
Abstract
Abstract
Background:
Fournier gangrene (FG) is a fulminant necrotizing infection of the perineal, perianal, and periurethral tissues. The Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) scale is used for diagnosis of necrotizing fasciitis. However, data on its relevance and usefulness in FG are lacking. The aim of this study was to evaluate the utility of the LRINEC scale in predicting the outcome of FG.
Methods:
This retrospective case study included 41 patents with FG treated at our institution from 2000 to 2013. The patients were divided into survivors and non-survivors.
Results:
The mortality rate was 22%. The median age (75 vs. 62.5 y; p = 0.013), rate of co-existing diabetes mellitus (66.7% vs. 3.1%; p < 0.001), and median affected skin surface (4% vs. 1%; p < 0.001) were greater in the non-survivors. Seven of nine patients (77.8%) who did not survive (compared with 37.5% who survived) had a polymicrobial infection (p = 0.032). Of all the causative pathogens isolated, Proteus mirabilis was more common in non-survivors (55.6% vs. 6.3%; p = 0.001). The median calculated LRINEC score for survivors was 5 compared with 10 for the non-survivors (p < 0.001). Regression analysis showed that all the aforementioned variables, except for polymicrobial culture, were significant risk factors for predicting death. The area under the receiver operating characteristic curve for the LRINEC score was the highest, 0.976 (95% confidence interval 0.872–0.999; p < 0.0001), and the cut-off value was ≥9 with 93.7% specificity and 100% susceptibility for the prediction of a lethal outcome.
Conclusions:
The LRINEC score could be used for prediction of disease severity and outcomes. A threshold of 9 could be a high-value predictor of death during the initial evaluation of patients with FG.
F
The diagnosis of FG is based on symptoms, which include genital discomfort and pruritus during the prodromal period, followed by scrotal edema, genital erythema, scrotal pain, partial necrosis, induration, crepitation, feculent odor, and fever. Some of these symptoms may be absent in a particular case [3]. The common laboratory findings are non-specific. Therefore, early clinical identification and differentiation of FG from other soft tissue infections is difficult. Despite aggressive treatment, the mortality rate from FG is still high, ranging from 3% to 67% [4].
Some factors are most often associated with a higher mortality rate from FG; such factors include diabetes mellitus (DM), chronic kidney failure, congestive heart failure, severe sepsis on admission, coagulopathy, alcoholism, and malignant disease [4–8]. However, currently, there is no consensus on the usefulness of these factors for the prognostication of the severity of FG and death from it.
The literature contains several prognostic tools for the prediction of the FG mortality rate, the most popular of which were compared by Roghmann et al. [9]. None of these tools—the FG Severity Index (FGSI), the Uludag Fourier Gangrene Severity Index (UFGSI), the age-adjusted Charlson Comorbidity Index (ACCI), or the surgical Apgar score (sAPGAR)—was superior when predicting FG outcomes, and, according to the author, all of these scoring systems can be used for the prognostication of death [9].
In our study, we evaluated an unusual, simple, and objective system, the Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score. The LRINEC is based on routine laboratory investigations, including C-reactive protein (CRP), white cell count, and the hemoglobin, sodium, creatinine, and glucose concentrations, which are easily available at most centers and can help evaluate the severity of necrotizing fasciitis (NF) and predict death. The LRINEC is a laboratory measurement score capable of identifying NF even if the clinical picture is questionable [10]. The aim of this study was to evaluate the utility of the LRINEC scale in predicting death from FG as a form of necrotizing fasciitis (NF), reviewing our experience in the management of FG over the last 13 years.
Patients and Methods
This retrospective case study examined the data of all patients with FG treated at our tertiary-care Department of Urology between January 2000 and December 2013. The patients' data were obtained from the hospital archives. A total of 41 patients were found, and they were distributed into two groups: survivors and non-survivors. The data collected from the medical records of those patients were age, gender, predisposing factors, disease etiology, duration of the symptoms before admission, antibiotic therapy given, and the length of the hospital stay. The laboratory and culture findings and the affected skin surface measurement data also were collected for all patients. The extent of the necrotic area was measured using a modified body surface area nomogram applied routinely to assess the extent of burns. The penis, scrotum, and perineum were measured as 1% and the ischiorectal fossa as 2.5% [11,12].
All patients underwent immediate surgical treatment, including abscess drainage and aggressive surgical debridement, with resection of all necrotic skin, underlying subcutaneous tissue, fascia, and muscle to the point where viable tissue was evident. Every patient was given empiric antibiotic therapy, which was modified according to the results of susceptibility tests. The LRINEC score was calculated according to laboratory data (CRP, white blood cell count, concentrations of hemoglobin, sodium, creatinine, and glucose) obtained immediately after arrival [10]. The score was stratified by survival or death. The mortality rate was calculated on the basis of disease-related deaths.
Statistical analysis was performed for the identification of significant differences between the patients who survived and the patients who died. The χ2, Student t, and Mann-Whitney tests were used as appropriate. A binary logistic regression was performed to determine associations between significant factors and death by estimating odds ratios (ORs) and 95% confidence intervals (Cis). The power, defined as the ability of the LRINEC score and other factors to distinguish survivors from non-survivors, was assessed by calculating the area under the receiver operating characteristic (ROC) curve, estimating the standard error (SE) and 95% CI. The optimal cut-off value for predicting death was identified as the score yielding the best Youden index (maximum [susceptibility + specificity − 1]) for the scoring model. Statistical significance was defined as p < 0.05.
Results
During the period between January 2000 and December 2013, we identified 40 male patients and 1 female patient with FG. Thirty-two patients recovered (the survivors group), and 9 patients died (the non-survivors group). The mortality rate thus was 22%. The main causes of death were severe electrolyte disorders (hypokalaemia and hypomagnesemia), sepsis, acute respiratory distress syndrome, and failure of multiple organs and systems.
The patients' median age, the rate of co-morbidity with DM, and the median affected surface area were significantly different in the two study groups, as shown in Table 1. The variables that were significantly different were subsequently included in the binary logistic regression analysis. This analysis revealed that age (OR 1.12; 95% CI 1.012–1.236; p = 0.028), DM (OR 62; 95% CI 5.479–701.53; p = 0.001), and the affected surface area (OR 20.8; 95% CI 2.41–179.78; p = 0.006) were significant risk factors for death from FG.
Data shown as median (25th–75th interquartile range).
On admission to the hospital, before the first surgical intervention, all patients received empiric antibiotic therapy, which usually consisted of intravenous cefuroxim and metronidazole. These two antibiotics were administered in 78.1% and 77.8% of the cases in the survival and non-survival groups, respectively, and this difference was not statistically significant. Microbiologic cultures were carried out in all patients, and antibiotic therapy was changed according to the results. A single microorganism was isolated in 13 patients (31.71%), two or more organisms were found in 19 patients (46.3%), and no pathogens were detected in 9 patients (21.95%). The micro-organisms most frequently isolated were Escherichia coli, Enterococcus, and Proteus mirabilis. The culture results are presented in Table 2.
The rate of polymicrobial infection was greater in non-survivors than in survivors (respectively, 77.8% vs. 37.5%; p = 0.032), but this factor was not significant when predicting death in the regression analysis: p = 0.063. Proteus mirabilis as the causative pathogen was detected more often in non-survivors than in survivors (55.6% vs. 6.25%; p = 0.001), and it also was a significant risk factor for death in the regression analysis (OR 18.75; 95% CI 2.685–130.94; p = 0.003).
Laboratory findings obtained immediately after the arrival and the calculated LRINEC points in both groups are shown in Table 3. At the time of admission, CRP, sodium, and creatinine concentrations differed in survivors and non-survivors. The calculated median LRINEC score for survivors was 5 compared with 10 in the non-survivors (p < 0.001). Only 2 of 32 (6.3%) survivors and all non-survivors had LRINEC scores of 9 or above. The LRINEC score was a significant factor for the prediction of death in the regression analysis. An increase in the LRINEC score by one point elevated the risk of death 7.7-fold (OR 7.74; 95% CI 1.33–45.032; p = 0.023).
Data shown as median (25th–75th interquartile range).
We conducted a ROC analysis for all significant factors detected in the regression analysis (Fig. 1). The area under the curve for age was 0.799 (95% CI 0.638–0.959; p = 0.007), for DM 0.818 (95% CI 0.624–1.00; p = 0.004), and for Proteus mirabilis infection 0.747 (95% CI 0.534–0.959; p = 0.025). The LRINEC score had the largest area under the ROC curve: 0.976 (95% CI 0.934–1.00; p < 0.0001). The cut-off value for the LRINEC score was ≥9, with 93.7% susceptibility and 100% specificity for the prediction of a lethal outcome of FG.
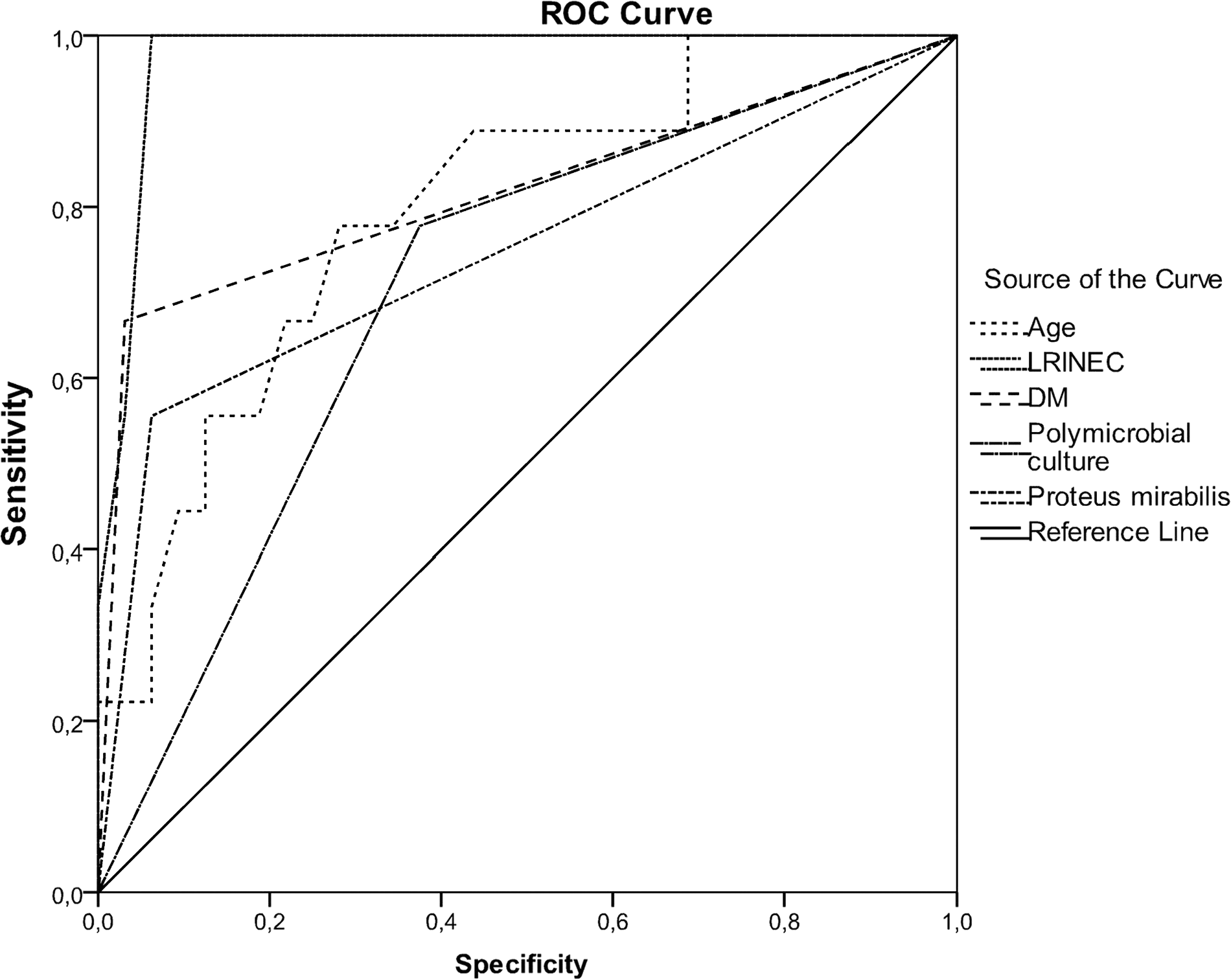
Receiver operating characteristic curves for factors associated with death caused by Fourier gangrene.
Discussion
Fournier gangrene is a fulminant and life-threatening disease characterized by NF of the perineal and genitourinary area resulting from a monomicrobial or polymicrobial infection. In spite of developing medical technology and experience, FG still is often a fatal disease, with a mortality rate ranging from 3%–67% [4]. In our study, the mortality rate was 22%, which corresponds to the rates found in other more recent studies [6,11,13–15]. A proper estimation of the mortality risk can help physicians manage the treatment and expectations in FG cases.
According to the literature, FG can occur in patients of all ages. The median age in this study was 67 years, which coincides with data presented by other authors [5,6,14,15]. Survivors were younger than non-survivors (62.5 vs. 75 years; p = 0.013). Regression analysis showed that an increase in age by one y significantly increased the risk of a lethal outcome (OR 1.12; p = 0.028). The ROC analysis revealed that the cut-off value for this factor was 70 y, with 78% susceptibility and 72% specificity for the prediction of death. Despite the finding that older patients have, logically, a greater risk of death, there are only a few studies in which age was found to be a risk factor [14]. In most series, the survivors were younger, but age did not influence the mortality rate [5,7,13]. The influence of gender on mortality risk has been investigated in some studies [16,17], but we cannot perform a proper analysis because we had only one female patient. This is not unexpected, as necrotizing fasciitis of the genital area occurs almost entirely in males.
There are several factors and scoring systems that are used for the prediction of death in patients with FG. Diabetes mellitus as a significant risk factor for death has been mentioned in several publications [18–21]. Nevertheless, there are studies in which DM has been detected only as the most common co-morbidity but not as a risk factor for FG outcomes [5,16,22–24]. In our study, DM was present in seven cases (17.1%) and was significantly more common in non-survivors than in survivors, 66.7 vs. 3.1%, respectively (p < 0.001). Mono-factorial regression analysis showed that patients with DM had a 62-fold greater risk of death (OR 62; 95% CI 5.479–701.53; p = 0.001), and our data confirm the reports of other authors who found DM to be a risk factor for death [18–21].
It is accepted that FG is associated with a variety of pathogens, both aerobic and anaerobic, and a correlation between mortality rates and bacterial types has been reported [19,20,25]. Escherichia coli, Proteus, Klebsiella, Bacteroides, Streptococcus, and Staphylococcus are the micro-organisms most commonly detected in patients with FG [11,26]. Polymicrobial infections usually predominate over monomicrobial ones, and the rate of such infections ranges from 35% to 83.8% [5,7,27]. In our study, polymicrobial infections constituted almost half of our cases (46.3%) and presented at significantly greater rates in non-survivors than in survivors (77.8% vs. 37.5%; p = 0.032). However, the regression analysis did not confirm polymicrobial infection as a risk factor for death (p = 0.063). Escherichia coli, Enterococcus spp., and Proteus mirabilis were commonly isolated in this study, but only Proteus mirabilis as a causative pathogen was identified as a risk factor for a lethal outcome. Patients with Proteus mirabilis infection had a 19-fold greater risk of death (OR 18.75; p = 0.003). The significance of this factor was confirmed by the ROC analysis; the area under the ROC curve was 0.747 (p = 0.025).
In our study, the median affected surface area was larger in patients who did not survive (4% vs. 1%; p < 0.001). The median affected area in our study was 2%. An affected area exceeding this figure was detected in 3.4% of survivors and 66.7% of non-survivors. The regression analysis revealed that an increase in the affected surface area by 1% elevated the mortality risk almost 21-fold (OR 20.8; p < 0.001). The affected area as a risk factor has been pointed out by other authors as well [5,7,14,15]. Even though this factor significant in our analysis, the retrospective manner of data collection requires our results to be interpreted with caution. For this reason, we did not include affected area in the ROC analysis. On the other hand, the comparison of our and the aforementioned studies is complicated because different methods were used for the calculation of the area of affected skin.
Early diagnosis could be associated with better outcomes of FG [7–11,13,14]. Korkut et al. drew more strict conclusions. They observed a greater mortality rate in patients in whom the duration of symptoms before admission to the hospital was 7 d or longer [8]; however, this view has not been confirmed by other authors [5,28]. We assume that the significance of this factor alone is controversial. In our study, the median duration of symptoms before admission was the same in survivors and nonsurvivors: 4 d. Other important issues are the time from admission to surgical intervention and the number of debridements performed in each patient. As pointed by Sugihara et al. [29], surgical intervention within 2 d after admission correlates significantly with a lower case fatality rate. In our study the median times from admission to the first surgical intervention were 3 h vs. 6 h in the survival and nonsurvival groups (p = 0.255). This result shows that the surgical tactic applied in our institution is appropriate and did not influence the mortality rate.
Various laboratory findings such as serum CRP; sodium, creatinine, and hemoglobin concentrations; and leukocyte count have been investigated as predictors of FG outcomes, but the data are conflicting [5,6,14,15,28]. We found that the sodium, creatinine, and CRP concentrations in the serum differed in the two study groups. However, a more detailed analysis of individual effects was not performed because these laboratory factors are included in the LRINEC score.
A number of scoring systems have been evaluated to enable a more reliable prognosis of FG outcomes. The most popular prognostic tool is the FGSI, which was first described by Laor et al. [12]. A score >9 is associated with a 75% probability of death, whereas a score of ≤9 is associated with a 78% probability of survival. However, the accuracy of this method remains controversial [14,28]. Although some evidence confirms the prognostic value of the FGSI [5,14,15], other data suggest that the system cannot be used safely in clinical practice to predict survival [30]. The necessity for blood gas measurement is the biggest deficiency in the FGSI in routine practice. Another scoring system combining age and disease dissemination with the FGSI score (UFGSI) showed a susceptibility of 94% and a specificity of 81% and was suggested by the authors of that paper as a powerful tool for the prediction of death from FG [31]. There is a recent study comparing FGSI, UFGSI, ACCI, and sAPGAR for predicting FG outcomes where it was concluded that all scores are useful for the prediction of death, and even though the UFGSI includes more variables, it does not seem to be more powerful than the FGSI. The authors suggested applying ACCI and sAPGAR in daily practice, as they are more easily calculated, are generally applicable, and are better validated than the FGSI [9]. Our study was retrospective. Therefore, the criteria for analysis were determined in advance, and we were unable to calculate scores such as FGSI or Acute Physiology and Chronic Health Evaluation (APACHE) II because of the lack of certain data required by these methods.
We used the LRINEC score, which initially was evaluated for the determination of NF severity. Because FG is a form of NF, our hypothesis was that the LRINEC score would be sensitive in cases of FG also. The hematologic and biochemical changes in NF develop early in the disease; and using the LRINEC score, patients can be distributed into high-, moderate-, and low-risk categories even when the clinical picture is only suggestive [10]. The prognostic value of the LRINEC score to predict the severity of NF was analyzed in several studies [10]. However, there is very little information about the validation of the LRINEC score with FG, and we found no studies on the feasibility of using the LRINEC score to predict lethal outcomes of FG. The LRINEC score is a simple and objective system based on routine laboratory investigations that are easily available at most centers.
The median LRINEC score in all study patients was six points, and a significant difference was detected when comparing survivors and non-survivors (5 vs. 10; p < 0.001). An increase in the LRINEC score by one point elevated the risk of death 7.7-fold. The area under the ROC curve for the LRINEC score was 0.976, and the detected cut-off value was ≥9, which has 93.7% susceptibility and 100% specificity for the prediction of death. Our findings show that a LRINEC threshold of 9 during the initial evaluation of patients with FG is a high-value predictor of death.
Even though age, DM, Proteus mirabilis infection, and the percentage of the affected skin surface were independent predictors of death in our study, we suppose that the LRINEC score system is the most powerful predictor of death in FG cases. To the best of our knowledge, this is the first study to evaluate the feasibility using of the LRINEC score to predict FG outcomes.
Our study has some limitations. The number of patients is small because of the rarity of FG. Only multi-center studies could increase the number to help us reach more powerful conclusions. The retrospective study design is another limitation. Although all laboratory data were collected without difficulties, the affected skin area measurement should be interpreted with caution because of possible variation in the method used during the long study period. The last but perhaps most important limitation is the lack of validation of the value of the LRINEC score for prediction of death in FG cases. Therefore, more prospective multi-center studies, as well as LRINEC score comparison with other scoring systems, are needed to confirm our findings.
The strength of the study is its simplicity: All the laboratory studies could be performed routinely, and the LRINEC score could be calculated easily. To our knowledge, this is the first study to evaluate the utility of the LRINEC score for predicting FG outcomes.
Conclusions
Fournier gangrene is a severe condition with a high mortality rate. Our study showed that the LRINEC score could be used for prediction of disease severity and outcomes in patients with FG. The LRINEC score threshold of 9 during the initial evaluation of patients has a high specificity and susceptibility to lethal outcomes. We believe that the LRINEC score based on routine laboratory investigations could be useful in daily practice for the prediction of fatal outcomes of FG.
Footnotes
Author Disclosure Statement
No competing financial interests exist.