
Abstract
Abstract
Background:
Despite frequent use of prophylactic antibiotics for patients undergoing transrectal prostate biopsy (TRPB), the incidences of urinary tract infection (UTI) and bacteria resistance are increasing. The aim of this study is to evaluate the current regimen of antimicrobial prophylaxis in TRPB.
Methods:
A systematic search of PubMed®, Embase®, and the Cochrane Library was performed to identify all randomized controlled trials (RCT) related to the effects of antibiotic prophylaxis for TRPB. The outcomes included bacteriuria, bacteremia, drug-resistant bacteria on urine/blood culture, fever, UTI, sepsis, and hospitalization.
Results:
A total of 22 RCTs with 3846 patients were identified and included. Nine trials analyzed antibiotics versus placebo/no treatment, with all outcomes substantially favoring antibiotic use (p<0.05), including bacteriuria (risk ratio [RR] 0.25, 95% confidence interval [CI] 0.15–0.42), bacteremia (RR 0.67, 95% CI 0.49–0.92), fever (RR 0.39, 95% CI 0.23–0.64), UTI (RR 0.37, 95% CI 0.22–0.62), and hospitalization (RR 0.13, 95% CI 0.03–0.55). There were no substantial differences between long-course versus short-course treatment and single versus multiple dose respectively, except for a greater risk of bacteriuria for short-course treatment (RR 2.09, 95% CI 1.17–3.73, p=0.01) and single-dose treatment (RR 1.98, 95% CI 1.18–3.33, p=0.01). There were no substantial differences among the groups for bacteriuria, fever, UTI, and hospitalization, when comparing oral versus systemic administration of antibiotics. The efficacy of several classes of antibiotics was compared without any difference among them. Despite the lack of significance, the synthesized data of three RCTs indicated a trend towards the use of combined antibiotics.
Conclusions:
Prophylactic antibiotics could be beneficial for the reduction of infective complications after TRPB. Single-dose or short-course oral administration with any type of antibiotic appears to be optimal. One additional type of antibiotic added to the basic antibiotic agent may contribute to the minimization of severe infection and drug resistance.
T
Both the European Association of Urology (EAU) and the American Urological Association (AUA) support the use of prophylactic antibiotics prior to performing core biopsy of the prostate, and suggest that a single dose or 1-d treatment is as effective as a 3-d regimen [4,5]. The choices of regimen are debatable, and the type, dose, route, and duration of antibiotics are not standardized. Although debatable, fluoroquinolones (FQs) remain the most common agents for antibiotic prophylaxis for prostate biopsy (PB), as advocated by AUA, EAU, and other international urology associations [4–6].
Despite the widespread prescription of antibiotic prophylaxis, serious post-TRPB infections, which may lead to hospitalization, are reported in up to 6% of patients, with rates estimated to be increasing worldwide [7,8]. Recently, an increase in antibiotic resistance has been reported, particularly for fluoroquinolones [9]. Correspondingly, most studies have shown an increase in infective complications after TRPB over time [7,10]. One study retrospectively analyzed data from 5798 patients undergoing TRPB and found that the incidence of sepsis post-TRPB increased from 0.52 per 100 patients between 2002 and 2009 to 2.15 per 100 patients between 2010 and 2011, with substantially more fluoroquinolone-resistant cases [7]. To ameliorate this emerging situation, a few researchers applied combinations of antibiotic agents to lower the incidence of UTIs [10]. However, the overall effects need to be evaluated.
To assess the use of current prophylactic antibiotics in patients undergoing TRPB, we conducted a systematic review and meta-analysis to clarify which type, dose, route, and duration of antibiotics are the most appropriate and effective.
Patients and Methods
Search strategy
We did a systematic review and meta-analysis in accordance with the PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyzes) guidelines, and used a predetermined protocol. We searched the PubMed database (from 1937 to May 2014), Embase (from 1937 to May 2014), the Cochrane Central Register of Controlled Trials, and the Cochrane Database of Systematic Reviews. The initial search process was designed to find all trials involving the terms “prostate biopsy,” “antibiotic,” “bacteremia,” “bacteriuria,” and “infection” (and multiple synonyms for each term). Furthermore, we hand-searched reference lists from relevant publications and conference proceedings from the AUA, EAU, and Société Internationale d'Urologie (SIU) between 2009 and 2014. Computer searches were supplemented with manual searches. Two authors (LY and LG) independently screened all citations and abstracts identified using this search strategy to identify potentially eligible studies. All relevant randomized controlled clinical trials (RCTs) were included, regardless of language.
Participants
The inclusion criteria were as follows: Male patients who required TRPB and received prophylactic antibiotics or placebo/no treatment. Patients with particular conditions before TRPB were excluded from analysis, such as history of hypersensitivity to antibiotics in study, presence of indwelling bladder catheters, presence of culture-proven UTI, substantial gastrointestinal disease or inability to tolerate oral medication, patients with prostheses (e.g., hip replacement, prosthetic cardiac valves), or congenital heart disease requiring prophylactic antibiotics. Patients with history of endoscopic manipulation of the urinary tract within 7 d prior to the study enrollment, or with antibiotic given during the preceding 10 d before TRPB were also excluded.
Interventions and comparisons
All patients underwent TRPB, and were then classified into the following groups: 1. a prophylactic antibiotic group or a placebo or no treatment group; 2. antibiotic class A versus class B; 3. single-dose versus multiple-dose treatment; 4. short-course (1 d) versus long-course treatment (over 3 d); 5. oral versus systemic administration (intravenous [IV] and intramuscular [IM]); 6. combined antibiotics versus single agent. Comparisons were made regarding the outcomes of prophylactic antibiotic in the prevention of infection after TRPB.
Outcome measures
Outcomes measured in this review were as follows: Bacteriuria, bacteremia, rate of fever, incidence of UTI, and hospitalization rate. Bacteriuria was defined as the presence of bacteria in the urine in the post-procedure period or proven in culture (presence of any uropathogen not present previously or colony forming units (CFU) >100,000/mL) in the absence of clinical signs of infection, diagnosed in a urine sample obtained by protocol urine collection. The definition of bacteremia was the presence of bacteria in blood culture, obtained by protocol blood collection, irrespective of clinical signs. Fever was defined as patient's temperature greater than 37.5°C. The definition of UTI was commonly described as bacteriuria during the post-procedure period associated with clinical signs of UTI (dysuria, frequency, urgency). Sepsis was defined as systemic inflammatory response syndrome (SIRS) caused by infection. Patients with UTI who were admitted to the hospital were considered hospitalized. Drug-resistant bacteria in this review meant ESBL- or fluoroquinolone-resistant bacteria identified by urine or blood culture.
Data extraction
Data were extracted independently by two authors (YJC and ZT) using a pre-designed data extraction form. Data extraction included data source, eligibility, methods, participant characteristics, interventions, and results. Both authors convened to synthesize their findings. The information was subsequently entered into RevMan 5.1.4. Any discrepancy among the extracted data was resolved by discussion, and if the disagreements persisted after the discussion, they were resolved in consultation with another author (WQ).
Quality assessment
The quality of included studies was assessed by two authors (LLR and HP) according to the Cochrane Collaboration Reviewers' Handbook and the QUOROM guidelines [11,12]. The quality items were a generation of randomization sequences, blinding method, allocation concealment, description of withdrawals and dropouts, and intent to treat analysis.
Statistical analysis
All meta-analyses were performed using RevMan 5.1.4. Dichotomous data were presented as relative risk (RR), with 95% confidence interval (CI). The meta-analysis was performed using the fixed effects method or the random effects method, depending on the absence or the presence of substantial heterogeneity. Statistical heterogeneity among trials was evaluated by the I2 test, with significance set at p<0.05. The fixed-effects method was used to combine the results when statistically significant heterogeneity was absent. When heterogeneity was confirmed, the random effects method was applied. Publication bias was evaluated using a funnel plot. Furthermore, sensitivity analysis was performed if low quality trials were included in the analysis.
Results
Description of studies
In this study, a total of 1026 studies were initially identified from the database and manual search. After removing 395 records of redundant publications, reviews, and meta-analysis and scanning titles and abstracts of another 530 unrelated records, 925 reports were excluded from study. After referring to full texts, 22 publications (RCTs), with 3846 enrolled patients, were identified and included in this review (Fig. 1) [13–37]. The characteristics and quality of the included studies are presented in Table 1 and Table 2. The search flow diagram is presented in Fig. 1. Twenty-two RCTs reported trial origination (Brazil=two, Canada=one, China=two, France=one, Greece=one, India=one, Italy=two, Spain=one, Turkey=three, United Kingdom=three, United States=five). Study discontinuations ranged from 0% to 25%, with an overall mean of 4.7%. Weighted mean follow-up was 13.5 d, and ranged from 4 d to 28 d.

Flow diagram of systematic review.
ND=not determined; UTI=urinary tract infection.
Antibiotics versus placebo/no treatment
Nine placebo controlled trials described the effects of antibiotics versus placebo/no treatment in preventing infectious complications following TRPB [13,14,19,23,25–28,31,34,36,37]. Five trials (1229 patients) compared fluoroquinolones to placebo [13,14,25,27,34,36,37]. Two trials (189 patients) compared sulfonamides to placebo [26,31]. Two trials (129 patients) compared penicillin to placebo (piperacillin [28]; carbenicillin [23]). One trial (40 patients) compared gentamicin to placebo [19]. Three trials were three-armed studies, [13,14,25,26,36,37], including one trial that compared data of two different antibiotics versus placebo [25,26], and two trials that compared short- and long-course antibiotic treatments versus placebo [13,14,36,37].
Bacteriuria
Data on bacteriuria could be extracted from seven trials with 870 patients [19,23–28,31,34]. There were 61 events of bacteriuria among 412 patients randomized to receive placebo and 18 among 458 patients randomized to receive antibiotics (Fig. 2A). The meta-analysis, including subgroup analysis, was substantial and favored antibiotic use (RR 0.25, 95% CI 0.15–0.42, p<0.00001; fluroquinolones RR 0.33, 95% CI 0.17–0.64, p=0.001; sulfonamide RR 0.17, 95% CI 0.05–0.57, p=0.004; other classes of antibiotics RR 0.20, 95% CI 0.07–0.54, p=0.001).

Antibiotics versus placebo/no treatment
Bacteremia
We collected data on bacteremia from five trials with 494 patients [13,14,19,23,28,31]. There were 45 cases of bacteremia among 237 patients randomized to receive placebo and 34 cases among 257 patients randomized to receive antibiotic (Fig. 2B). The comparison was substantial and favored antibiotic use; however, there were no substantial differences between fluoroquinolones versus placebo and sulfonamide versus placebo (RR 0.67, 95% CI 0.49–0.92, p=0.001; fluoroquinolones RR 0.32, 95% CI 0.05–2.01, p=0.22; sulfonamide RR 0.85, 95% CI 0.61–1.17, p=0.32; other classes of antibiotics RR 0.47, 95% CI 0.22–0.98, p=0.04).
Fever
Data on fever were extracted from seven trials with 820 patients [13,14,19,23,28,31,34,36,37]. There were 43 events of fever among 397 patients randomized to receive placebo and 17 among 423 patients randomized to receive antibiotic (Fig. 2C). The comparison was substantial and favored antibiotic use; however, there were no substantial differences between fluoroquinolones versus placebo and sulfonamide versus placebo (RR 0.39, 95% CI 0.23–0.64, p=0.0003; fluoroquinolones RR 0.48, 95% CI 0.22–1.06, p=0.07; sulfonamide RR, 0.69 95% CI 0.20–2.38, p=0.056; other classes of antibiotics RR 0.23, 95% CI 0.10–0.54, p=0.0007).
UTI
We collected data on UTI from three trials with 1077 patients [13,14,27,36,37]. There were 48 cases among 534 patients randomized to receive placebo, and 18 among 543 randomized to receive antibiotics (Fig. 2D). The meta-analysis result was substantial and favored the use of antibiotics (RR 0.37, 95% CI 0.22–0.62, p=0.00002).
Hospitalization
Data on hospitalization could be collected from two trials (one trial subdivided) with 650 patients [25–27]. There were 10 hospitalizations among the 306 patients randomized to receive placebo and only one among the 344 patients randomized to receive antibiotics (Fig. 2E). The comparison was substantial and favored antibiotics (RR 0.13, 95% CI 0.03–0.55, P=0.006).
Adverse effects
Adverse effects (nausea and abdominal cramps in Crawford's study [23], and pruritus and diarrhea in Ruebush's study [31]) were poorly reported among the included studies, and were extracted from only two studies with 127 patients (Fig. 2F). The comparison was not substantial (RR 1.62, 95% CI 0.23–11.56, p=0.63).
Sepsis
The sepsis was reported in only one study [23]. There were three cases of sepsis among 25 patients randomized to receive placebo and one case among 23 randomized to receive antibiotic use (RR 0.36, 95% CI 0.04–3.24, p=0.36).
Short-course (1 d) versus long-course (3 d) antibiotics
This intervention was reported in seven trials [13,18,20,30,32,35,36].
Bacteriuria
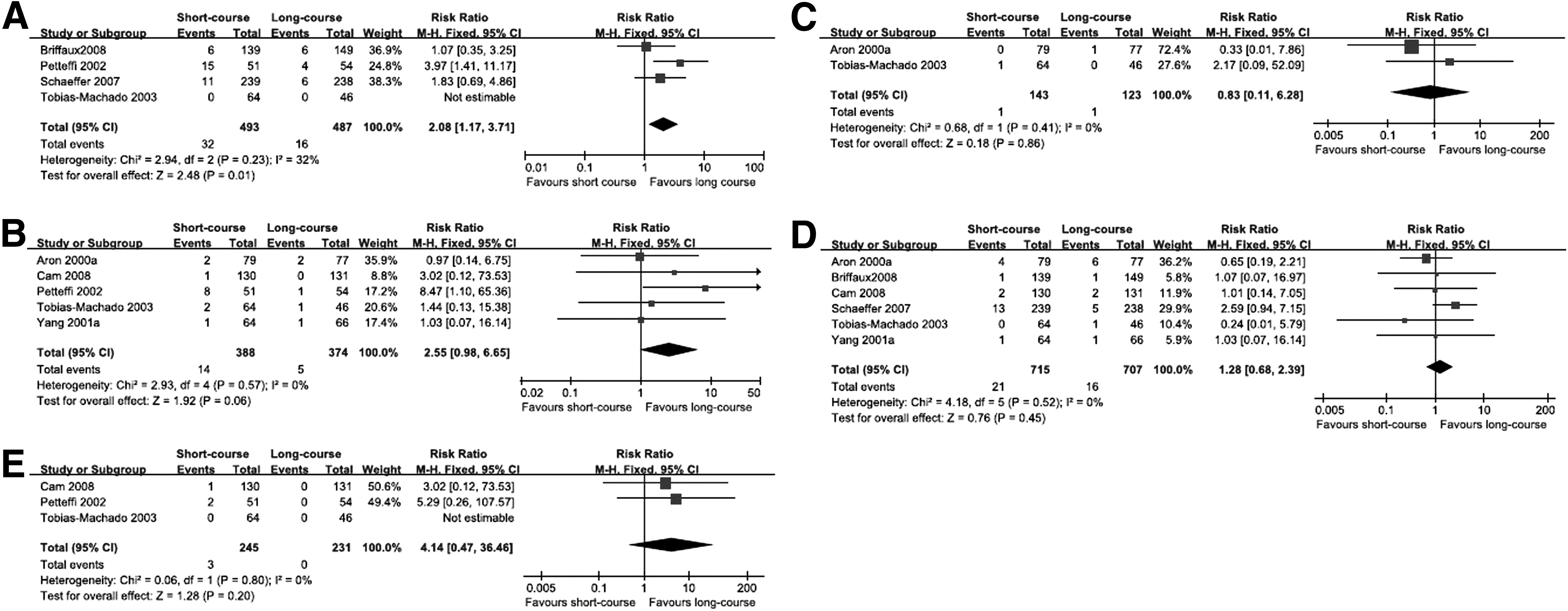
Four studies investigated bacteriuria [18,30,32,35]. There were 32 events of bacteriuria among 493 patients randomized to receive short-course treatment and 16 among 487 patients to receive long-course treatment (Fig. 3A). The rate of bacteriuria in long-course is substantially lower than the short-course (RR 2.08, 95% CI 1.17–3.71, p=0.01).
Short-course versus long-course antibiotics
Bacteremia
Bacteremia was reported in two included studies [13,35]. There was one case of bacteremia among 143 patients randomized to receive short-course treatment and one case among 123 patients to receive long-course treatment (Fig. 3B). There was no substantial difference between short-course and long-course in the rate of bacteremia (RR 0.83, 95% CI 0.11–6.28, p=0.86).
Fever
Data on fever were extracted from five trials with 820 patients [13,20,30,35,36]. There were 14 events of fever among 388 patients randomized to receive short-course treatment and five among 374 patients to receive long-course treatment (Fig. 3C). There was no substantial difference between short-course and long-course in the rate of fever (RR 2.55, 95% CI 0.98–6.65, p=0.06).
UTI
We collected data on UTI from six trials with 1422 patients [13,18,20,32,35,36]. There were 21 cases among 715 patients randomized to receive short-course antibiotic, and 16 among 707 to receive long-course antibiotic (Fig. 3D). There was no substantial difference between short-course and long-course in the incidence of UTI (RR 1.28, 95% CI 0.68–2.39, p=0.45).
Hospitalization
Data on hospitalization could be collected from three trials with 476 patients.[20,30,34] There were three hospitalizations among the 245 patients randomized to receive short-course treatment and zero among the 231 patients to long-course treatment (Fig. 3E). There was no substantial difference between short-course and long-course in the rate of hospitalization (RR 4.14, 95% CI 0.47–36.46, p=0.20).
Single dose versus multiple dose
This intervention was reported in eight trials [13,15,18,20,30,32,35,36].
Bacteriuria
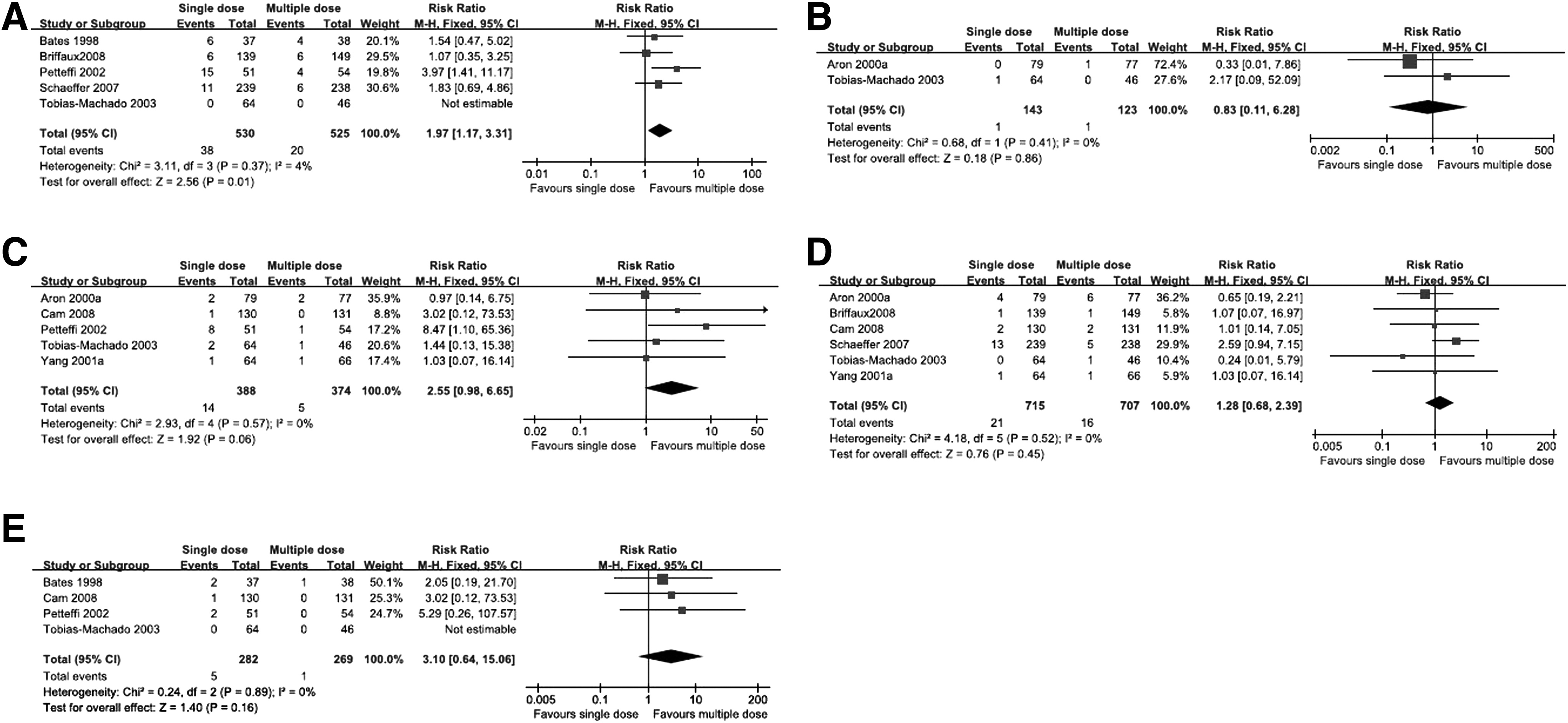
Bacteriuria was reported in five included studies [15,18,30,32,35]. There were 38 events of bacteriuria among 530 patients randomized to receive single-dose and 20 among 525 patients randomized to receive multiple-dose (Fig. 4A). The rate of bacteriuria in multiple-dose is substantially lower than the single-dose (RR 1.97, 95% CI 1.17–3.31, p=0.01).
Single dose versus multiple dose
Bacteremia
Only two studies investigated bacteremia [13,35]. There was one case of bacteremia among 143 patients randomized to receive single-dose and one case among 123 patients randomized to receive multiple-dose (Fig. 4B). There was no substantial difference between single-dose and multiple-dose in the rate of bacteremia (RR 0.83, 95% CI 0.11–6.28, p=0.86).
Fever
Data on fever were extracted from five trials with 820 patients [13,20,30,35,36]. There were 14 cases of fever among 388 patients randomized to receive single-dose and five among 374 patients randomized to receive multiple-dose (Fig. 4C). There was no substantial difference between single-dose and multiple-dose in the rate of fever (RR 2.55, 95% CI 0.98–6.65, p=0.06).
UTI
We collected data on UTI from six trials with 1422 patients [13,18,20,32,35,36]. There were 48 events among 715 patients randomized to receive single-dose antibiotic, and 18 among 707 patients randomized to receive multiple-dose antibiotic (Fig. 4D). There was no substantial difference between single-dose and multiple-dose in the incidence of UTI (RR 1.28, 95% CI 0.68–2.39, p=0.45).
Hospitalization
Data on hospitalization were collected from four trials with 571 patients [15,20,30,34]. There were five hospitalizations among the 282 patients randomized to receive single-dose and one among the 269 patients randomized to receive multiple-dose treatment (Fig. 4E). There was no substantial difference in the rate of hospitalization (RR 3.10, 95% CI 0.64–15.06, p=0.16) between short- and multiple-dose treatments.
Sepsis
Sepsis was reported in only one study [15]. There were two cases of sepsis among 37 patients in the single-dose group versus one case of sepsis among 38 patients in the multiple-dose group (p>0.05).
Oral versus systemic antibiotic administration
This intervention was reported in four trials [20,22,24,33]. There were 13 cases of bacteremia among 47 patients randomized to receive systemic antibiotics versus 20 cases of bacteremia among 54 randomized to receive oral antibiotics (p>0.05) [24]. There was one event of sepsis among 66 patients randomized to receive oral antibiotic versus zero events among 72 randomized to receive systemic antibiotic (p>0.05) [22].
Bacteriuria
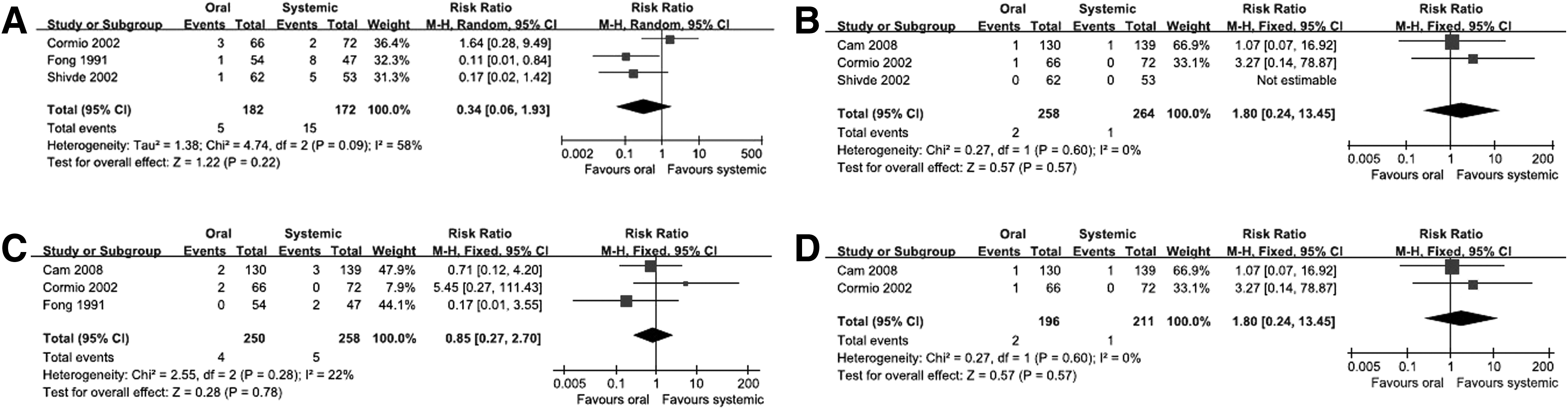
Three studies addressed to this issue [22,24,33]. There were five cases of bacteriuria among 182 patients randomized to receive oral administration and 15 among 172 patients randomized to receive systemic administration (Fig. 5A). The difference in the rate of bacteriuria between groups was not substantial (random effects model; RR 0.34, 95% CI 0.06–1.93, p=0.22).
Oral versus systemic antibiotic administration
Fever
Data on fever were collected from three trials with 522 patients [20,22,33]. There were two cases of bacteriuria among 258 patients randomized to receive oral administration and one among 264 randomized to receive systemic administration (Fig. 5B). The difference in the rate of fever between the groups was not substantial (RR 1.80, 95% CI 0.24–13.45, p=0.57).
UTI
We collected data on UTI from three trials with 508 patients [20,22,24]. There were four cases of UTI among 250 patients randomized to receive oral administration and five among 258 randomized to receive systemic administration (Fig. 5C). The difference in the incidence of UTI between the groups was not substantial (RR 0.85, 95% CI 0.27–2.70, p=0.78).
Hospitalization
Data on hospitalization were extracted from two trials with 407 patients [20,22]. There were two cases of hospitalization among 196 patients randomized to receive oral administration and one among 211 randomized to receive systemic route (Fig. 5D). The difference in the rate of hospitalization between the groups was not substantial (RR 1.80, 95% CI 0.24–13.45, p=0.57).
Antibiotic class A versus B
Included in this section were studies that compared different types of antibiotics, per class of antibiotic. We performed three subgroup analyses: Fluoroquinolone versus other antibiotics, sulfonamide versus other antibiotics, and piperacillin-tazobactam versus other antibiotics.
Fluoroquinolones versus other antibiotics
The outcomes analyzed were bacteriuria, bacteremia, fever, UTI, hospitalization, and sepsis. The comparisons between the groups (fluoroquinolone and other antibiotics) were not substantial for all outcomes.
1. Bacteremia
2. Bacteriuria
3. Fever
4. UTI
5. Hospitalization
6. Sepsis
The sepsis was reported in only one study [22]. There was one case among 66 randomized to receive fluoroquinolone and no case in group piperacillin-tazobactam (p>0.05)
Antibiotic class A versus B 1. Quinolones versus other antibiotics.
Sulfonamide versus other antibiotics
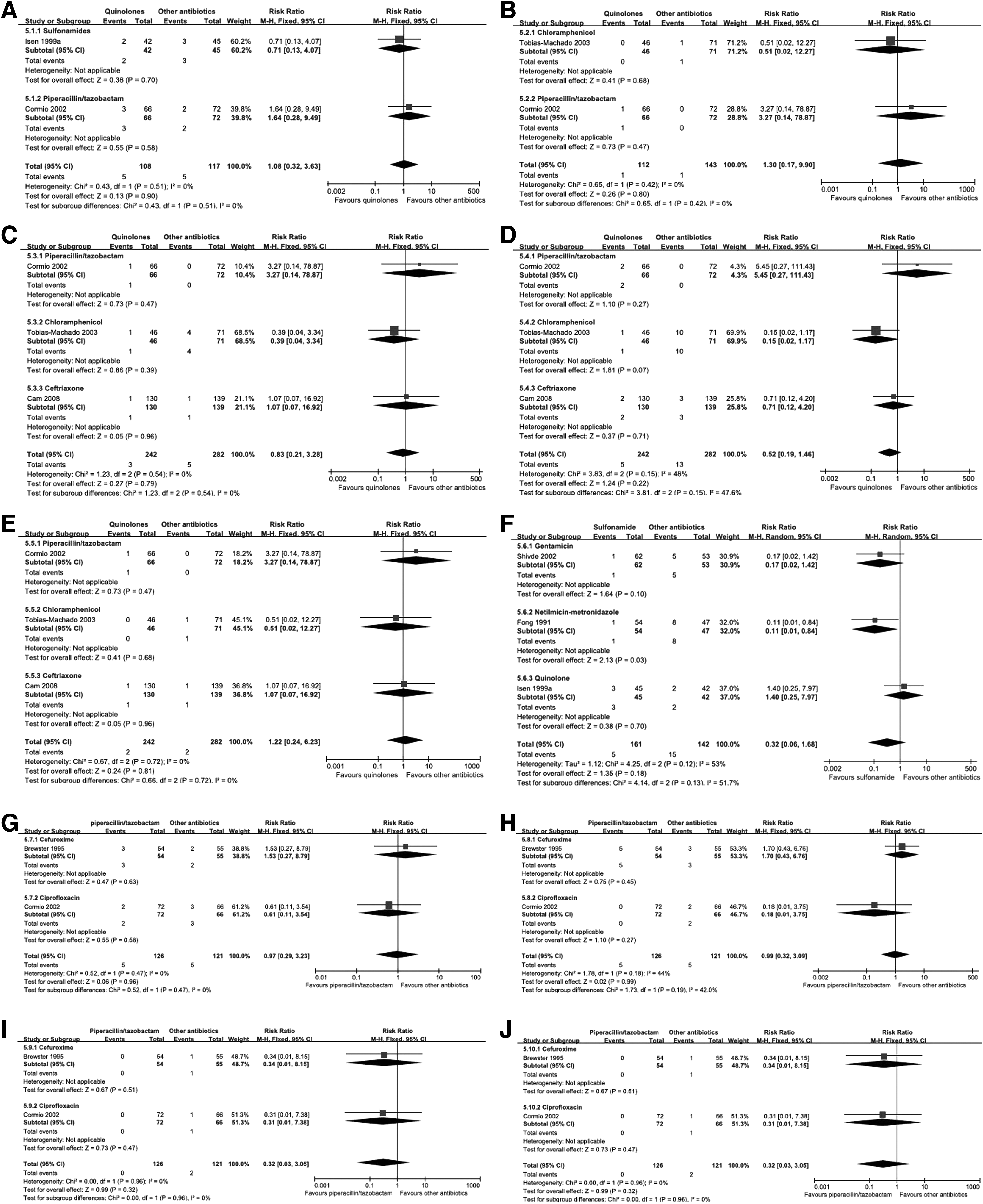
The outcomes analyzed were bacteriuria, bacteremia, and UTI. For bacteriuria, three trials with 303 patients were included [24,25,33], comparing sulfonamide to gentamicin, netilmicin–metronidazole, and fluoroquinolone. There were five cases among 161 patients using sulfonamide and 15 cases among 142 randomized to receive other antibiotics. The comparison between these groups was not substantial (random effects model; RR 0.32, 95% CI 0.06–1.68, P=0.18, Fig. 6F). Bacteremia and UTI were reported in only one study [25]. There were 13 cases of bacteremia and two cases of UTI among 47 patients randomized to receive the netilmicin-metronidazole and 20 cases of bacteremia and no case of UTI among 54 randomized to receive sulfonamide (P>0.05).
Piperacillin-tazobactam versus other antibiotics
The outcomes analyzed were bacteriuria, bacteremia, fever, UTI, sepsis, hospitalization, and adverse events.
For bacteriuria, UTI, sepsis, and hospitalization, two trials [17,22] were included with 247 patients. The comparisons between groups were not substantial for all outcomes.
1. Bacteriuria
The RR was 0.97, 95% CI 0.29–3.23, p=0.96 (Fig. 6G).
2. UTI
The RR was 0.99, 95% CI 0.32–3.09, p=0.99 (Fig. 6H).
3. Hospitalization
The RR was 0.32, 95% CI 0.03–3.05, p=0.32 (Fig. 6I).
4. Sepsis
The RR was 0.32, 95% CI 0.03–3.05, p=0.32 (Fig. 6J).
Only one trial reported bacteremia and adverse events [17]. There were no case of bacteremia and 16 adverse cases (diarrhea) among 54 patients randomized to piperacillin-tazobactam and one case of bacteremia (p>0.05) and two of adverse cases (diarrhea) among 55 randomized to receive cefuroxime (p<0.05). Fever was reported in one trial [22]. There was one case of fever among 66 patients randomized to receive fluoroquinolone and no case in 72 patients randomized to receive piperacillin-tazobactam (p>0.05).
Single drug versus combined drugs
Three trials involving 659 patients described the effects of single drug versus combined drugs in preventing infectious complications following TRPB [16,21,29]. One study compared tobramicin with tobramicin plus ciprofloxacin [16]. One trial compared amoxicillin-clavulanate with amoxicillin-clavulanate plus ciprofloxacin [21]. Ciprofloxacin was compared with ciprofloxacin plus ceftriaxone in another study [29].
Bacteriuria
Data on bacteriuria could be extracted from two trials with 502 patients [21,29]. There were four cases of bacteriuria among 249 patients randomized to receive single drug and zero cases among 253 patients randomized to receive combined drugs (Fig. 7A). There was no substantial difference between single and combined antibiotic use (RR 5.00, 95% CI 0.60–41.90, p=0.14).
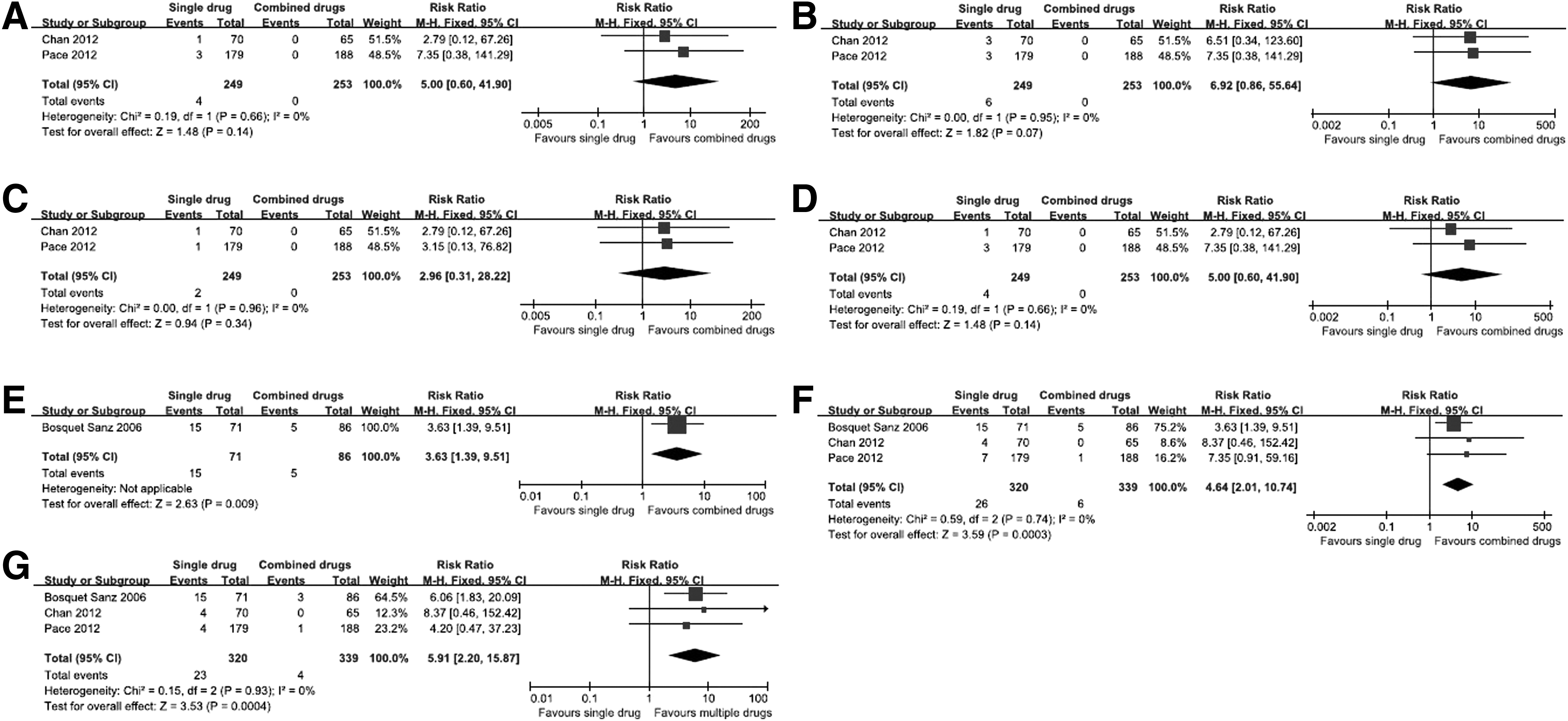
Single drug versus combined drugs
Bacteremia
We collected data on bacteremia from two trials with 502 patients [21,29]. There were six cases of bacteriuria among 249 patients randomized to receive single drug and zero cases among 253 patients randomized to receive combined drugs (Fig. 7B). There was no substantial difference between single and combined antibiotic use (RR 6.92, 95% CI 0.86–55.64, p=0.07).
Drug-resistant bacteria on urine culture
Data on drug-resistant bacteriuria could be extracted from two trials with 502 patients [21,29]. There were two cases among 249 patients randomized to receive single drug and zero cases among 253 patients randomized to receive combined drugs (Fig. 7C). There was no substantial difference between single and combined antibiotic use (RR 2.96, 95% CI 0.31–28.22, p=0.34).
Drug-resistant bacteria on blood culture
We collected data on drug resistant bacteremia from two trials with 502 patients [21,29]. There were four cases among 249 patients randomized to receive single drug and zero cases among 253 patients randomized to receive combined drugs (Fig. 7D). There was no substantial difference between single and combined antibiotic use (RR 5.00, 95% CI 0.60–41.90, p=0.14).
Fever
Fever was reported in one trial [16]. There were 15 cases of fever among 71 patients randomized to receive single drug and five cases in 86 patients randomized to receive combined drugs (p=0.009, Fig. 7E).
UTI
We collected data on UTI from three trials with 659 patients [16,21,29]. There were 26 events among 320 patients randomized to receive single drug, and six among 339 randomized to receive combined drugs (Fig. 7F). The meta-analysis was substantial and favored combined antibiotic use (RR 4.64, 95% CI 2.01–10.74, p=0.0003).
Hospitalization
Data on hospitalization could be collected from three trials with 659 patients [16,21,29]. There were 23 hospitalizations among the 320 patients randomized to receive single drug and four among the 339 patients randomized to receive combined drugs (Fig. 7G). The comparison was substantial and favored combined antibiotics (RR 5.91, 95% CI 2.20–15.87, p=0.0004).
Discussion
TRPB is currently an essential procedure for diagnosis of Pca [38]. It is a frequently performed procedure in urology that millions of men undergo PB throughout the world each year as part of the accepted diagnostic pathway for Pca [39]. UTI, fever, sepsis, and even death have been reported as complications after a PB procedure, particularly by TR route. The goal of antibiotic prophylaxis for patients undergoing TRPB is to prevent these serious complications. Most RCTs and a few case-control studies established the efficacy of antibiotic prophylaxis in TRPB [13,19,23,25,27,28,31,34,36]. In addition, we noted that a large variety of antibiotic regimens were used in these studies.
FQs are the most frequently used antibacterial prophylaxis agents for TRPB. A recent international survey reported that 98.2% of the patients undergoing biopsy in 84 countries received antibiotic prophylaxis, FQs being the drug most commonly prescribed (92.5%) [1]. FQs are appropriate because of their high bioavailability, antimicrobial spectrum, and high concentrations in prostatic tissues. The efficacy of FQs in decreasing the risk of UTI after TRPB have been well demonstrated in a few RCTs published approximately 10 years earlier [13,25,27,34,36].
Although the incidence of UTI was well controlled for a period of time, the incidences of infectious complications after TRPB have increased again during the recent years. A Canadian retrospective study evaluated 75,000 Canadian men who underwent TRPB between 1996 and 2005 and determined that infection-related hospital admissions had increased four-fold in this time period (p<0.001) [8]. Recent studies have demonstrated increasing rates of infectious complications and the need for hospitalization after TRUS-guided biopsies owing to FQ-resistant bacteria [10,40], with rates of FQ-resistant Escherichia coli of the intestinal flora ranging from 13% to 22% [40]. Lange et al. reported that 96% of men (24 cases) with post-biopsy sepsis had FQ-resistant E. coli [41]. Therefore, these findings raised concern regarding FQ-resistant strains and the risk of sepsis.
However, probably because of the greater incidence of UTI and drug resistance reported recently, both AUA and EAU no longer highly recommend fluoroquinolones for antibiotic prophylaxis as they used to. This raised a lot of debates that how urologists could use prophylactic antibiotics rationally and effectively.
Despite routine antibiotic prophylaxis, infectious complications are a continued threat following PB, with greater incidence of infection and drug resistance. If the empirical use of prophylactic antibiotic persists (FQ being the most common), an increasing number of patients would require intensive in-patient treatment. Furthermore, given that in a single case hospitalization for sepsis represents elevated costs and poses a serious threat for the patient's health and may be life-threatening, any proposed regimen must provide adequate proof of safety and effectiveness. Therefore, we attempted to evaluate the efficacy of augmented prophylaxis reported by several new studies to determine if it is suitable to propose an alternative to the current regimen of antibiotic prophylaxis [16,21,29].
Augmented prophylaxis refers to the combined use of antibiotic prophylaxis to minimize the possibility of infection [42–46]. On the basis of the studies involved in this meta-analysis, most studies added one type of aminoglycoside or cephalosporins (usually one IM or IV dose) to fluoroquinolone or other antibiotic treatment. The combined use of prophylactic antibiotics not only reduced the incidence of UTI, the rate of fever, and hospitalization, but also lowered the rate of positive urine and/or blood culture (although no substantial results were acquired, a trend towards lowering for the rate of positive urine and blood culture appeared in this review). Furthermore, the reduced drug-resistant bacteria in urine and blood cultures were also promising.
The foremost benefit that was achieved from augmented prophylaxis was the lower incidence of infective complications, which is directly related to the patients' health. Second, although the use of combined antibiotic represents a greater cost for a single patient, such preventive measure may be more cost-effective for patients involved as a whole. Third, drug-resistant bacteria could be reduced, which would translate into lower risk of nosocomial infections. Nevertheless, the greatest concern still lies in the antibiotic resistance. If augmented prophylaxis fails to ameliorate bacterial resistance in the future, will it be necessary to increase the number of drugs used (i.e., three types of drugs together) or use the most potent agent? Furthermore, the use of combined antibiotic treatment would be more costly for one patient, although a single dose is usually prescribed. The IV or IM administration is also more painful and inconvenient for some patients than oral administration. Finally, although Carignan et al. [7] claimed that a single dose of aminoglycoside did not lead to substantial nephrotoxicity or ototoxicity, the potential risk of side effects should also be considered.
To use augmented prophylaxis more reasonably, the patients with risk factors should be identified and treated carefully. Perhaps patients with definitive risk factors for post-biopsy septicemia, such as diabetes mellitus, immunosuppressive treatment, history of fluoroquinolone use, endocarditis or artificial cardiac valves, chronic obstructive pulmonary disease, and performance of the biopsy several months before may benefit from targeted prophylaxis [3,7,40]. The other uncertain risks such as age>80 y, indwelling catheter, former pyuria, history of prostatitis, and prostatic enlargement should not be ignored.
Despite great challenges, there are some other methods currently under debate to prevent the infection following PB. First, several studies have assessed whether technical modifications can influence infection rates. For instance, transperineal biopsy has been suggested as a possible alternative way to perform the technique, although Shen et al. found no qualitative difference in infection rates in a secondary analysis of studies on transrectal versus transperineal biopsy [47]. Second, microbiological sampling of the fecal flora prior to biopsy could be utilized to identify susceptibility to specific agents [40]. Third, pre-biopsy bowel preparation was also reported in our previous work to reduce the infection [48]. Then, a smaller 18-gauge needle for biopsy could also be used [49]. And the last but not least way to reduce the post-biopsy infection is to well consider the indication for TRPB and reduce the total number of TRPBs [50].
Conclusion
Our study shows that prophylactic antibiotics are beneficial for the reduction of infective complications after TRBP. A single-dose or short-course treatment and the oral administration with some type of antibiotic are preferred. Depending on the recommended use of one type of antibiotic, an additional dose of another antibiotic could be added to minimize severe infection and drug resistance, particularly for patients at high risk.
Footnotes
Acknowledgments
This study was supported by the Prostate Cancer Foundation Young Investigator Award 2013, the National Natural Science Foundation of China (Grant No. 81300627, 81370855, and 30901484), and Programs from Science and Technology Department of Sichuan Province (Grant No. 2013SZ0006 and 2014JY0219).
Author Disclosure Statement
The authors have no conflicts of interests to disclose.