
Abstract
Abstract
Objective:
To evaluate the efficacy of prophylactic antibiotics in reduction of infections after shock wave lithotripsy (SWL) in patients undergoing shock wave lithotripsy (SWL).
Methods:
The study was a randomized control trial. Between 2012 and 2014, patients with pre-operative sterile urine undergoing SWL were randomly assigned by the randomization ratio of 1:1 to receive prophylactic antibiotics with single-dose oral levofloxacin (500 mg) or no treatment (control group), respectively. Urinalysis and urine cultures were obtained between post-operative day five and seven, respectively. Pyuria was defined as ≥10 white blood cells per high power field (WBC/hpf). Significant bacteriuria was defined as ≥105 colony forming units per milliliter (CFU/mL) uropathogens. Febrile urinary tract infection (fUTI) was defined as body temperature higher than 38.0°C with pyuria or significant bacteriuria within seven days after SWL treatment.
Results:
Initially, 274 patents underwent randomization with 135 and 139 patients in the levofloxacin and control group, respectively. A total of 206 patients (106 with placebo and 100 with levofloxacin) with complete follow-up of urinalysis were eligible for analysis. The rates of post-operative pyuria were not significantly different in patients with and without prophylaxis (8% versus 4.7%, p = 0.33). Moreover, there was also no significant difference in rates of bacteriuria in patients with and without prophylaxis (1% versus 0%, p = 0.49). Patients without follow-up urinalysis and urine culture received telephone survey. Among them, there was only one patient reporting post-SWL fever in the levofloxacin group (0.7%) compared with none (0%) in the control group (p = 0.49). As the results of the interim analysis revealed no benefit of levofloxacin in preventing post-SWL pyuria, bacteriuria, and fUTI, we terminated the study early before the pre-planned sample size was achieved.
Conclusions:
The incidence of asymptomatic and fUTI is low in patients with pre-SWL sterile urine undergoing SWL. Therefore, prophylactic antibiotics may be unnecessary in this cohort of patients.
S
Patients and Methods
Study design
All procedures were performed in compliance with the guidelines for Good Clinical Practice and the Declaration of Helsinki. The study was approved by the Institutional Review Board of our hospital. All patients provided written informed consent before enrollment. The design was a randomized control study.
Participants
From January 2013 to December 2014, patients diagnosed with renal or ureteral stones without UTI and scheduled to receive SWL in our institution were invited to participate in the study. The patients ranged in age from 18 to 65 years. Exclusion criteria included: (1) pyruria (≥10 white blood cells per high power field [WBC/hpf] per milliliter), positive leukocyte esterase, positive nitrite or bacteria on pre-operative urinalysis; (2) patients with known allergy to quinolone; (3) patients who received antibiotics for treatment of a UTI or other infections over the 4-wk period prior to the procedure; (4) immunocompromised patients, such as those with liver cirrhosis or taking corticosteroid; (5) recent ureteroscopic surgery with/without ureteral JJ stent; and (6) patients with Foley urethral catheterization, ureteral catheterization, or nephrostomy tube. Patient characteristics including age, gender, height, body weight, stone size on plain abdominal radiograph, as well as location and laterality of the stone were recorded. The pre-operative evaluation entailed taking a thorough history, physical examinations, blood chemistry tests and C-reactive protein (CRP), renal ultrasound, plain abdominal radiograph, urinalysis, and urine culture. To allocate the participants, a computer-generated list of random numbers was used by a study nurse. The patients were randomly assigned by the randomization ratio of 1:1 to receive either a single dose of oral levofloxacin (500 mg) 1–2 h pre-operatively or no prophylactic antibiotics (levofloxacin versus control group).
Intervention
All SWL procedures in this study were performed on an outpatient basis. Sterile technique was practiced and maintained in all cases. All procedures were performed with the Dornier Lithotripter S II (Dornier MedTech, Munich, Germany). Physiologic parameters including blood pressure, pulse, electrical activity of the heart, and oxygen saturation were all monitored continuously during the procedure. All patients received intravenous general anesthesia with dormicum and fentanyl. The stones were monitored with real-time fluoroscopy. The patients with renal stones underwent 3,000 shocks with a pulse repetition frequency (PRF) of 80 per minute; the shock wave energy level was increased to a maximum of 4. Patients with ureteral stones received 3,000 shocks with a PRF of 80 per minute; the shock wave energy level was increased to a maximum of 5.
Outcomes and follow-up
After SWL treatment, patients would be followed up with serum CRP on post-SWL day two and four and urinalysis and urine culture on post-SWL day five to seven. Significant bacteriuria was defined as grow of ≥105 colony forming units per milliliter (CFU/mL) uropathogens. Post-operative febrile urinary tract infection (fUTI) was defined as body temperature of ≥38.0°C with pyuria or significant bacteriuria over a period of 7 d after the procedure.
Sample size calculations
The aim of the study was to evaluate the efficacy of prophylactic antibiotics in reduction of post-SWL bacteriuria. The study sample size was calculated in accordance with the 1:1 allocation rule. Alpha value of 0.05 and a beta value of 0.2 were assumed to have a UTI rate of 2.1% and 5.7% in the levofloxacin and control group, respectively [4]. The minimum of sample sizes to detect statistically significant differences were 507 patients in each group of patients.
Statistical methods
We used MedCalc version 12.3.0.0 (MedCalc Software, Ostend, Belgium) to analyze the data. Comparisons of parameters between patients with and without prophylaxis were performed using the independent t test (continuous data), χ2 test, or Fisher exact test (categorical) and Mann-Whitney U test (ordinal data). A p value of <0.05 was regarded as statistically significant.
Results
During the study period, there were 1,380 patients undergoing SWL at our institution. After excluding those with UTIs, recent antibiotic use, older than 65 or younger than 18 years, immunocompromised, and administrative reasons, 292 patients were invited to participate in our study; 18 patients declined to participate. A total of 274 patients were enrolled and randomly assigned to one of two groups. Five patients were lost to follow-up in each group. Thirty patients in the levofloxacin group and 28 patients in the control groups did not receive post-operative urinalysis and urine culture on post-SWL day five to seven. They received telephone survey 2 wks after SWL treatment. A total of 206 patients were eligible for analysis (Fig. 1).

Flow diagram of patients undergoing shock wave lithotripsy (SWL) progress through the phases of randomization.
Table 1 summarizes the baseline characteristics and outcomes of procedure in the two groups. Age, gender, body mass index, location and size of stones were comparable between the two groups of patients. No significant difference was observed in the peri-operative parameters, including procedure time.
The rates of post-SWL pyuria were not different in patients with and without antibiotic prophylaxis (8% versus 4.7%, p = 0.33). There was also no difference in rates of bacteriuria in patients with and without prophylaxis (1% versus 0%, p = 0.49). Patients without follow-up urinalysis and urine culture received telephone survey. Among them, there was only one patient reporting post-SWL fever in the levofloxacin group (0.7%), compared with none (0%) in the control group (p = 0.49). Urine culture with mixed growth was regarded as being contaminated and was omitted while analyzing data in regard to the number of significant bacteriuria. The results of urine culture are detailed in Table 2. It is noteworthy that there was no significant difference in serum CRP level between the two groups (Fig. 2; p = 0.59).
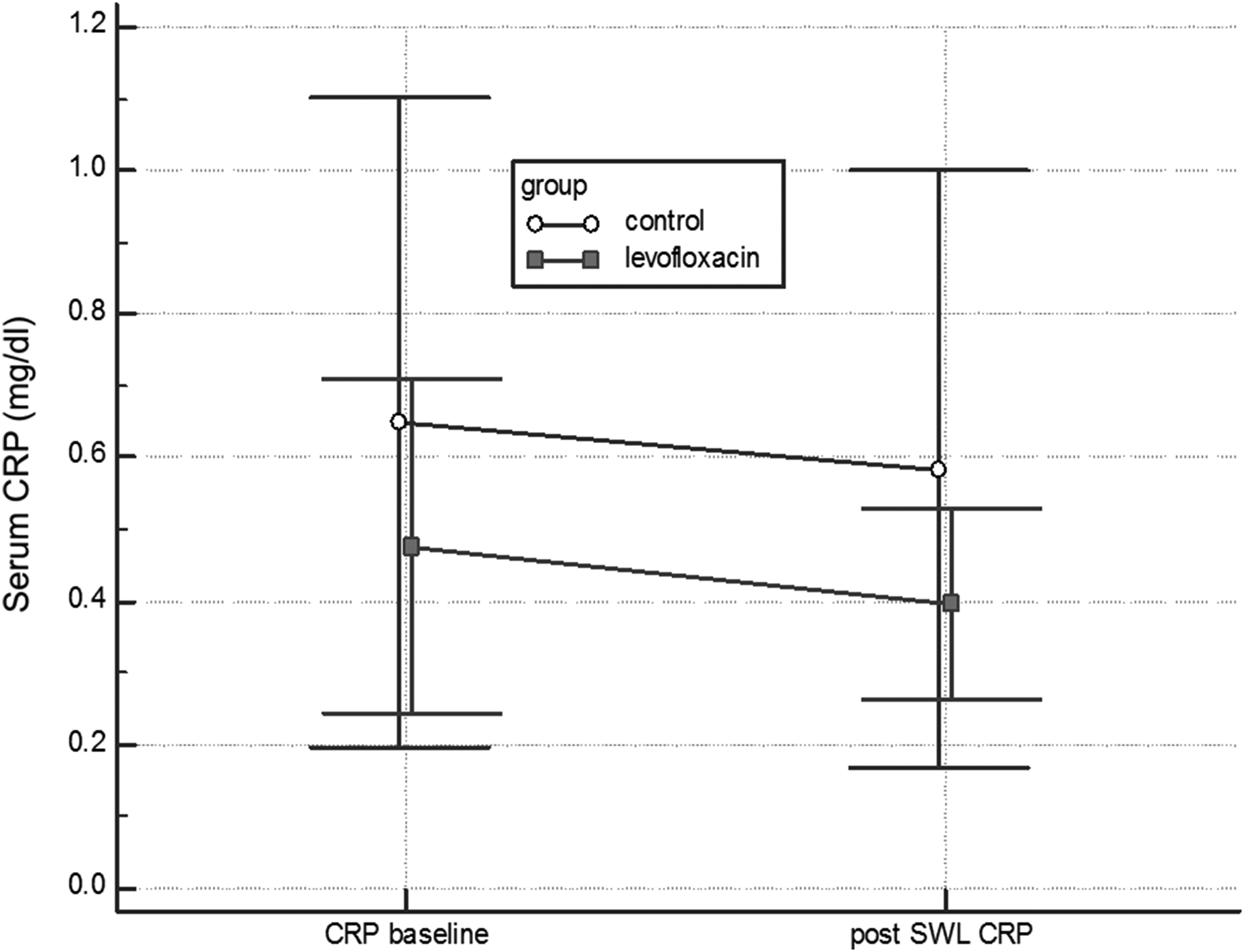
Comparison of change in serum C-reactive protein (CRP) in patients with and without antibiotics prophylaxis.
Growth ≥105 colonies per milliliter.
Discussion
All surgeries and procedures have variable risks of post-surgical infection and the major purpose of prophylactic antibiotics is to reduce post-surgical infection. Antibiotic prophylaxis involves a brief course of antibiotics administered before or at the start of a diagnostic and/or therapeutic intervention and could reduce post-surgical infections. The dose and duration were given based on the probability of post-surgical infections.
Shock wave lithotripsy is a common procedure that is utilized for the treatment of renal and ureteral stones with good efficacy and low complication rates [1]. The general consensus is that patients with pre-SWL bacteriuria or UTI should receive treatment with antibiotics, whereas whether patients with pre-SWL sterile urine should have prophylactic antibiotics has been controversial. The AUA best practice published in 2008 suggested that all patients—even those patients with sterile urine—should receive prophylactic antibiotics [6]. The EAU guidelines recommended prophylactic antibiotics only in select patients at risk of infection [5]. A meta-analysis performed in 2012 revealed that prophylactic antibiotics offered little benefit for preventing UTIs and reducing incidence of bacteriuria in patients with pre-SWL sterile urine [2]. However, some protective effect of prophylactic antibiotics was observed on preventing post-SWL bacteriuria (RR 0.67, 95 CI 0.44–1.02) and UTI (RR 0.54, 95 CI 0.29–1.01), although not statistically significant. Additionally, two studies reported that post-SWL infectious complication rate is low in select patients, which is commensurate with recommendations on EAU guidelines [5].
The associated risk factors in post-SWL infection included advanced age, urinary tracts anomaly, recurrent UTI history, immunocompromised status, external catheter, internal stent, coexisting infection, bacteriuria, and infectious stones. Our current randomized controlled trial, excluding patients with the above-mentioned risks, revealed that prophylaxis with oral levofloxacin did not offer benefit in reducing post-SWL infectious complications in these patients, as shown by the result that antibiotic prophylaxis did not result in a lower rate of pyuria, bacteriuria, and fever. In sample size calculation, the estimated bacteriuria rates were 5.7% in the control group and 2.1% in the levofloxacin group [4]. However, the actual bacteruira rates among these patients were low in patients with and without prophylaxis. The interim analysis disclosed that the rates of pyuria (8% versus 4.7%, p = 0.33), bacteriuria (1% versus 0%, p = 0.49), and fever (0.7% versus 0%, p = 0.49) were not lower in the levofloxacin group and even slightly higher compared with the control group. The serum CRP did not differ significantly between two groups of patients (p = 0.59).
Because the incidence of post-SWL infectious complications is low and use of prophylactic antibiotic did not reduce the rate of post-SWL infectious complications, we terminated the study early. We recommend that SWL can be performed safely without antibiotic prophylaxis in patients with pre-SWL sterile urine, with possible benefit of less bacterial resistance and side effects associated with the antibiotics. [9]
Fluoroquinolones had high oral absorption rate, high renal excretion, and relatively longer half-life than other antibiotics, which made oral fluoroquinolone a good choice for prophylactic antibiotics in the urologic field [10]. For patients who underwent trans-rectal ultrasound-guided biopsy [11] and ureteroscopic lithotripsy [12], single dose of oral levofloxacin could reduce procedure-related infections. As such, the current study used levofloxacin as prophylactic antibiotics. However, the current study did not show the benefit of levofloxacin as prophylaxis in low-risk patients. There are high proportions of antibiotic resistance in bacteria that cause common infections (e.g., UTIs, pneumonia, blood stream infections) in all parts of the world. A high percentage of hospital-acquired infections are caused by highly resistant bacteria. Because SWL is used widely as a first-line treatment for urolithiasis and there were trends of emerging levofloxacin-resistant Escherichia coli, current results justify the unnecessary use of antibiotic prophylaxis with levofloxacin to prevent further increases in bacteria resistance [9].
No general agreement regarding which factor is associated with higher risk of post-SWL infection exists. The EAU guidelines [5] suggest that there is a risk of developing post-SWL infections in patients with a ureteral internal stent placement, in-dwelling catheter, nephrostomy tube, and infectious stones. However, the AUA proposed different risk factors that included advanced age, urinary tract anomalies, poor nutritional status, smoking, long-term corticosteroid use, immunodeficiency, external catheter, colonized endogenous/exogenous material, coexistent infections, and prolonged hospitalization [7]. Therefore, we excluded these patients from evaluation. It is better to calculate the score of each risk factor based on the probability of post-SWL infections. Fujita et al. [13] proposed a scoring system to stratify patients into different risk group but the study only enrolled limited risk factors for evaluation. Also, patients with pre-SWL bacteriuria may be regarded as having UTIs and should receive antibiotic treatment and not prophylaxis. Another commonly encountered risk factor is ureteral stenting. Whether ureteral stenting is associated with more infectious complications remains unanswered and warrants further studies [7,14]. Although some studies questioned the increased risk in patients with JJ stenting, the AUA and the EAU still listed ureteral stenting as a risk factor [5,8].
There were several limitations of the study. First, despite the fact that the study is a randomized controlled trial, the study was conducted in a single center. To generalize the results globally, multicenter randomized trials through the auspices of different urologic organizations is warranted. Second, we did not check the stone analysis routinely and therefore the exact effects of the stone components on the post-SWL infection rates remains unclear. Third, our results did not enroll the pre-planned sample size. The interim analysis revealed persistently low rates of post-SWL bacteriuria in both groups of patients. Despite these limitations, the study provide good evidence to support the current suggestion by the EAU guidelines that antibiotics are unnecessary in low-risk patients undergoing SWL.
Conclusions
The current study revealed that the incidence of asymptomatic and febrile urinary tract infection is low in low-risk patients undergoing SWL. Therefore, we suggest that prophylactic antibiotics in these patients is unnecessary with no benefit in reducing infectious complications and may pose the risk of increased bacterial resistance and side effects of antibiotics.
Footnotes
Acknowledgment
The study is sponsored by Taipei Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation TCRD-TPE-101-C1-2 IRB: 00-IRB-022-XD.
Author Disclosure Statement
No competing financial interests exist.