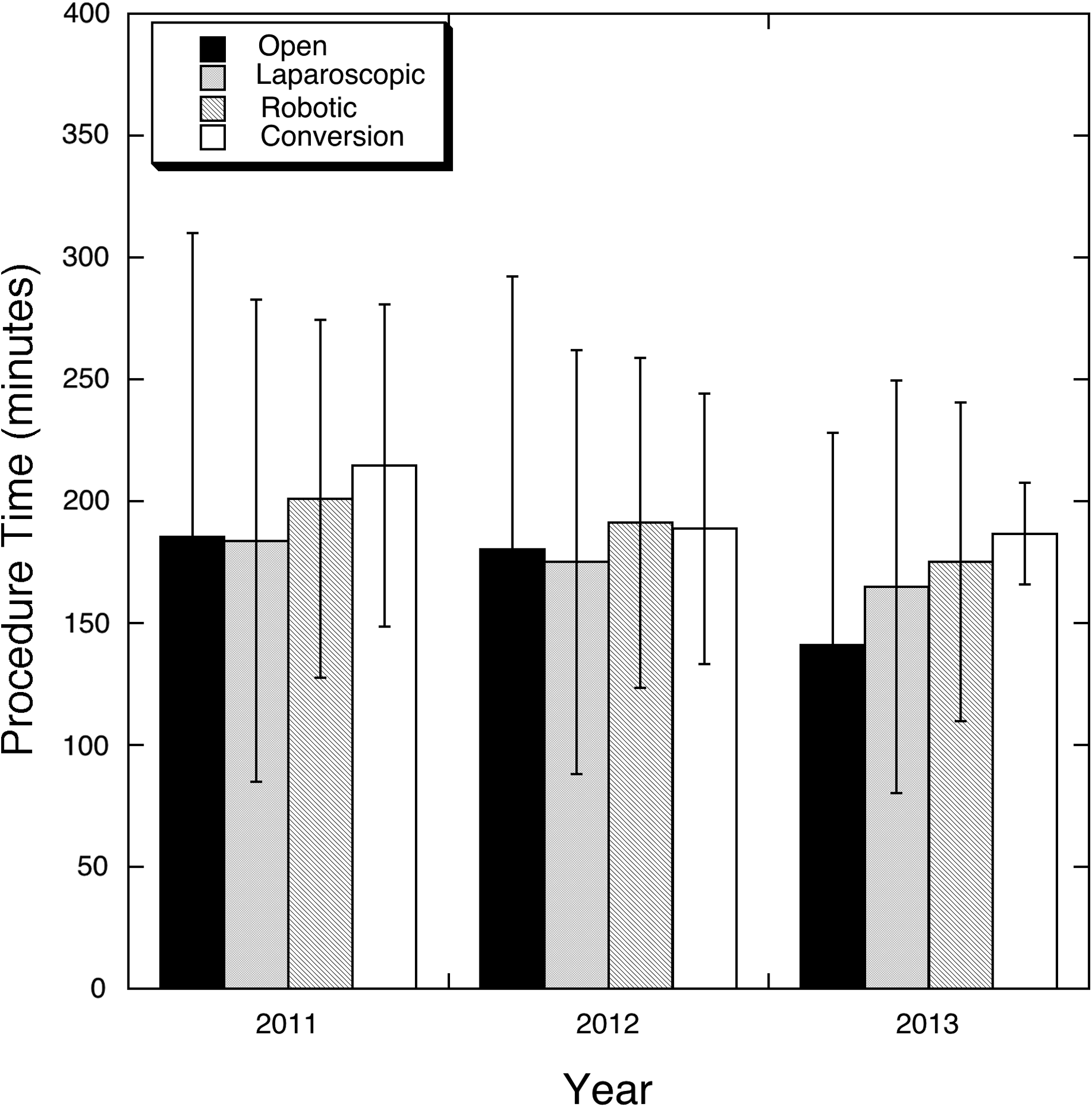
Procedure time for each operative technique by year. There were no differences in operative times between groups, however, both open and robotic procedure times were significantly shorter in 2013 compared with 2011 (p<0.05).
Surgical site infection risk factors
The rate of SSI was significantly lower in the robotic and laparoscopic groups than in the open or conversion groups (Fig. 3). The total rate of SSI in our cohort was 4.2% (41/986 patients). Superficial incisional SSI occurred at a rate of 2.5% (25/986), deep incisional 0.1% (1/987), and organ/space SSI 1.5% (15/986). By univariate analysis, SSI was associated with open technique, age greater than 75 y, BMI, ASA score≥3, wound class III or IV, and longer procedure times (Table 2). By multivariable analysis, open technique, BMI>40, age greater than 75 y, and wound class III or IV were found to be associated independently with the development of SSI after abdominal hysterectomy (Fig. 4). When multivariable analysis was performed comparing open and robotic techniques alone (i.e., removing the laparoscopic group with no infections and the conversion group), open technique remained independently associated with risk of SSI (adjusted odds ratio [aOR]: 3.5; 95% CI 1.5–11.2; p=0.005), as did wound class of III or IV (aOR: 4.9; 95% CI: 1.01–23.9), BMI>40 (aOR: 3.1; 95% CI: 1.4–7.2) and age greater than 75 y (aOR: 4.0; 95% CI: 1.4–11.2).

Rate of surgical site infection by operative technique. Robotic and laparoscopic techniques had fewer surgical site infections compared with open and converted cases (p<0.0001).
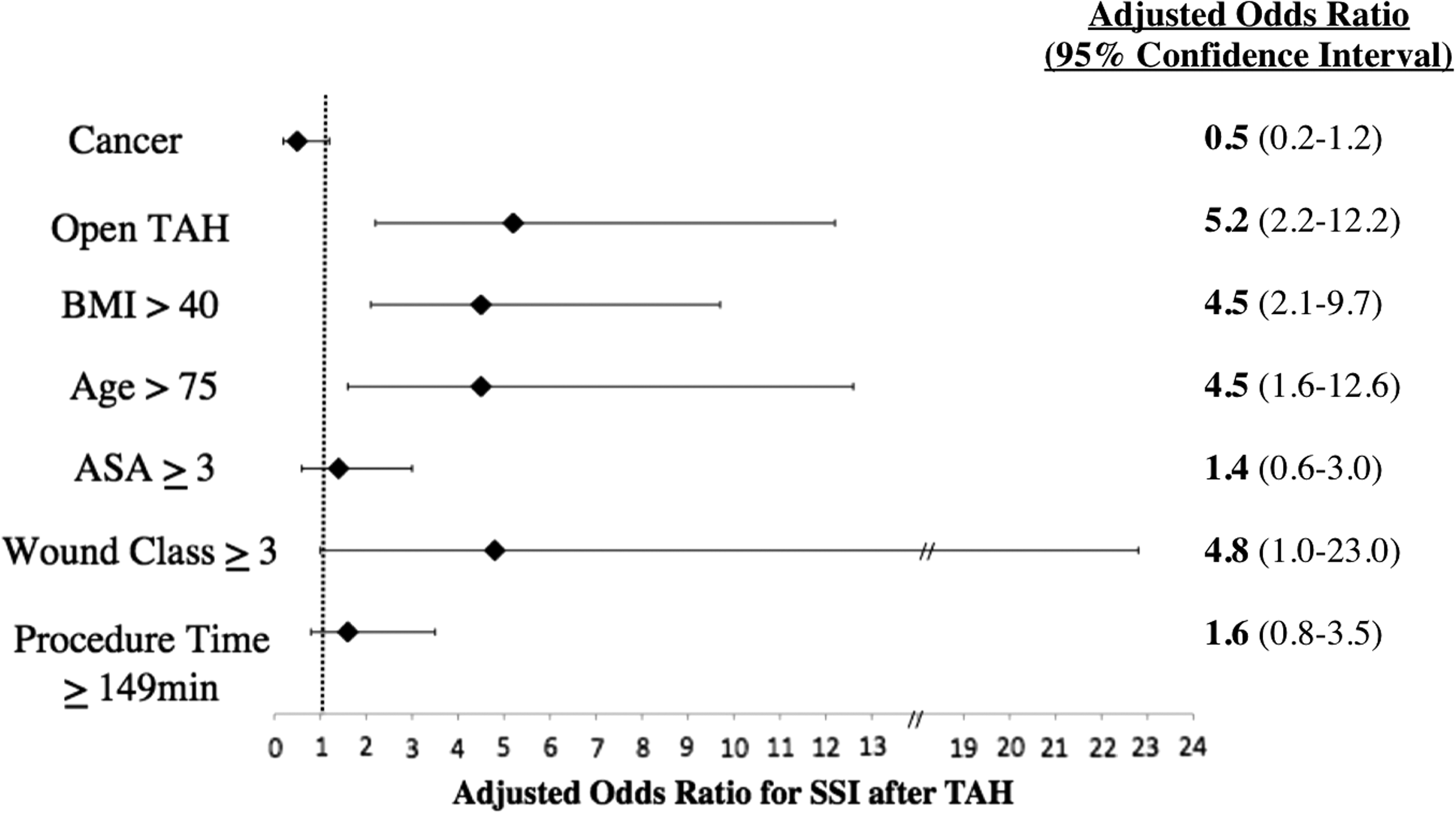
Adjusted odds ratios from multivariable analysis. Open procedures, body mass index (BMI)>40, age greater than 75 y, and wound class≥III were all associated independently with increased risk of surgical site infection (SSI). TAH, total abdominal hysterectomy; BMI, body mass index; ASA, American Society of Anesthesiologists.
SSI=surgical site infection; BMI=body mass index; ASA=American Society of Anesthesiologists.
The majority of these infections were superficial incisional SSI, with only 39% (16/41 SSI) being deep incisional or organ/space SSI. Superficial incisional SSI were significantly more common after open and converted procedures (21/433 [4.8%] in open and 3/30 [10%] in converted) compared with robotic cases (1/407 [0.3%]) (p<0.001). There was no significant difference in the rate of deep incisional or organ space SSI in open or minimally invasive techniques (7/433 [1.4%], 8/407 [2.0%], and 1/30 [3.3%] in open, robotic and converted cases, respectively; p=0.430). By multivariable regression, the only variable that was found to be associated independently with development of a deep or organ space SSI was a wound class of III or IV (OR 21.47; 95% CI 3.5–130).
Bacteriologic data
Approximately one-half of the superficial incisional SSI had culture data available (15/25 superficial SSI did not have cultures performed), whereas all deep and organ space infections had culture data available (16/16). Gram-positive bacteria were the most common isolates (Table 3). We had low rates of Staphylococcus aureus infections, no methicillin-resistant infections, and only one drug-resistant pathogen identified (vancomycin-resistant Enterococcus). There was no statistical difference between bacterial isolates between procedure techniques (data not shown).
Robotic total abdominal hysterectomy only had one superficial SSI, which was not cultured. Pathogens isolated from deep/organ space SSI were not different between groups. There were 64 isolates in 26 SSI wound cultures performed. Five of the 12 superficial SSI grew more than one organism and nine of 16 deep and organ space SSI grew multiple organisms.
SSI=surgical site infections.
Discussion
We have shown that minimally invasive hysterectomy, both laparoscopic and robotic, was associated with significantly decreased rates of SSI. The overall rate of SSI in our cohort was 4.2% (2.6% superficial incisional, 0.01% deep incisional, and 1.5% organ space). Surgical site infections can be a devastating post-operative complication, leading to increased patient morbidity and mortality, as well as greater length of stay, hospital costs, and patient and physician dissatisfaction [5–9]. Preventing SSI is of utmost importance. Appropriate pre-operative antibiotic prophylaxis, glycemic control, aseptic technique, and appropriate pre-operative skin preparation are all evidence-based methods of preventing infections [5]. In many studies, minimally invasive techniques, thereby limiting the incision size and area of skin contamination, have been shown to decrease the rate of SSI [10,11]. In gynecologic surgery, the use of robotic technique are increasing [12], however, there is a paucity of data on how this surgical approach affects SSI rates.
Lake et al. [13] conducted a cross-sectional analysis of the all hysterectomies in the American College of Surgeons National Surgical Quality Improvement Program database and reported SSI rates of 2.7%: 1.6% superficial incisional and 1.1% deep incisional SSI. This study included all routes of hysterectomy, including vaginal, open, and laparoscopic but did not evaluate robotic technique. They reported an increased risk of SSI with open abdominal hysterectomy (aOR: 3.7), but no significant difference between laparoscopic and vaginal hysterectomy. Mu et al. [1] also reported an increased risk of SSI with open abdominal hysterectomy, however, the risk was only modestly increased (OR: 1.43; 95% CI 1.17–1.74).
In our study open hysterectomy was a significant independent risk factor for SSI (aOR: 3.5; 95% CI 1.5–11.2). Other independent risk factors in our cohort were morbid obesity (BMI>40), advanced age (>75 y), and dirty or contaminated wound classes, which are similar to risk factors reported by others [14–16]. In these studies, blood transfusion, diabetes mellitus, and smoking have also been identified as risk factors for SSI after hysterectomy. Because we did not have these data available to us, we cannot comment on these risk factors.
Similar to the review by Lake et al. [13], in our study open procedures had an increased rate of superficial SSI, however, there was no difference in organ/space infections with procedure technique. The only characteristic that was independently associated with organ/space infection in our cohort was wound class III or IV. This lack of association between organ/space infections is likely because minimally invasive techniques do not change the internal contamination but only decrease the surface area of skin contamination (10,11).
In addition to the decreased rate of SSI in our cohort, patients who underwent minimally invasive hysterectomies had shorter hospital stays compared with those undergoing open hysterectomies. This shorter hospital stay and faster recovery time is one of the major benefits of minimally invasive procedures [17–20]. Other benefits of robotic procedures compared with open procedures that are noted in the literature include decreased blood loss, faster post-operative mobilization, and better visualization, especially for pelvic procedures [17–25]. Compared with laparoscopy, robotic operative times, lymph node recovery, and surgeon learning curve and dexterity have been reported to be improved [19,23,26–32].
As gynecologists become more comfortable with the procedure, the rate of robotic hysterectomy is increasing and procedure time is decreasing [12,24,28]. As has been noted in other studies [33], we found that conversion rates for robotic cases were lower than for laparoscopic procedures. In our cohort, the patients selected to undergo laparoscopic hysterectomy were younger, thinner, and healthier, whereas robotic technique was performed on a similar patient population as the open group. Despite the robotic patient population having higher BMI, suggesting that the procedures performed robotically may be more technically involved and difficult, more robotic cases were completed successfully and minimally invasively compared with the laparoscopic group.
Although not an outcome we initially sought to evaluate, we observed low rates of S. aureus and drug-resistant organisms in our series. We had only one case of S. aureus (1/41 SSI; 2.4%), no cases of methicillin-resistant S. aureus (MRSA), and one case of vancomycin-resistant Enterococcus. Staphylococcus aureus is reported to be the most common pathogen isolated from SSI and in 2008 the CDC reported that S. aureus was isolated from approximately one-third of all gynecologic SSI [34]. Surgical site infections caused by MRSA and other drug-resistant organisms increase morbidity and mortality as well as treatment costs [34]. Our hospital has a system-wide policy requiring patients to have a pre-operative shower or bath with chlorhexidine antiseptic soap. All patients are reminded with a call from the pre-operative nurse the night prior to their procedure. We have demonstrated that this protocol decreases SSI caused by S. aureus and MRSA [35].
Our findings should be interpreted with the following limitations in mind. This is a retrospective review and a single institution study performed at large academic hospital. The analysis of patient demographics associated with risk of SSI was limited, in that our patient database does not include smoking status, diabetes mellitus and other comorbidities, or intra-operative blood loss or transfusion requirements. As such, we were unable to assess how these factors may have contributed to SSI. We chose not to evaluate patients who underwent vaginal hysterectomy because this procedure is reported to have a lower SSI rate, and the patient population undergoing vaginal hysterectomy often varies greatly from those undergoing robotic, laparoscopic, or open techniques (e.g., large uterine weights, extensive oncologic procedures).
In conclusion, minimally invasive hysterectomy is associated with a lower rate of SSI compared with open procedures. Both robotic and laparoscopic approaches led to shorter hospital stays compared with open procedures. Robotic cases were less likely to be converted to open procedure than laparoscopic. In addition to open technique, we identified age greater than 75 y, wound class III or IV, and BMI greater than 40 kg/m2 as independent risk factors for the development of SSI after abdominal hysterectomy. Further study needs to be done to delineate which procedures and patients derive the most benefit from robotic assistance and the cost effectiveness of this technique.
Footnotes
Acknowledgment
Second place award for Best Poster Presentation at the Surgical Infection Society Annual Meeting, Baltimore, Maryland, May 2014.
Author Disclosure Statement
No competing financial interests exist.