
Abstract
Abstract
Background:
The incidence of nosocomial infections caused by multi-drug- and extended-drug resistant strains of Acinetobacter is constantly increasing all over the world, with a high mortality rate. We analyzed the in-hospital data on the sensitivity of Acinetobacter baumannii isolates and correlated them with antibiotic treatment and clinical outcomes of nosocomial infections over a 17-mo period.
Methods:
Retrospective analysis was performed at the Clinical Center “Bezanijska kosa,” Belgrade, Serbia. Microbiologic data (number and sensitivity of A. baumannii isolates) and clinical data (medical records of 41 randomly selected patients who developed nosocomial infection caused by A. baumannii) were matched.
Results:
Acinetobacter baumannii, detected in 279 isolates and obtained from 19 patients (12% of all samples), was resistant to almost all antibiotics tested, including carbapenems, with the exception of colistin and tigecycline. It was obtained most often from the respiratory tract samples. Empiric treatment of the nosocomial infections (pneumonia in 75% of cases) involved cephalosporins, metronidazole, and carbapenems (80%, 66%, and 61% of patients, respectively), whereas tigecyclin and colistin were used primarily in targeted therapy (20% and 12% of patients, respectively). The mortality rate of patients treated empirically was significantly higher (p < 0.01), reaching 100% in the elderly.
Conclusions:
Nosocomial A. baumannii infections represent a significant clinical problem because of their high incidence, lack of susceptibility to the most commonly used antibiotics, and the often inappropriate treatment, which favors the development of multi-drug-resistant strains.
A
The importance of hospital-acquired infections caused by these bacteria, especially by Acinetobacter baumannii, has increased during the last decade [3,4]. Indeed, the incidence of nosocomial infections caused by Acinetobacter spp. is increasing constantly [5]. Immunocompromised patients, patients with permanent catheters, post-operative patients, patients in the intensive care unit (ICU), as well as patients who have previously been exposed to a wide range of antibiotics, parenteral nutrition, and mechanical ventilation are most susceptible to these infections [6]. The most common A. baumannii infections are pneumonia, skin/soft tissue infections, urinary tract infections, meningitis, and bacteremia/sepsis with a mortality rate of 8%–32%. These data suggest that infections with Acinetobacter spp. must be treated adequately [7,8].
During the 1970s, A. baumannii was sensitive to almost all antibiotics, whereas carbapenems remained the last reliable treatment option by the end of the 1990s [6]. Today, A. baumannii is multi-drug-resistant (MDR) with increasing resistance to antimicrobial agents that presents a serious worldwide problem [9]. In 2008, the rate of carbapenem resistance was 54%, and the results of studies published during 2014 indicate that carbapenem resistance increased to more than 65% in Europe and the United States [8,9]. Resistance of A. baumannii increased 50-fold (from 1% to 51%) during the 12-y period, whereas Pseudomonas aeruginosa resistance increased only two-fold according to a Korean study [10].
The objectives of this study were to perform a retrospective analysis of the sensitivity of A. baumannii according to the findings of hospital microbiology laboratories, the choice of antibiotics used in empiric and targeted antimicrobial therapy of A. baumannii infections, and the treatment outcomes of patients with hospital-acquired infections caused by this organism.
Patients and Methods
Antibiotics
The retrospective cohort study was carried out at the University Medical Center “Bezanijska kosa,” Belgrade, Serbia, a 360-bed tertiary-care center. Both microbiology and clinical efficacy data were analyzed.
First, antimicrobial surveillance was conducted utilizing in-patient microbiology laboratory records for 17 mo (June 1, 2013–November 1, 2014). Identification of isolated cultures of bacteria and antibiotic susceptibility testing in the laboratory was performed using the Vitek2 system (bioMérieux, Mercy l'Etoile, France) according to the manufacturer's recommendations. The total number of isolates was 279.
Susceptibility of A. baumannii was tested to the following antibiotics: Amikacin (n = 263), amoxicillin (n = 67), amoxicillin–clavulanic acid (n = 267), ampicillin (n = 190), azithromycin (n = 4), cefahlor (n = 98), cefazolin (n = 5), cefepime (n = 265), cefixime (n = 247), cefoxitin (n = 11), cefotaxime (n = 266), ceftazidime (n = 261), ceftriaxone (n = 263), cefprozil (n = 96), cefuroxime (n = 258), cephalexin (n = 258), chloramphenicol (n = 9), ciprofloxacin (n = 266), colistin (n = 168), doripenem (n = 2), ertapenem (n = 96), fosfomycin (n = 8), gentamicin (n = 263), imipenem (n = 266), levofloxacin (n = 227), lincomycin (n = 1), meropenem (n = 274), minocycline (n = 1), nitrofurantoin (n = 13), ofloxacin (n = 214), pipemidic acid (n = 17), piperacillin (n = 260), piperacillin–beta-lactamase inhibitor (n = 243), rifampicin (n = 25), sulbactam–ampicillin (n = 207), tetracycline (n = 12), ticarcillin (n = 5), tigecycline (n = 59), tobramycin (n = 5), and trimethoprim–sulfamethoxazole (n = 276).
Subgroup Analysis
In the second phase, a sample of 41 adult patients was selected randomly. All of these patients had been admitted for >48 h to the University Medical Center “Bežanijska kosa” before the antimicrobial surveillance was conducted. They had symptoms and signs of hospital-acquired infection by A. baumannii during the trial period. Patient demographic, epidemiologic, and clinical data were obtained. Personal data were not used, and the results could not be correlated with particular patients. For this type of study, informed consent is not required. Internationally accepted definitions proposed by the U.S. Centers for Disease Control and Prevention (CDC) and national regulations (Rulebook on the Prevention, Early Detection and Eradication of Infection of the Republic of Serbia from 2013) were used for the definition of nosocomial infections [11,12].
Empiric antimicrobial therapy was the initial application of antibiotics based on experience and adjusted to the clinical picture, whereas targeted therapy was the use of antibiotics based on the results of susceptibility testing [13]. Of note, patients on empiric therapy never received targeted therapy during their hospital stays. The success of the therapy was evaluated according to the outcome of treatment (cure or survival) of patients.
Data analysis
Data were analyzed by descriptive statistics, involving the calculation of the frequency distribution, arithmetic mean (X-bar), standard deviation (SD), median (M), and interquartile range (IQR 25–75). Differences among the categories were tested using χ2 and the Fisher exact tests. Values of p < 0.05 were considered statistically significant. All tests were two-sided. The statistical program IBM SPSS Statistics 20.0 was used for all calculations.
Results
According to the hospital microbiology laboratory record, A. baumannii was present in 279 of 2,325 isolates (12%) collected from 192 patients during the 17 mo of the study. In other words, Acinetobacter isolates represented 26% of all gram-negative pathogens isolated. Acinetobacter baumannii usually was isolated from the upper and lower respiratory tract (127/279); i.e., from nasal and pharyngeal swabs, endotracheal tube, or sputum. In addition, A. baumannii was isolated from central venous catheters (25/279), blood (36/279), and the incision (55/279) (Table 1).
Post-operative surgical site n = 41; traumatic wound n = 2; pressure ulcer n = 12.
The sensitivity of the isolated strains of A. baumannii to the antibiotics is presented in Fig. 1, and the resistance of A. baumannii to carbapenems; i.e., to imipenem (251/279), meropenem (255/279), and ertapenem (96/279), is presented in Fig. 2.
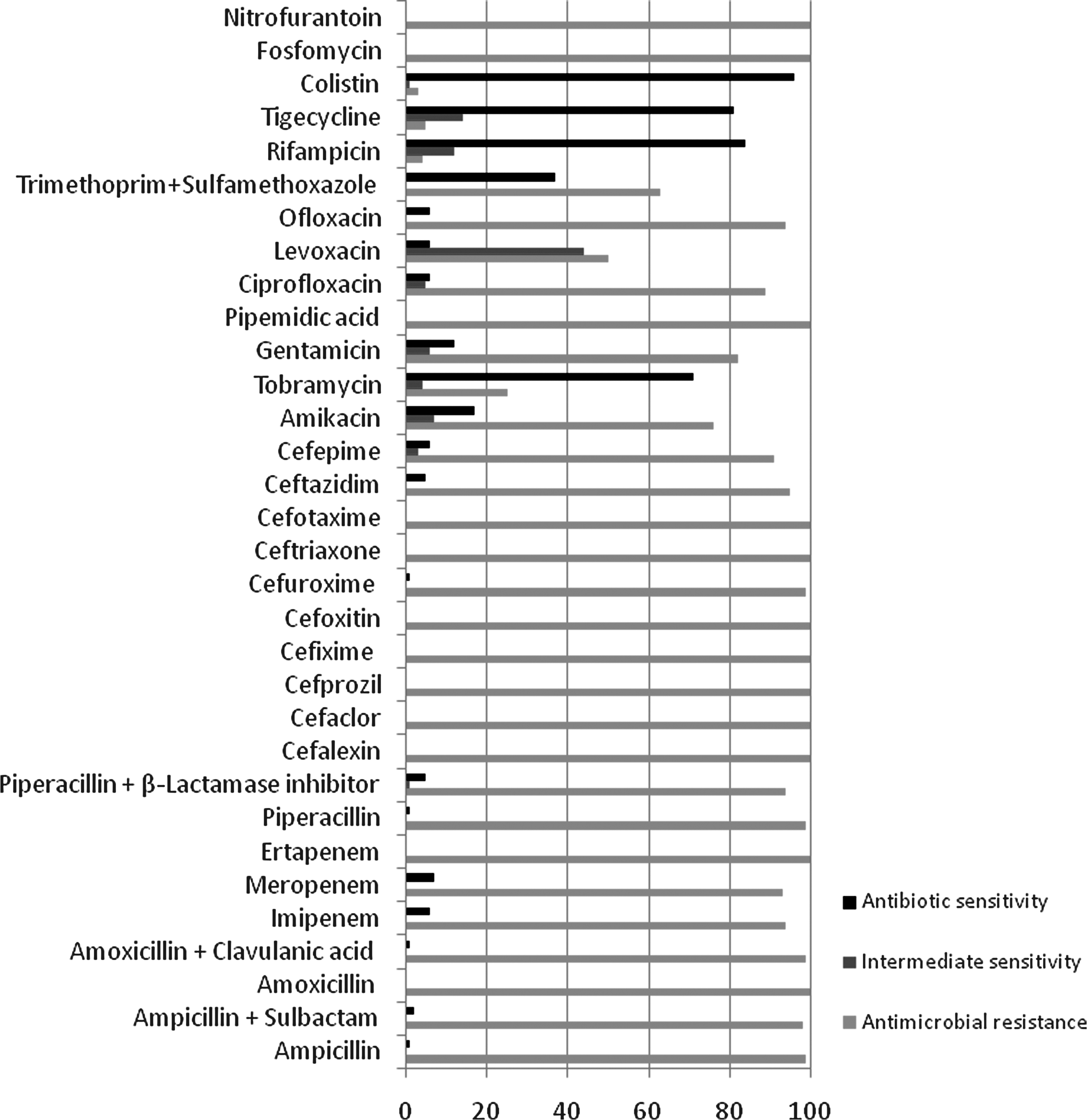
Sensitivity of Acinetobacter baumannii to antibiotics, June 2013–November 2014.
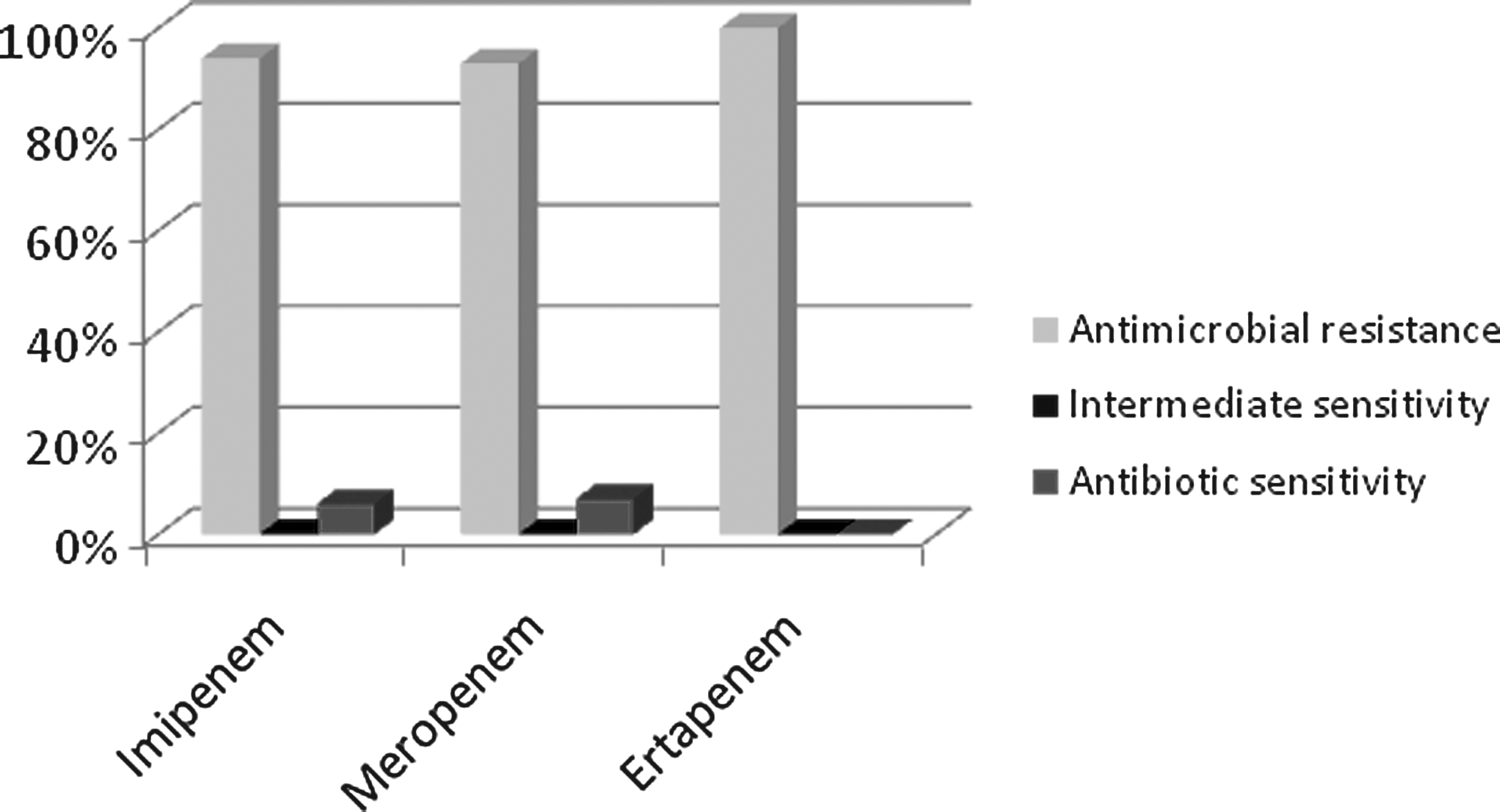
Sensitivity of Acinetobacter baumannii to carbapenems, June 2013–November 2014.
Analysis of the whole sample of 192 patients showed that slightly more male than female patients suffered from A. baumannii infection (60% and 40%, respectively).
Patients with no signs of infection were excluded from further analysis, and the data from the 41 patients with hospital-acquired infections (pneumonia, sepsis/bacteremia, surgical site infections [SSIs], and urinary tract infections) were analyzed statistically. There were 22 men (54%) and 19 women with an average age of 70 ± 12 y (x-bar ± standard deviation) and 73 y (M) (IQR 25–75 = 62–79 y). The youngest patient was 39 y, and the oldest was 91 y. Distribution of patients with hospital-acquired A. baumannii infections by age group and their survival are shown in Fig. 3.
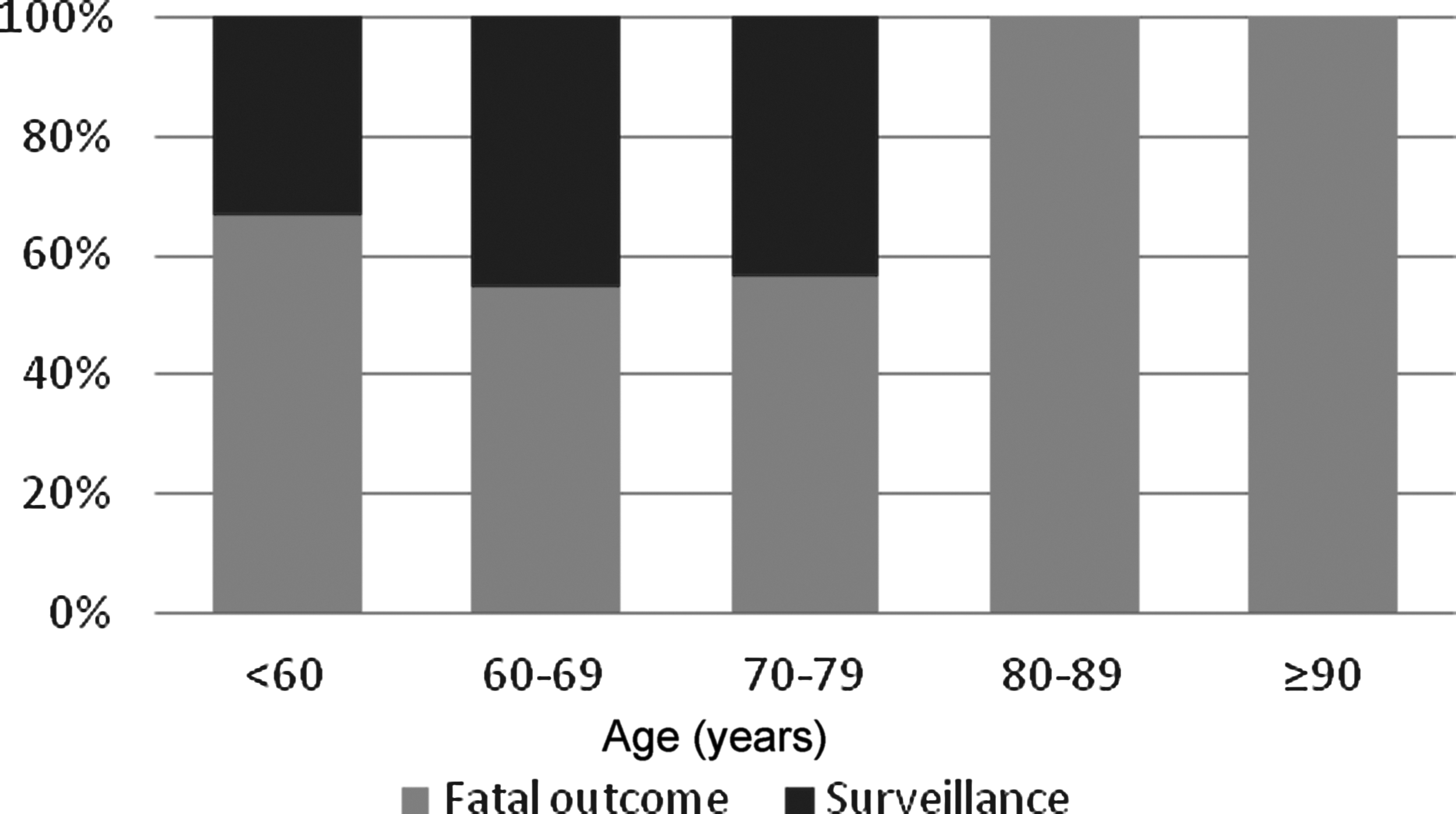
Fatal outcome of different age cohorts of patients with Acinetobacter baumannii infection.
Nineteen patients were admitted to the internal medicine ward, whereas 22 patients were admitted to the surgical ward. The average time from hospital admission to the isolation of A. baumannii was 13 ± 10 d, or 9 d (M), with an IQR 25–75 of 6–21 d.
Mixed infections were observed in 17 of the 41 patients. Twenty-seven bacterial isolates were recovered, with similar numbers of gram-positive and gram-negative organisms (13 and 14 of 27, respectively). Coagulase-negative staphylococci, Klebsiella pneumoniae, and Pseudomonas aeruginosa were detected in many patients (6, 5, and 5, respectively).
Thirteen of 28 cases of pneumonia were caused by mixed infections (19 isolates in total). There were equal numbers of gram-positive and gram-negative organisms, with a predominance of K. pneumoniae, P. aeruginosa, and coagulase-negative staphylococci (5, 4, and 5, respectively).
Finally, one of the four cases of Acinetobacter pneumonia was caused by a mixed infection with coagulase-negative staphylococci and Staphylococcus aureus.
The antibiotics used most often are shown in Table 2. All patients were treated for several days before we received data about the bacteria isolated and the results of antibiotic susceptibility tests (i.e., they received empiric therapy). The antibiotics used most often for empiric therapy were third-generation cephalosporins (80%), metronidazole (66%), carbapenems (61%), and vancomycin (54%).
Colistin, linezolid, piperacillin/tazobactam, aztreonam, clindamycin.
The distribution of patients according to treatment outcome is shown in Table 3. There was a highly significant difference in the survival of patients on empiric and targeted therapy. That is, the mortality rate was significantly lower in the group treated on the basis of susceptibility testing (p < 0.01).
Patients treated only with empiric antibiotics, without the introduction of targeted antimicrobial therapy.
Four of the 41 patients with Acinetobacter baumannii infection died of complications of their primary condition, not of the infection. Accordingly, they were omitted from this analysis.
The most common types of hospital-acquired infections were pneumonia, SSI, bacteremia/sepsis, and urinary tract infections (75%, 11%, 11%, and 3%, respectively). As for the group as a whole, there was a great difference in the survival of patients with pneumonia treated empirically and those on targeted therapy (p < 0.01).
Discussion
Multi-resistant Acinetobacter has become a significant therapeutic problem in hospitals [14]. More than 40 years ago, it was realized that the presence of gram-negative bacteria in the equipment for mechanical ventilation might pose a risk for nosocomial pneumonia [15]. The increase in the number of hospitalized older patients with chronic diseases, as well as the frequent use of invasive procedures, favor the development of nosocomial infections caused by Acinetobacter spp. [2].
Nosocomial infections caused by A. baumannii create a substantial economic burden for hospitals and healthcare budgets [16]. The annual cost of treating ICU-admitted patients with A. baumannii colonization (prevalence 4%) at the University of Pittsburgh Medical Center ranged from US$400,000 to US$1,600,000 in 2008. The mean cost to a hospital for each case is estimated to be US$8,000 to US$29,000 with a 20% to 70% probability that the colonized patient will develop an infection.
According to the 2013 Report of the European Centre for Disease Prevention and Control (ECDC), Serbia belongs to the countries with an intermediate incidence of carbapenem-resistant bacteria [17]. However, such data seem to be unreliable because of underreporting. In addition, the outbreak of nosocomial infections caused by multi-resistant Acinetobacter in Serbia has been reported elsewhere [18]. Infections caused by Acinetobacter spp. represent 10% of all nosocomial infections in the KBC “Kragujevac,” another tertiary-care center in Serbia [18]. Such data fit into the range found in the present study. Similar data from the U.S., European Union, and South America differ significantly; the prevalence of Acinetobacter infections in hospitals was found to be 3%, 14%, and 39%, respectively. In addition, the incidence of those infections has increased since the mid-2000s [9,19]. The incidence and prevalence of nosocomial infections differ in various countries, depending on many factors but primarily on the development of health services and the procedures adopted to control these infections [20].
Respiratory tract specimens predominate among the biologic samples presented in Table 1. Similar results have been reported by other authors [8]. The distribution of specimens containing Acinetobacter probably is related to hospital epidemiology and infection control procedures. Recently adopted national regulations [12], as well as the hospital infection control policy, might reduce the intra-hospital spread of multi-resistant A. baumannii and dissemination of these strains outside the hospital.
As is well known, the virulence of other bacteria can be increased in mixed infections involving A. baumannii. Coagulase-negative staphylococci deserve particular attention. These organisms are normal inhabitants of the human skin and mucous membranes but recently have attracted attention as major nosocomial pathogens, especially in critically ill patients [21]. The impact of co-infection with A. baumannii and coagulase-negative staphylococci on the mortality rate in different groups of in-patients, their length of stay, and healthcare costs remains to be clarified.
As regards the antibiotic armamentarium shown in Table 2, it should be emphasized that 80% of patients were treated with cephalosporins, and 61% of patients were treated with carbapenems in an empiric manner. Almost one fifth of those patients were treated empirically with antibiotics from the Critically Important Antibiotic List [22] such as colistin and linezolid. In addition, the majority of the antibiotics used empirically were ineffective against Acinetobacter because of the high prevalence of resistant strains. The local patterns of resistance of A. baumannii shown in Fig. 1 fits into the range reported in recent papers [9]. However, resistance to carbapenems in the present study was 97%–100% (Fig. 2), which significantly outscored the results in other studies. For example, Acinetobacter resistance to carbapenems was most pronounced in Greece (90%), followed by Croatia (89%), Romania (85%), and Italy (79%) in the 2013 Report of the ECDC [17].
There are many factors that could contribute to such a high prevalence of Acinetobacter resistance. Previous use of antibiotics, length of hospital stay, and patient age are the main risk factors for the emergence of multi-resistant Acinetobacter infections according to the data obtained in this study. A more detailed overview of the risk factors for colonization and infection by Acinetobacter was provided by Mioiljevic et al. [23]. Baran et al. [24] have shown that prolonged use of carbapenems also favors the occurrence of nosocomial infections caused by imipenem-resistant strains of Acinetobacter spp. [2,9,21].
Viehman et al. have suggested the empiric use of colistin-based combinations for multi-resistant and carbapenem-resistant strains of A. baumannii; i.e., prior to the determination of antibiotic susceptibility [25]. Such an approach is controversial because of the increasing resistance of A. baumannii to colistin and the multiple mechanisms that could be involved in the development of resistance. In addition, there is a need for further education of medical practitioners on the use of colistin in the treatment of nosocomial infections. The physician adherence to the current guidelines should be improved, especially regarding the colistin-based combinations that may be inappropriate (for example, colistin + carbapenem in patients with pneumonia caused by carbapenem-resistant strains). In addition, there are significant variations in dosage regimens recommended in U.S. and European sources [26,27].
Another argument against the empiric treatment of nosocomial A. baumannii infections could be the high mortality rate of inadequately treated patients. As shown in Table 3, there was a striking difference in the mortality rate of patients who received empiric vs. targeted treatment. Obviously, if A. baumannii infection remains unrecognized and the patient continues on empiric treatment, the mortality rate increases significantly. It should be emphasized that the mortality rate of patients over age 80 with A. baumannii infection was 100% (Fig. 3). Further analysis of this population is needed because of the small sample in the current study. However, a diagnosis of A. baumannii infection usually is omitted in hospital settings, and physicians should be warned about that problem. The elderly treated in the Medical Center “Bežanijska kosa” often originated from long-term care facilities, where the A. baumannii colonization rate is high [28].
Current guidelines for the treatment of nosocomial multi-resistant A. baumannii infections were published recently [29]. However, low physician adherence to clinical practice guidelines may adversely affect the outcome [30]. In other words, physicians usually describe themselves as “light” users of guidelines [31]. Possible obstacles to successful treatment of multi-resistant A. baumannii infections in clinical settings could be the following: (1) inadequate use of antibiotics/polypharmacy, especially in the ICU; (2) lack of knowledge of the significance of A. baumannii infections in hospitalized patients; (3) inadequate knowledge of the extrapolation of in vitro susceptibility data to the antibiotic choice in clinical settings (for example, use of carbapenems in combination with colistin for multi-resistant A. baumannii infections); and (4) lack of reliable knowledge of antibiotic safety.
Pharmacokinetic/pharmacodynamic (PK/PD) analysis is of particular importance in rational pharmacotherapy of nosocomial A. baumannii infections, especially in relation to posology and dosage regimens. In brief, colistin PK is a complex puzzle of different accuracies and reliabilities [32]. Accordingly, there are different dosage recommendations in various countries, for example, in the European Union and the U.S. Of note, the peak plasma concentration (Cmax) of colistin was predicted to be 0.60 mg/L after the first dose of 3 million international units (IU) of colistimethate sodium (CMS) and 2.3 mg/L after repeated administration of 3 million IU t.i.d in ICU patients [33,34]. Accordingly, if CMS is administered without a loading dose, the plasma concentration will remain below the minimum inhibitory concentration (MIC)(2 mg/L) after the first few doses, leading to a significant therapeutic delay and treatment failure. (The MIC of colistin ranges from 0.25–2 mg/L for most clinical isolates of A. baumannii [25].) It should be emphasized that colistin exerts a concentration-dependent antimicrobial action that correlates with the ratio of the area under the curve (AUC) and MIC. The mean post-antibiotic effects of 1× MIC and 4× MIC colistin were 3.90 and 4.48 h in a study of 19 multi-resistant isolates of A. baumannii, but other authors indicate that long intervals of colistin dosing might be inadequate for A. baumannii, suggesting an advantage of an 8-h regimen rather than 12- or 24-h schedules.
Tigecycline is bacteriostatic against A. baumannii, with an in vitro post-administration therapeutic effect of 0.7–3 h [35]. In the PK/PD of tigecycline in patients with A. baumannii infections, the cornerstones are: (1) A large volume of distribution and extensive tissue distribution; (2) a low serum Cmax (0.7–0.8 mg/L) after the standard loading dose of 100 mg; (3) insufficient urinary excretion of unchanged drug; and (4) poor lung penetration and lower free AUC/MIC ratios [25]. Accordingly, suboptimal clinical outcomes should be expected in patients with carbapenem-resistant A. baumannii infections of the blood stream or urinary tract or pneumonia treated with standard doses of tigecyline (loading dose of 100 mg followed by 50 mg b.i.d.). Greater maintenance doses (75–100 mg b.i.d.) might be more effective in these cases [25].
In conclusion, this study confirms that infections with A. baumannii occur frequently in tertiary healthcare centers in our country. Evolution of multi-resistant and carbapenem-resistant nosocomial A. baumannii is alarmingly fast, with nearly 100% multi-resistant strains at present. One of the factors that could contribute to such resistance is inadequate antibiotic therapy, especially in elderly patients with numerous co-morbidities and medications. The cost of long-term use of antibiotics in the treatment of infections caused by multi-resistant A. baumannii has become a heavy burden for the healthcare system. It is necessary to conduct rigorous epidemiologic measures to control these infections and apply modern therapeutic guidelines for the anti-microbial treatment of nosocomial infections, adjusted to local resistance patterns.
Footnotes
Acknowledgments and Author Disclosure Statement
This study was supported by Scientific Research Grants from the Ministry of Science of Montenegro (No. 01-1370) and the Ministry of Education and Science of Serbia (No. OI 175046).
The authors declare that they have no conflicts of interest.