
Abstract
Abstract
Background:
A prospective, single center, open-label study was conducted to determine if the standard practice for surgical prophylaxis, which includes standardized dosing of cefazolin, at the University of Maryland Medical Center (UMMC) is adequate for patients placed on bypass during cardiac surgery.
Methods:
All patients were given the same standard dosing regimen regardless of weight: two grams of cefazolin administered within 1 h of incision, an additional one gram injected into the bypass circuit at the onset of bypass, and two grams every 3 h after the initial dose. Cefazolin serum concentrations were collected immediately after incision, after the start of bypass, each hour of bypass, at the end of bypass and at sternal closure.
Results:
Ten patients were consented and completed the study with an average age of 62 y, average weight of 84.7 kg and average cardiopulmonary bypass time of 116 min. The free serum concentrations of cefazolin stayed above the pre-defined inhibitory threshold of 16 mcg/mL throughout the procedure for 100% of participants. The mean total serum concentration in the blood throughout surgery was 160 mcg/mL. No patients were found to have surgical site infections using standard criteria and no adverse events were observed.
Conclusions:
For patients undergoing cardiac surgery with cardiopulmonary bypass, the UMMC dosing regimen surpassed targeted cefazolin concentrations during the entire surgical procedure for all patients regardless of weight or time on bypass.
S
Cefazolin is the standard drug of choice for antibiotic prophylaxis in elective cardiac surgery based on spectrum of activity against common organisms responsible for infection as well as a favorable side effect profile. In order to be most effective, the antibiotic should achieve a concentration above the minimum inhibitor concentration (MIC) for the targeted organisms (e.g., Staphylococcus aureus, Staphylococcus epidermidis, Enterobacteriaceae, and Streptococcus spp.) for the duration of the procedure [5]. Cefazolin, like other beta-lactam antibiotics, is a time-dependent antibacterial, meaning that the length of time the concentration of drug remains above the MIC, rather than the relation of drug concentration to the MIC dictates killing ability [6].
Drug concentrations may be altered during cardiopulmonary bypass (CPB). When considering the implications for antimicrobial prophylaxis, unanticipated reductions in drug concentrations may produce exposures that are below targeted inhibitory values and may therefore put patients at an increased risk for post-operative infection of the surgical site. This phenomenon of altered concentrations is hypothesized to be the composite result of hemodilution, protein binding changes, or sequestration of drug by the cardiopulmonary bypass tubing [7]. The effect of cardiopulmonary bypass on the pharmacokinetic profile of cefazolin is not well understood, however, it is well recognized that insufficient concentrations will place the patient at a higher risk for developing surgical site infections [8,10]. Furthermore, current guidelines acknowledge a lack of evidence in this area and do not provide specific guidance on dosing during cardiopulmonary bypass [9].
This purpose of this study was to determine if utilizing a two gram dose of cefazolin and re-dosing during cardiopulmonary bypass is adequate to maintain free cefazolin concentrations above the MIC throughout the surgical procedure.
Patients and Methods
This was a prospective, open label study of cefazolin serum concentrations in adult patients who underwent a coronary artery bypass graft procedure in which they would be placed on cardiopulmonary bypass and receive cefazolin for surgical prophylaxis. Patients who were already scheduled for bypass surgery were approached for consent sequentially on study days. Patients were excluded if they were already on therapeutic cefazolin prior to surgery or if they had a creatinine clearance less than 35 mL/min. This study was approved by the University of Maryland Institutional Review Board.
Study participants received the standard dosing protocol at the University of Maryland Medical Center: Two grams of cefazolin administered within 1 h of incision, an additional one gram injected into the bypass circuit at the onset of bypass, and two grams every 3 h after the initial dose. The cefazolin placed in the bypass circuit was injected into the tubing of the circuit so that when bypass was initiated, the dose was delivered directly to the patient. The bypass circuit used was a Sorin S3 and S5 heart lung machine with an Apex oxygenator. The two gram dose of cefazolin was chosen to comply with current guidelines for surgical prophylaxis [9].
Blood samples were obtained immediately after incision, 10 min after the start of bypass, each hour of bypass, at the end of bypass, and at sternal closure. Blood samples for cefazolin concentrations (5 mL) were collected using red top tubes directly from the bypass circuit when the patient was on bypass and from a central venous catheter when the patient was not on bypass. Blood samples were centrifuged and serum was frozen to −80°C before analysis.
The biologically active free drug concentrations of cefazolin were determined for each patient using the ultracentrifugation technique. In attempt to generate the most robust estimates of protein binding with limited sample volume, three separate samples from each patient were combined. Three aliquots of serum were preserved for the determination of total drug concentration and three additional 0.9 mL samples of serum were transferred into three individual ultrafiltration devices (Centrifuge Centrifugal Filters, Millipore Corporation, Billerica, MA) with a molecular weight cutoff of 30 kDa and centrifuged at 2,000 × g using a fixed angle roto for 45 min at 10°C to obtain the ultrafiltrate (free drug matrix). The total and free protein binding determinations were conducted in triplicate. Cefazolin concentrations in serum and ultrafiltrate were determined using a previously validated HPLC method [11].
Because a concentration of 16 mcg/mL is the highest value considered susceptible for the organisms commonly implicated in surgical site infections in the cefazolin package insert, this value was defined as the target value for the adequacy of this prophylactic regimen [20]. If concentrations exceeded 16 mcg/mL, the regimen was deemed to be adequate prophylaxis for the pathogens of concern.
Results
Ten patients consented for participation and completed the study. The average age of participants was 62 y, average weight 84.7 kg and average cardiopulmonary bypass time 116 min (Table 1). All patients received cefazolin prophylaxis according to protocol with respect to agent, dose and time.
The cefazolin total serum concentration time profile of individual participants is depicted in Figure 1.
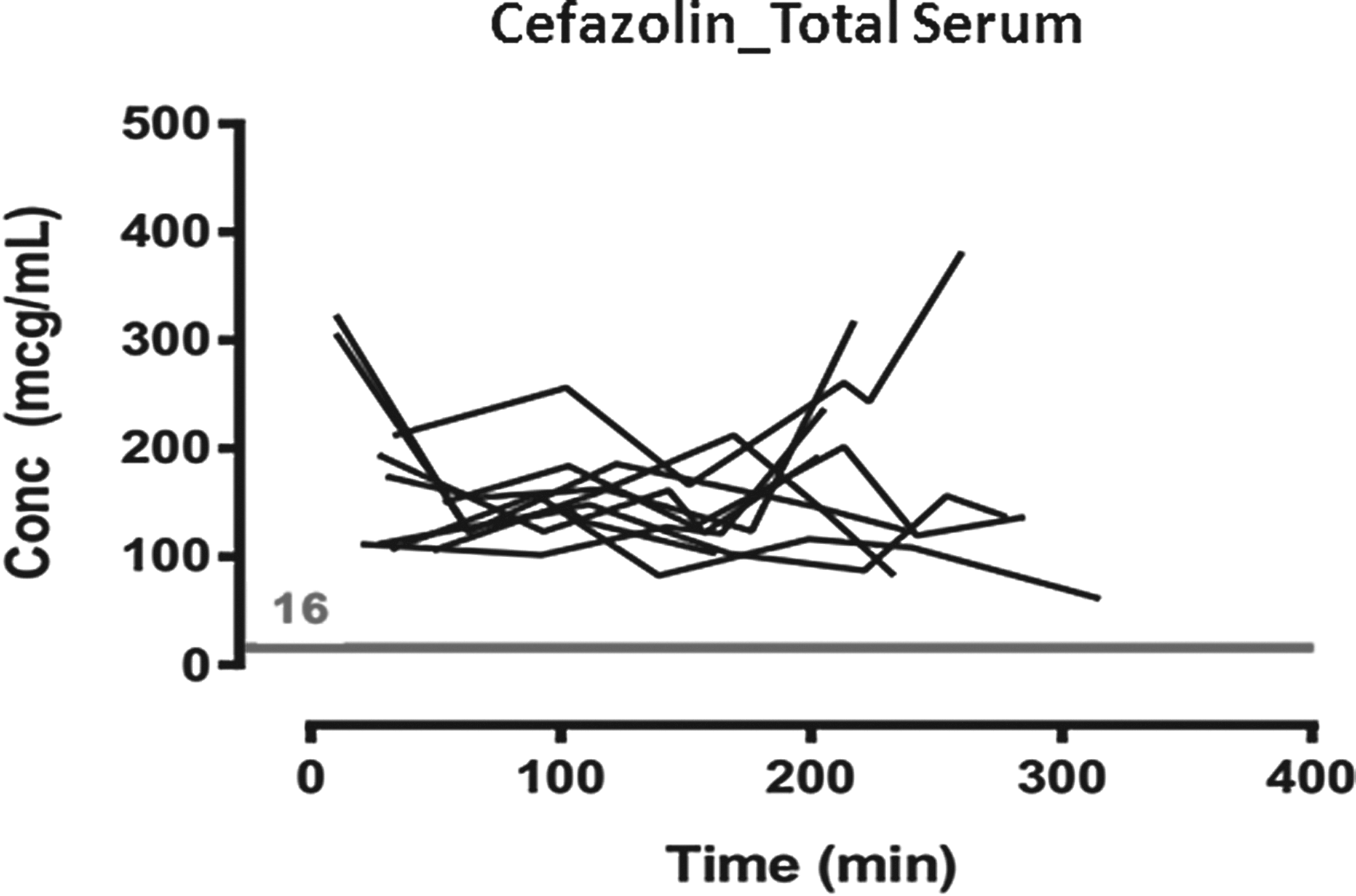
Cefazolin total serum concentration (Cp) time profile for all 10 participants. Each line represents a patient's total cefazolin concentration during the surgical procedure. A Cp of 16 mcg/mL or greater was considered to be inhibitory for organisms commonly implicated in surgical site infections.
The average cefazolin concentration in the blood at each collection time is shown in Table 2. The mean total concentration in the blood throughout surgery was 160 mcg/mL. The protein binding of cefazolin in this surgical population ranged from 53 to 75%, which produced free cefazolin concentrations ranging from 25 to 150 mcg/mL. Free serum concentrations of cefazolin stayed above the target value of 16 mcg/mL throughout the procedure for 100% of the study population. When drawn after the initiation of bypass, half the patients studied had a higher cefazolin serum concentration than at the time of incision (Appendix 1). Three patient's serum concentration remained relatively the same after the initiation of bypass and two patients had a large drop in cefazolin serum concentration. The average amount of CellSaver and plasmalyte given was 700 mL and 2500mL, respectively (Table 3). One study patient required less fluid resuscitation than others with 900 mL of plasmalyte whereas another patient had a higher CellSaver of 1400 mL. No adverse reactions to cefazolin were noted. No patients were found to have surgical site infections within 30 d of procedure according to the CDC/NHSN criteria [12].
FFP = fresh frozen plasma; PRBC = packed red blood cells.
Comment
We found that administering two grams prior to incision, one gram directly into the bypass circuit and two grams redosed every 3 h achieved more than adequate free serum concentrations throughout the entire surgical procedure for patients undergoing cardiac bypass surgery.
Current Infectious Disease Society of America/American Society of Health-System Pharmacist guidelines for thoracic and cardiovascular surgery recommend two grams of cefazolin be administered within 60 min of surgical incision, then redosing with two grams every 3 h for the duration of the procedure. The recently updated guidelines also recommend that a dose of three grams of cefazolin be considered if the patient is greater than 120 kg [9].
The standard protocol for surgical prophylaxis in cardiac surgery patients at UMMC is two grams of cefazolin administered within 1 h of incision, an additional one gram injected into the bypass circuit at the onset of bypass, and two grams every 3 h after the initial dose. It was hypothesized that administering one gram of cefazolin into the bypass circuit, serum cefazolin concentrations would not drop at the onset of bypass and by redosing of cefazolin with two grams every 3 h, serum concentrations would not drop below the cefazolin breakpoint as has been shown in previous studies [8,18].
In the current study, we observed that both the total and free drug concentrations exceed the MIC90 of cefazolin by three to four times [13]. As a result, this regimen provided cefazolin exposures well above the quoted pharmacodynamic target of concentration above the minimal inhibitory concentration (MIC) for at least 60% of the dosing interval [14]. This dosing regimen provided a cefazolin concentration above the MIC for 100% of the dosing interval.
Whereas cefazolin displays linear protein binding of approximately 80% as per the package insert, the protein binding values as determined in our patients were lower, thus our population displayed higher free drug concentrations that further exceeded the target MIC. A recent study by Bhalodi and colleagues showed that free cefazolin concentrations distributed adequately from serum into tissue, with a mean penetration ratio of 1.2. Tissue concentrations remained above 1 mcg/mL for 60% of the dosing interval for one patient and for 100% of the dosing interval for five patients receiving 1 g every 8 h [22]. This data suggests that the tissue concentrations in our patient population would be well above the MIC goal to prevent surgical site infections.
There is limited data on the dosing of cefazolin for surgical prophylaxis patients who are placed on cardiopulmonary bypass and currently no documented research on redosing these patients throughout the procedure using two grams of cefazolin. Most data consists of cefazolin one g given at the onset of anesthesia, then redosing with one g of cefazolin after the start of cardiopulmonary bypass or after the conclusion of bypass. This redosing strategy results in total serum concentrations lower than the MIC for a portion of the time on bypass [8,10,18]. A study by Adembri et al. showed that giving a two g bolus of cefazolin for prophylaxis prior to surgery increases the serum cefazolin concentration in the blood [10]. In a study of 10 patients undergoing cardiopulmonary bypass who received one g cefazolin administered at induction of anesthesia and repeated at surgical incision closure, plasma concentrations were lower than eight mcg/mL (sensitivity threshold of Staphylococcus aureus for cefazolin) in 50% of patients undergoing cardiopulmonary bypass for longer than 120 min [8]. This current study showed that by giving patients two grams prior to incision and redosing with two grams every 3 h, even patients who were on bypass greater than 120 min were able to achieve concentrations over the MIC for the entire procedure.
The above studies utilized a MIC breakpoint of eight mcg/mL based off of CLSI guidelines at the time the studies took place. Since those studies have been published, CLSI has removed breakpoints for cefazolin in Staphylococcus and suggested using oxacillin as a surrogate marker [19]. We chose to use 16 mcg/mL based on the cefazolin package insert [20]. Additionally, new data from a surveillance study indicate even lower susceptibility thresholds, further solidifying that we have achieved adequate concentrations [21].
There is currently no data on injecting cefazolin into the bypass circuit during the procedure. Multiple studies have shown that excessive vancomycin is removed in the cardiopulmonary bypass circuit. These studies showed that there was an 11–16% decrease in vancomycin concentration once the antibiotic was injected into the bypass circuit [15–17]. There is concern that because some antibiotics, such as vancomycin, are removed in the cardiopulmonary bypass circuit, cefazolin could also be removed. In this study, injection of cefazolin directly into the bypass circuit achieved adequate cefazolin concentrations during bypass.
With the new IDSA/ASHP guidelines recommending three grams of cefazolin be administered if the patient is greater than 120 kg, only one patient in our study would have been dosed at three grams [9]. This patient remained well above the MIC throughout the entire procedure when only receiving two grams at incision indicating that with this dosing strategy it might not be necessary to give an initial two grams at incision.
The dosing strategy at UMMC gave a cumulative cefazolin dose higher than previously documented intraoperative doses. The associated cefazolin serum concentrations were higher than observed in previous literature [8,10,18]. Although some patients had total concentrations greater than 300 mcg/mL, no adverse reactions were witnessed as a result of these high concentrations.
The generalizability of the study may be limited by the patient population consisting of only those patients undergoing elective cardiopulmonary bypass graft surgery. However, the pharmacokinetics of cefazolin for surgical prophylaxis should be the same for any cardiac surgery utilizing cardiopulmonary bypass. Although the study had a small sample size, there was a large variety of patient weight, bypass times and surgical times represented and similar pharmacokinetic studies such as this have similarly evaluated eight to 12 patients [8,10,18].
Administering cefazolin into the bypass circuit and utilizing a two gram dose for redosing throughout the surgical procedure achieves targeted serum concentrations. Future, larger prospective studies that take into account protein binding and tissue levels should assess if the aggressive dosing of cefazolin recommended by the current guidelines is necessary.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.