
Abstract
Abstract
Background:
Our institution had an outbreak of multi-drug-resistant Acinetobacter (MDRA) in 2011. We analyzed the costs of responding to this outbreak from the hospital's perspective.
Methods:
We estimated retrospectively the excess costs associated with an MDRA outbreak response at a major academic medical center, including the costs of staffing, supplies, administrative time, deep cleaning, and environmental testing. Differences in mean costs before and during the 2011 MDRA outbreak were analyzed using the Student t-test.
Results:
The overall excess cost incurred during the outbreak response was $371,079 in 2011 U.S. dollars. The largest contributors were the extra resources needed to staff and clean the two intensive care units (ICUs) (78%). In the general surgery ICU, the mean weekly cost of nursing during the outbreak was $13,276 more for regular hours (+15%; p < 0.01) than in the pre-outbreak period and $2,682 more for overtime hours (+86%; p = 0.02). In the trauma ICU, the cost was $20,746 more for regular hours (+24%; p < 0.01) and $3,445 more for overtime hours (+124%; p < 0.01). The costs of supplies ($13,036; +30%; p = 0.03) and gloves ($2,572; +48%; p = 0.01) also were greater during the outbreak. Administrative time, consumables, use of a surge pod, and environmental testing accounted for the remainder of the extra costs.
Conclusions:
Our institution incurred $371,079 in excess costs as a result of an MDRA outbreak. This figure does not include the costs related to treatment of the infections, loss of reimbursement because of hospital-acquired infection, legal services, or changes in staff morale, patient satisfaction, or hospital reputation. Strategies to prevent and control such outbreaks better have substantial value.
H
Acinetobacter baumannii, a gram-negative bacterium, is associated with approximately 2%–10% of all gram-negative bacterial infections in U.S. intensive care units (ICUs) and has a crude mortality rate as high as 52% [11,12]. It can increase the mortality rate by 22% in ICU patients and add $30,000 in additional patient charges for greater hospital length of stay [13,14].
In 2004, and again seven years later, in 2011, our institution had outbreaks of multi-drug-resistant Acinetobacter (MDRA) infections in the trauma and general surgical ICUs. Both outbreaks triggered aggressive, multi-disciplinary infection-control responses. These included collective efforts by physicians, nurses, directors of various departments, as well as other hospital leadership to enhance hand hygiene, cohort infected patients, increase the nurse-to-patient ratio to 1:1, renew all disposable supplies, and shut down surgical units for deep cleaning of the environment and all permanent equipment.
There are limited data about the financial impacts of outbreaks and outbreak responses on major academic medical centers in the United States. In this paper, we calculated these excess costs of responding to the 2011 MDRA outbreak at our institution from the hospital's perspective.
Patient and Methods
Setting and population
Our institution is a 793-bed acute-care hospital with a 10-bed general surgery ICU and a 10-bed trauma ICU, both run by a multi-disciplinary team of surgeons, anesthesiologists, pulmonary critical care physicians, and emergency critical care physicians. The patient populations are similar in the two ICUs: The general surgery ICU population on average is 50% male, has an average age of 63 years, and length of stay of 3.7 days; and the trauma ICU population is 60% male with an average age of 57 years and length of stay of 3.6 days. Severity of illness, as measured by case mix index, is similar in the two ICUs (unpublished data from hospital quality management metrics).
The outbreak and the response
Nine cases of MDRA occurred over the course of a nine-week period in 2011. When the first case of MDRA was identified in the trauma ICU in May, strict contact precautions were implemented to limit transmission to other patients. In the ensuing weeks, however, two more patients were found to have MDRA in their incisions and sputum samples. When the third case was noted in early June, the hospital assembled a multi-disciplinary team to lead a response to a potential outbreak. The team included the chief medical officer and chief nursing officer, the hospital epidemiologist, infection prevention staff, medical and nursing leadership, respiratory therapy, environmental services, information systems, public relations, frontline physicians and nurses, and materials management. The importance of hand hygiene, strict contact precautions, cleaning of shared equipment, and environmental cleaning were highlighted and reinforced with the staff through group sessions, e-mails, handouts, and one-on-one discussions.
Despite these measures, a fourth case of MDRA was identified shortly thereafter, prompting the hospital to consider environmental contamination as a source and leading to a shut–down of the general surgery ICU for deep cleaning. All four MDRA patients were transferred to a surge pod: A separate hospital ward designed to accommodate overflow patients, typically to off-load the Emergency Department. Patients were cohorted to minimize interactions between the staff caring for these patients and those taking care of other ICU patients. Nurses were assigned to MDRA patients on a 1:1 basis, an increase from the standard 1:2 nurse-to-patient ratio, in order to limit contact between MDRA and non-MDRA patients, thereby limiting transmission of the pathogen. Screening for MDRA in uninfected patients was initiated, with cultures taken from the axilla, groin, wound/incision, and sputum.
Nevertheless, additional cases were detected in the trauma ICU, which is on the same floor of the hospital but in a different wing. The hospital then decided to close both ICUs to new admissions, conduct environmental sampling, and limit the number of physicians examining each ICU patient. The trauma ICU was shut down and deep cleaned, and all patients were temporarily transferred to a surge pod. By mid-July, no further cases of MDRA were identified, and the outbreak was considered contained. The measures taken during the intervention are summarized in Table 1. The response to the outbreak occurred over a six-week period from June–July 2011.
Deep cleaning was done by the housekeeping staff once per ICU during the intervention when all the patients were moved out of the ward with close supervision by the Director of Housekeeping, who led the black light testing.
Limiting the number of physicians to avoid transmission of pathogens, as physicians could carry the bacteria with them. Patients may have multiple teams of physicians such as ICU, surgery, infectious disease, cardiology, etc.; a maximum of two physicians per team were allowed to enter each ICU room to do examinations during the outbreak.
ICU = intensive care unit; MDRA = multi-drug-resistant Acinetobacter baumanniii.
Cost analysis
A cost analysis of the MDRA outbreak response was conducted in 2011 U.S. dollars and analyzed from the hospital's perspective. The cost of the outbreak response was calculated as excess costs during the outbreak response compared with pre-outbreak costs. We excluded the costs of treating patients with MDRA, as we aimed solely to quantify the costs associated with containment of the outbreak. We obtained Institutional Review Board approval and then contacted hospital finance managers and directors of patient service departments, including the directors of nursing, respiratory, environmental, and transport services. We obtained the costs of staffing and supplies from hospital accounting records, which included cost data for eight months (33 weeks) leading up to the outbreak and the six weeks during the outbreak response.
Cost data for regular and overtime nursing hours are recorded at week's end in the hospital's accounting records. These data were analyzed between October 2010 and May 2011 (before the outbreak) and from June to July 2011 (during the outbreak response). We observed variations in the weekly labor costs and calculated both mean and median costs. We tested for differences in mean costs between the pre-outbreak and the outbreak response periods. The excess cost was calculated as actual weekly cost from the outbreak response period less the mean weekly cost in the pre-outbreak period. This was summed across the six weeks of the outbreak response to generate estimates of total excess cost attributable to the additional nursing staff required in each unit.
The unit directors in the general surgery and trauma ICUs collect cost data in three categories on a monthly basis: General supplies, gloves, and laundry. Data from October 2010 to July 2011 records were pulled for this study. Supply costs were captured in an offset manner in the standard accounting practices such that the values referred to supplies purchased in the previous month. Furthermore, because the cost data were captured routinely on a monthly basis, there was no accurate method of calculating supply costs for the six-week outbreak response time. Therefore, we elected to use two full months of costs for consumables during the outbreak response period in order to generate the best possible estimate of excess consumables cost. We compared the mean monthly costs in the pre-outbreak period with the actual monthly costs during the outbreak to determine the excess costs that could be attributed to supplies, gloves, and laundry.
Patients with MDRA were moved to a surge pod for two 48-h periods when each of the ICUs was being cleaned. This surge pod had to undergo deep cleaning after patients were moved back to the ICUs. Thus, the cleaning costs for each of the ICUs and the surge pod were captured as excess costs attributable to the outbreak response. This included the costs of cleaning supplies and housekeeping staff. The additional nursing staff required for the move also was taken into consideration.
When cost data could not be deciphered from the accounting records, the directors of each patient service department gave estimates of the additional costs associated with the outbreak response, including respiratory therapy supplies and environmental laboratory tests such as swabs and cultures. We did not take into account the cost of unoccupied ICU beds when the ICUs were closed, because we could not determine retrospectively how many beds were not available during this time.
Administrative costs for the overall 2011 outbreak response period were estimated by multiplying the time spent (in hours) responding to the outbreak by the fully loaded (i.e., salary and fringe benefits) compensation rates for individual personnel. Interviews were conducted with clinicians and hospital administrators to gather estimates of time (in hours) spent in organizing and conducting the MDRA outbreak response. Combining these time estimates with confidential salary and benefits of involved personnel, the Hospital's Budget Office calculated the aggregated administrative labor cost.
Post-outbreak costs were not used for analysis, as they may have been affected by the outbreak. For instance, the nursing costs might be high for weeks to months after the outbreak, possibly as a result of the consequences of caring for patients with MDRA, who, according to the literature, have longer and more complicated hospital stays [15].
Statistical analysis
The cost items before and during the 2011 MDRA outbreak were entered and analyzed using Microsoft Excel (Microsoft, Seattle, WA) and Stata/SE 12.0 for Windows software (StataCorp LP, College Station, TX). Tests for mean difference were performed using a two-tailed Student t-test with an alpha of 0.05. All p values < 0.05 were considered statistically significant.
Results
Cost analysis
The overall excess cost incurred by the hospital during the 2011 MDRA outbreak response was estimated to be $371,079 (Table 2). The largest contributors to the cost were the extra resources needed to staff and clean the two ICUs, which accounted for more than 78% of the total outbreak response cost (Fig. 1).
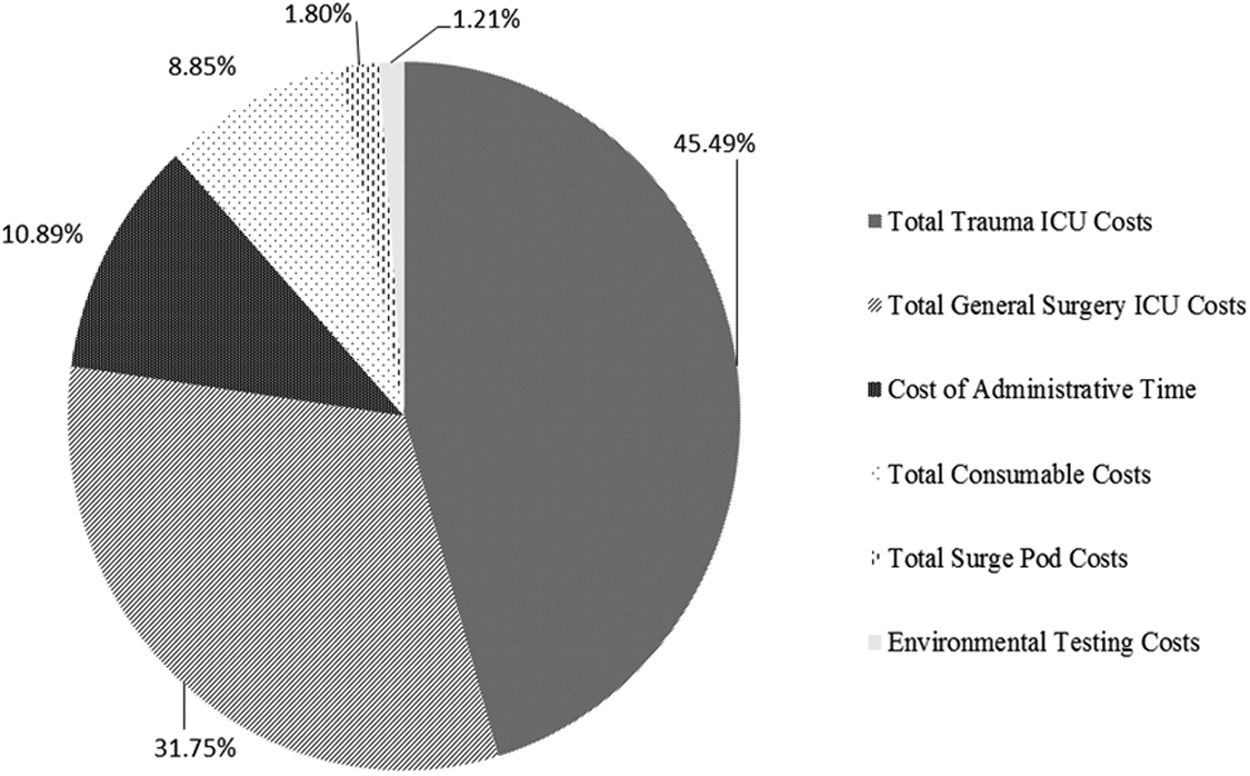
Distribution of response costs during 2011 multi-drug-resistant Acinetobacter baumannii outbreak.
All costs are expressed in 2011 U.S. dollars.
GS = general surgery; ICU = intensive care unit; MDRA = multi-drug resistant Acinetobacter baumannii.
The mean and median weekly costs of nursing staff were significantly greater during the outbreak response in both the general surgery and the trauma ICU (Table 3). In the general surgery ICU, the mean excess weekly costs attributable to regular nursing hours during the outbreak period were $13,276 (15%) more than in the pre-outbreak period (p < 0.01), and the excess attributable to overtime hours was $2,682 (86%) more than in the pre-outbreak period (p = 0.02). In the trauma surgery ICU, the mean excess weekly cost of nursing regular hours during the outbreak was $20,746 (24%) more than before the outbreak (p < 0.01), and the excess caused by overtime costs was $3,445 (124%) more (p < 0.01).
Calculated from two-tailed Student t-test with alpha of 0.05. All costs are expressed in 2011 U.S. dollars.
CI = confidence interval; ICU = intensive care unit; max = maximum; MDRA = multi-drug-resistant Acinetobacter baumannii; min = minimum.
The excess costs for consumables during the outbreak period are noted in Table 4. The mean general supply cost was $13,036 (30%) greater per month than the pre-outbreak value (p = 0.03), and the cost of gloves was $2,572 (48%) greater per month than the pre-outbreak value (p = 0.01). There was no statistically significant change in the mean monthly laundry cost (p = 0.92).
Calculated from two-tailed Student t-test with alpha of 0.05. All costs are in 2011 U.S. dollars.
CI = confidence interval; ICU = intensive care unit; max = maximum; MDRA = multi-drug-resistant Acinetobacter baumannii; min = minimum.
Deep cleaning of the surge pod cost a total of $14,448 in labor. Environmental testing of the affected ICUs resulted in an additional cost of $4,500 (see Table 2). The excess administrative time and effort required to address the outbreak were calculated on the basis of an estimated 393 hours spent by hospital leadership, surgical and anesthesia directors, patient care department leaders, and infection control staff on outbreak response-related activities (Table 5). The hospital's budget office estimated the value of this time to be approximately $40,395 based on salary and benefit calculations.
Not including preparatory time for meetings; e.g., time spent reading or writing reports regarding the outbreak or disseminating plans from the meetings.
ICU = intensive care unit.
Discussion
This study is the first to report the hospital-level costs of responding to a multi-drug-resistant Acinetobacter outbreak in the United States; patient-level costs have been reported previously [15]. Cost analyses of other resistant Acinetobacter outbreaks have been reported to be €539,325 and €202,214 ($671,600 and $251,809 in 2011 dollars) for two outbreaks at a hospital in Poitiers, France—one in 2006 and another in 2009—based on the cost of bed closures, screening, and hygiene measures [16, 17] Those investigators concluded that moving quickly to unit closure facilitated faster outbreak containment and limited overall outbreak costs. Another hospital, in Brest, France, reported €264,553 ($329,437 in 2011 dollars [16]) in outbreak response costs, including the costs of waste elimination and cleaning (€12,000 and $14,943 in 2011 [16]) and disposal of medications and supplies (€36,000 and $44,829 in 2011 [16]), as well as the loss of revenue from unoccupied ICU beds for the 10 days the unit was closed [18]. However, neither of these studies undertook a detailed quantification of costs, as in our study, and the obvious major differences in the health systems in the two settings limit the generalizability and comparability of outbreak management costs in France and the United States.
This project attempted solely to quantify the costs of the outbreak response. We intentionally excluded the costs of treating patients with MDRA. No doubt inclusion of these costs would have increased the total excess costs that could be attributed to an MDRA outbreak. The cost attributable to an hospital-acquired infection is estimated to be $25,694–$32,388 in 2011 U.S. dollars [16,19]. Other estimates have ranged from several thousand dollars to as much as $60,913 [13–15]. If included in this analysis, the cost of managing each additional case of MDRA infection during this outbreak therefore could contribute as much as $548,217 in excess costs beyond the outbreak response costs we calculated here (nine cases of MDRA at $60,913 per case). Thus, whereas we report the best possible cost estimates of containing an MDRA outbreak, the costs of the outbreak itself are likely to be much greater than $371,079 when treatment costs are included. Furthermore, we excluded other costs such as the financial impact of any operating room case cancellations, use of any additional recovery room resources, changes in staff morale and patient satisfaction, litigation, loss of reimbursement, and impact on the hospital's reputation in the community, which are financial implications of the outbreak itself and not of the outbreak response.
There are many limitations to our study. The quality and availability of cost data in the hospital were limited, and the data had to be obtained retrospectively from each of several patient care departments as well as the hospital's budget office. Currently, the institution's accounting system tracks expenditures as they relate to patient care and the cost of daily operations but not direct costs associated with anomalous events such as outbreaks. For instance, cost data for staffing the surge pods were not specific to the days on which ICU patients were moved to permit deep cleaning. Rather, it was reported to be $3,486 for the week of the move. That full week's cost was used for the outbreak response even though the surge pod was used for only a few days when the ICUs had to be deep-cleaned. The same situation applied to the cost of consumables, although again, this would at overestimate the total cost of the outbreak response by 3% at most. Furthermore, any seasonal variation in cost could not be assessed in this study.
Our estimation of the contribution of administrative costs to the overall outbreak response is another limitation. Because this component was based on the estimated number of hours spent by hospital and unit leaders in organizing the outbreak response, and was determined by asking the involved participants to estimate the time they spent on the response, it is prone to recall bias. However, the estimated number of administrative hours spent on responding to the outbreak probably is an underestimate, as it was based solely on scheduled meeting times. Staff could recall accurately the daily or weekly meetings that were scheduled during the outbreak response period, but we did not account for the time they spent preparing for meetings or disseminating plans after meetings, as this could not be quantified accurately in retrospect. Lastly, although molecular typing and clonality analysis are useful adjuncts to outbreak responses [20], we did not have access to such techniques for this study.
The key components of the outbreak response were shutting down and deep-cleaning the ICUs, cohorting infected patients, increasing the nurse-to-patient ratio to 1:1, and renewing all disposable supplies. As we have shown elsewhere, the value of improving hand hygiene compliance is essential but needs to be part of a larger infection control strategy that includes aggressive environmental cleaning [21,22]. Hand hygiene compliance was more than 90% in both units before and after this MDRA outbreak; therefore, hand hygiene alone may not be the panacea for outbreak control [22]. From our experience, we suspect that environmental decontamination played the major role in finally halting the outbreak. Patient decontamination with chlorhexidine baths, as reported by Climo et al., may be a potentially critical method to reduce reservoirs of infection [23]. Furthermore, it may be argued that key components of the outbreak response should be implemented sooner to limit the extent of Acinetobacter outbreaks, especially because of the organism's longevity on environmental surfaces [24]. Whether these interventions can be implemented as a part of a standard package to prevent outbreaks remains to be seen.
Our findings may not be generalizable to other hospitals or healthcare settings. Across U.S. hospitals, the costs of a similar outbreak response certainly would vary with patient volume, size of hospital units/wards, and staff salary costs. Nevertheless, the costs associated with this outbreak response reinforce the value of supporting rigorous routine infection prevention programs.
Conclusion
Aggressive, multi-faceted infection control interventions can be effective in containing MDRA outbreaks but do so at a substantial financial impact, not including the costs of treatment as well as other broader effects on the hospital and the community. Scheduled periodic infection control bundles may reduce the probability of outbreaks and may be of high value if they can be implemented at a reasonable cost.
Footnotes
Acknowledgments
We thank S.A., A.K., and the Partners Center for Clinical Excellence at Brigham and Women's Hospital for their support of this work. We are grateful to all of our patients for the opportunity to care for them, and to P.K., in particular, whose illness spurred us to ask these questions.
Author Disclosure Statement
No competing financial interests exist. The Partners Centers of Expertise Quality and Patient Safety Program and Partners Graduate Medical Education supported the conduct of this project.