
Abstract
Abstract
Background:
Severe acute pancreatitis (AP) often leads to distant organ dysfunction with a high morbidity and mortality rate. The most common and earliest organ to fail is the lungs, but the exact pathophysiological mechanisms underlying the disease are still unclear. No successful targeted therapy exists, and treatment is limited to organ supportive care. It is believed that the gut is involved in the development of distant organ failure, as severe AP is associated with changes in the microcirculation, gut permeability/motility, bacterial translocation, and activation of the gut-associated lymphoid tissue (GALT). Experimental evidence implicates the mesenteric lymph as a primary route for these toxic factors to gain access to the systemic circulation. This literature overview was made to survey these mechanisms and the potential of surgical interventions on the thoracic duct as a means of therapy.
Methods:
Review of the pertinent English-language literature.
Results:
In experimental studies, interruption of mesenteric lymphatic flow has preventive qualities for acute lung injury (ALI) in the setting of critical illness with various etiologies. Experimentally, diversion of mesenteric lymph is able to prevent ALI if done before its development, whereas a later intervention partially reduces the lung damage. Few studies have investigated surgical approaches to the thoracic duct in human beings under these circumstances, and the ones that have been performed are of low quality and have conflicting results. It seems likely that the intervention would need to be performed prior to the development of ALI to obtain maximum benefits, which complicates its application clinically, because prediction of ALI cannot today be done with high precision.
Conclusion:
Studies are ongoing to identify the factors carried in mesenteric lymph that may cause end-organ failure (e.g., ALI) and, once recognized, might allow the development of novel targeted agents that would modify the disease course.
A
Deaths in AP occur in two phases, with early deaths caused by SIRS/multiple organ dysfunction syndrome (MODS) in the absence of bacterial infection and late deaths caused by the combination of MODS and sepsis [7]. The exact pathophysiological mechanisms that contribute to the systematic inflammatory response in AP are still largely unknown. This reduces the possibilities of treatment to merely organ supportive [8], leading to high morbidity and mortality rates, long hospital stays [9], and a substantial economic burden [10]. There is a demand for a more targeted intervention that could limit the risk of disease progression. Addressing the mesenteric lymph is tempting, because growing evidence points to the importance of the gut and the lymphatic system in critical illness [11–14]. This literature overview was performed to survey underlying mechanisms for AP, including the association between gut barrier failure, systemic inflammatory response, and the development of remote organ failure, with a focus on acute lung injury (ALI). Furthermore, we investigated the possibilities of surgical intervention directed toward the mesenteric lymph as a means of treatment or prevention of ALI in severe AP.
Acute Pancreatitis: From Local Event to Remote Organ Injury
It is believed that pancreatic inflammation is initiated by the inappropriate activation of trypsinogen into trypsin inside the acinar cells of the pancreas. This causes autodigestion of the cells, and the inflammatory process in the pancreas is initiated [15]. The endothelial cells of the pancreatic microcirculation express adhesion molecules that enable leukocytes to infiltrate the pancreas, which increases the damage to the pancreas further [16]. Additionally, epithelial barrier dysfunction causes edema and third-space fluid loss, resulting in hypovolemia [17]. In the mild type of the disease, the effect is limited to a localized edema of the pancreas, which is easily manageable, whereas the severe form can extend into critical fluid loss requiring intensive care. The inflammatory reaction may thus progress into SIRS that, if substantial, can lead to MODS and give rise to necrosis in the pancreatic–peripancreatic tissue.
The magnitude of the acute inflammatory response and release of cytokines and other pro-inflammatory mediators correlates with the development of systemic complications and the development of single or multiple organ dysfunction [18–21]. Persistent SIRS is associated with MODS and death in AP and is an early indicator of the severity of the disease [22]. Furthermore, there is evidence that SIRS correlates with ischemia and reperfusion injury and that low blood pressure (i.e., hypovolemia; systolic blood pressure <100 mm Hg) at admission correlates with a higher mortality rate in patients with severe AP [23].
Acute Lung Injury: The Most Common Organ Dysfunction
A subset of patients with AP (about 20%) die before admission to the hospital, mainly as a consequence of ALI as a single organ dysfunction [24]. Deaths from AP during the hospital stay occur in about 40% of patients within the first week as a result of single (mainly ALI) or multiple organ dysfunction, often in the absence of overt bacterial infection. Later deaths generally are attributable to the combination of MODS and infection/sepsis. The most common organ to fail and the earliest one is the lung. Respiratory failure develops in some 45% of patients with severe AP, evident clinically as ALI. The mortality rate in general correlates with the number of failing organs [7].
Acute lung injury presents clinically with an acute onset and is defined by the presence of radiologic findings of bilateral pulmonary infiltrates, normal cardiac filling pressure, and a ratio of arterial oxygen pressure and fraction of inspired oxygen (PaO2/FiO2) of ≤300 mm Hg. Acute respiratory distress syndrome (ARDS) has the same criteria, except for a PaO2/FiO2 ratio of ≤200 mm Hg [25], meaning that all patients with ARDS also meet the criteria for ALI, therefore representing a severe form of ALI.
Acute lung injury occurs frequently in critically ill patients, but the exact underlying pathophysiological mechanism has in many instances yet to be defined [11]. For this reason, there is at present no effective treatment directed at these mechanisms in patients with established ALI, leaving organ supportive care as the only treatment option [8]. It has been estimated that ALI gives rise to 190,000 cases and 74,000 deaths in the U.S. annually and accounts for 3.6 million hospital days [9]. Thus, ALI represents a substantial cost for public health care.
Gut Barrier Failure in Acute Pancreatitis
Gut barrier failure was described long ago as being involved in critical illness, playing an active role in the development of both SIRS and MODS [26]. However, gut barrier failure is not merely a change in intestinal permeability leading to translocation of bacteria, but also involves the activation of immunocompetent cells within the gut wall and adjacent lymph nodes—gut-associated lymphoid tissue (GALT) [27,28]. The mechanisms believed to responsible for the development of gut barrier failure in AP are summarized in Figure 1.
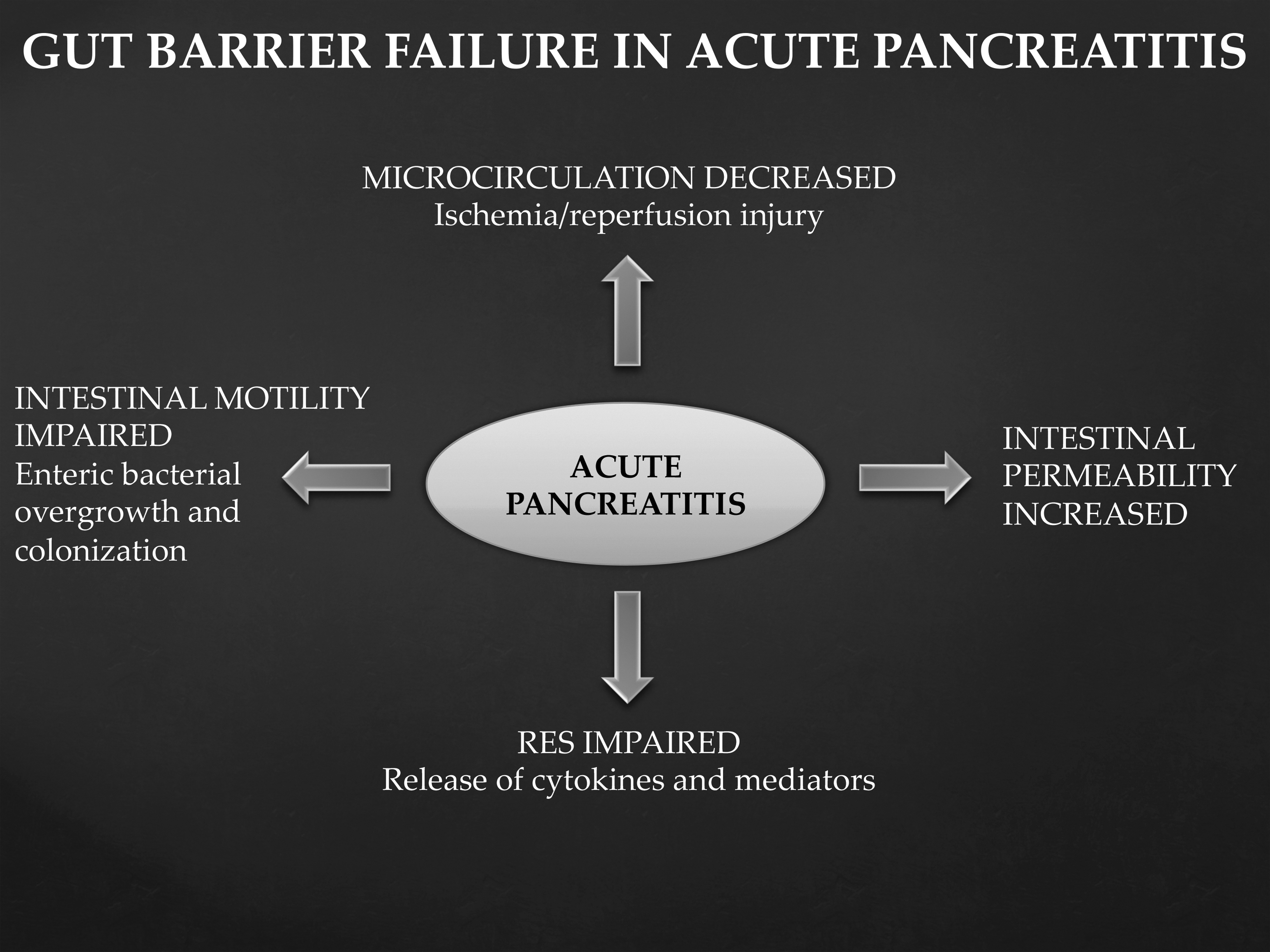
Mechanisms involved in gut barrier failure in acute pancreatitis. Abbreviation: RES=reticuloendothelial system. Adapted from references 27 and 28.
Acute pancreatitis is characterized by disturbances in the microcirculation. Potential mechanisms include increased vascular permeability, vasoconstriction, shunting, inadequate perfusion, and increased coagulation [29]. Impaired systemic and intestinal microcirculation leads to ischemia and reperfusion injury and the release of free oxygen radicals, which contribute to the development of gut barrier failure [27–29].
Translocation of bacteria attributable to increased permeability of the intestinal wall is thought to stimulate GALT and promote inflammation through the interaction between polymorphonuclear leukocytes and the endothelium, which may lead to a more intense SIRS reaction and MODS. The GALT may be overactivated, although reticuloendothelial system function seems to be impaired, resulting in local excessive release of cytokines and other mediators, which promote a gut inflammatory state [14,30,31]. In AP, intestinal motility also is impaired, leading to enteric bacterial overgrowth, morphologic changes, and tissue colonization [32].
Acute pancreatitis has been studied extensively in experimental models, and the grade of intestinal permeability was found to correlate with severity of disease in a rodent model [33]. Similar findings have been shown in human beings [34–36]. Traditionally, management of patients with AP has been to let the pancreas “rest” by applying parenteral fluids/nutrition and “nil per mouth” in all types of AP awaiting clinical improvement and normalization of C-reactive protein and amylase concentrations. In experimental AP, enteral nutrition improves gut barrier function by preserving the intestinal mucosa, permeability, and microbial flora, preventing bacterial translocation and sustaining the immunologic host response [37]. This implies that enteral nutrition may have a disease-limiting role. Meta-analyses of randomized clinical trials have found that enteral nutrition is associated with significant reductions in the mortality rate, multiple organ failure, systemic infections, and surgical interventions compared with parenteral nutrition [38,39].
Role of Mesenteric Lymph in the Development of Acute Lung Injury
The role of the gut lymph in the development of ALI has long been debated. Evidence from experimental studies points to mesenteric lymph not only participating, but also playing a key role, in the pathogenesis of lung complications in critical illness, as exemplified by severe AP. It is conceivable that the mechanisms underlying MODS are similar, although the etiologies may differ, and that a common denominator is gut barrier dysfunction and release of substances from both the intestinal lumen and, to some extent, GALT. Deitch et al. [40] theorize that this process begins with systemic hypotension, leading to splanchnic hypoperfusion. The resulting ischemia then impairs the barrier function of the gut, making it possible for bacteria/endotoxins and other harmful substances from the gut lumen to translocate over the gut barrier, in turn stimulating GALT to produce endogenous toxic factors. Rather than entering the portal circulation, these factors could instead exit through the mesenteric lymphatics and thereby bypass the filtering effect provided by the liver.
Molecular Analysis of Mesenteric Lymph
Molecular analysis of mesenteric lymph in the setting of AP has been conducted in only a few studies, and yet, from a biological standpoint, so much seems to hinge on an understanding of its composition in order to predict disease course and to modulate specific components.
A first step toward understanding the molecular composition of mesenteric lymph in AP was provided by the analysis of the proteome changes that accompany AP [41]. Mesenteric lymph was collected from rats with AP or from sham-treated control animals. The lymph was subjected to proteomic analysis using isobaric tags for relative and absolute quantification (iTRAQ) and liquid chromatography–tandem mass spectrometry. Two hundred forty-five proteins were identified in mesenteric lymph. Eight of them were significantly increased in the mesenteric lymph of the AP group, and all of these were pancreatic catabolic enzymes, namely pancreatic amylase 2, pancreatic lipase, carboxypeptidase A2, chymotrypsinogen B, carboxypeptidase B1, cationic trypsinogen, glutathione S-transferase, and ribonuclease 1.
The factors carried in the mesenteric lymph that contribute to dysfunction of remote organs; e.g., the lungs, have been investigated in experimental AP and then verified in human beings [42]. In the initial study, proteomic analysis of rats with AP-associated MODS was performed using surface-enhanced laser desorption/ionization time-of-flight (SELDI-TOF) mass spectrometry and two-dimensional gel electrophoresis. The results showed an increase of the kynurenine catabolites of tryptophan in the AP group compared with sham-treated animals. Plasma kynurenine concentrations were increased in human patients with AP and correlated directly with the occurrence of organ dysfunction and predicted the need for mechanical ventilation and hemodialysis.
The miRNAs are small non-protein-coding molecules that regulate gene expression. It has been hypothesized that miRNAs are present in mesenteric lymph and that changes in their amounts occur during AP [43]. Using Affymetrix miRNA profiling, 85 miRNAs have been detected in rat mesenteric lymph, of which seven (miR-375, -217, -148a, -216a, -122, -214, and -138) were increased in mesenteric lymph from rats with AP compared with sham-treated control animals. Several of the miRNAs identified in the experimental study were also found to be altered in the plasma of patients with AP, with one specific miRNA, miR-216a, showing a correlation with disease severity.
Surgical Diversion of Mesenteric Lymph: A Treatment Option?
The idea that surgical diversion of mesenteric lymph would have desirable effects is based on the view that diversion of mesenteric lymph in mice subjected to trauma/hemorrhagic shock (T/HS) prevented the increase in lung permeability and alveolar apoptosis observed in T/HS-mice that did not receive any intervention against the mesenteric lymph [44]. Furthermore, the degree of neutrophil sequestration in the lungs decreased, as measured by the activity of neutrophil-specific myeloperoxidase in the lung tissue. It thus was hypothesized that MODS in critical illness was not attributable primarily to the translocation of bacteria/endotoxins but rather to endogenous toxic factors produced by GALT in response to intestinal ischemia and disseminated into the mesenteric lymph. The beneficial effects of interruption of mesenteric lymph flow on the development of lung injury in critical illness of different etiologies have now been demonstrated in several animal models [45–50].
The effect of thoracic duct ligation was compared with thoracic duct drainage in an experimental model of acute hemorrhagic necrotizing pancreatitis [50]. There is a theoretical difference between the two approaches. Thoracic duct ligation may block the transport of harmful factors into the lungs so that lung injury may be reduced, but the intestine and pancreas may be damaged by the sequestration of factors in the abdomen. On the other hand, thoracic duct drainage results in the drainage of lymph from the organism, which theoretically leads to reduced damage to the lung, intestine, and pancreas simultaneously. In this particular study, both thoracic duct ligation and drainage decreased lung injury, but ligation of the thoracic duct aggravated intestinal and pancreatic injury, whereas thoracic duct drainage attenuated the injury to the lung, intestine, and pancreas at the same time. Similar findings were reported in a rodent model of intestinal ischemia/reperfusion injury, where drainage of mesenteric lymph reduced both lung and intestinal injury significantly [46].
In human beings, only a few clinical studies have been performed to test surgical interventions on the thoracic duct as a means to prevent ALI. In a non-randomized prospective study [51], 12 patients with severe AP complicated by ALI had their thoracic duct cannulated for collection of lymph. The patients improved their pulmonary gas exchange rapidly, and all patients survived the early phase of the disease without any specific adverse reactions. However, 11 of the patients suffered from late pancreatic complications (>10 d from onset), although only one patient died.
In another non-randomized, prospective study, conflicting results were found [52]. The study included six patients with severe AP who developed ARDS and were treated with drainage of the thoracic duct within 24 h after the onset of ARDS. Three of these patients died within the first week following drainage and another one after 19 d.
The timing of thoracic duct drainage seems important to achieving the best outcome. When the mesenteric lymph is diverted before inducing hemorrhagic shock in rats, lung injury can be prevented, whereas intervening after the shock only reduces the injury [44]. The studies performed in human beings have enrolled only those with severe AP in whom ALI is already established. Because both clinical studies mentioned above were non-randomized, without control groups, and containing small study populations, it is impossible to draw any conclusions concerning potential benefits of thoracic duct intervention. Possibly, the procedure should be applied even before ALI has developed, but predicting which AP patients will develop ALI is not possible with high precision. With the ambition to prevent ALI, this would therefore imply that patients at risk of developing ALI might be subjected to an invasive intervention, which is not without risks.
More literature on the surgical access to the thoracic duct exists in the field of chylothorax, where a minimally invasive percutaneous approach has been developed [53]. After examining the thoracic duct by pedal lymphangiography, the duct is catheterized transabdominally after applying local anesthesia and moderate sedation. The procedure is reported to have a low risk of complications [54]. The appropriateness of the transfer of this technique to use in critical illness is debatable, but for a surgical technique to be applied under these circumstances, its invasiveness needs to be minimized.
Conclusion
Acute pancreatitis is still a disease with substantial morbidity and mortality rates. Underlying pathophysiological mechanisms are to a large extent known, and we still lack details on many of the involved pro-inflammatory mediators and cells. It is evident that disease progresses from a local inflammatory condition to a systemic inflammatory response, where its magnitude to a large extent correlates with development of single or multiple organ dysfunctions and outcome. The role of the gut has been discussed, through impairment of microcirculation, gut barrier function, as well as pro-inflammatory substances and mediators from GALT. These factors augment the systemic inflammatory response and organ dysfunction where ALI is the first and dominating failing organ, related to fatal outcome and consuming enormous resources. The repeatedly shown association between mesenteric lymph and ALI in the experimental setting argues in favor of the idea that factors present in mesenteric lymph fuel the lung injury. Thoracic duct drainage has proved to attenuate ALI experimentally and even to prevent ALI if performed prior to critical illness. However, clinical experience is essentially absent, and the exact factors in mesenteric lymph responsible for ALI are not defined. Further studies are being performed by groups with a specific interest in the subject in order to define the factors in the mesenteric lymph that are responsible for ALI in AP, ideally providing novel tools for prevention and treatment.
Author Disclosure Statement
No competing financial interests exist.