
Abstract
Abstract
Background:
Post-operative pneumonia is a frequent and possibly fatal complication of esophagectomy and is likely caused by aspiration of oropharyngeal fluid that contains pathogenic micro-organisms. We conducted a multi-center retrospective study to investigate the preventive effect of oral health care on post-operative pneumonia among patients with esophageal cancer who underwent esophagectomy.
Methods:
A total of 280 patients underwent esophagectomy at three university hospitals. These patients were divided retrospectively into those who received pre-operative oral care from dentists and dental hygienists (oral care group; n = 173) and those who did not receive such care (control group; n = 107). We evaluated the correlations between the occurrence of post-operative pneumonia and 18 predictive variables (patient factors, tumor factors, treatment factors, and pre-operative oral care) using the χ2 test and logistic regression analysis. The differences of mean hospital days and mortality rate in both groups were analyzed by the Student t-test.
Results:
Age, post-operative dysphagia, and absence of pre-operative oral care were correlated significantly with post-operative pneumonia in the univariable analysis. Multivariable analysis revealed that diabetes mellitus, post-operative dysphagia, and the absence of pre-operative oral care were independent risk factors for post-operative pneumonia. The mean hospital stay and mortality rate did not differ between the oral care and control groups.
Conclusion:
Pre-operative oral care may be an effective and easy method to prevent post-operative pneumonia in patients who are undergoing esophagectomy.
D
Post-operative pneumonia reportedly occurs in 7.4%–50% of patients who undergo esophageal resection for cancer, and age, poorer pulmonary function, smoking, diabetes mellitus, and greater surgical stress are related to its frequency [3–17]. However, few studies have evaluated the correlation between oral hygiene and the frequency of post-operative pneumonia. This multi-center retrospective cohort study investigated the preventive effect of oral care on post-operative pneumonia among patients who underwent esophagectomy.
Patients and Methods
Patients
A total of 280 patients with esophageal cancer underwent esophagectomy between 2010 and 2014 at three university hospitals (Kagoshima University Hospital, Nagasaki University Hospital, and Kobe University Hospital) and were included in this study. The study's design was approved by the Ethics Review Boards of all participating hospitals. We excluded patients who underwent endoscopic mucosal resection or submucosal dissection. The selected patients were divided into two groups: (1) an oral care group that consisted of 173 patients, and (2) a control group that consisted of 107 patients. In Japan, the Medical Insurance System established coverage for peri-operative oral care in 2012. Patients in the control group underwent surgery before the start of peri-operative oral care in each hospital, and patients in the oral care group underwent surgery after that time. Most patients were admitted to the hospital a few days before surgery, and there were no differences in pre-operative hospital days between the two groups.
Oral care
Each patient in the oral care group received care from a dentist and dental hygienist. This care was provided between the time the hospitalization was determined and the day before surgery and consisted of oral health instruction, removal of dental calculus (scaling), professional mechanical tooth cleaning, removal of tongue coating with a toothbrush, and extraction of teeth with severe periodontitis. After surgery, both groups were asked to perform frequent (every 3–6 h) gargling with water during the daytime.
Variables
The objective variable was the occurrence of post-operative pneumonia. Pneumonia was diagnosed by the presence of fever, elevated white blood cell count, and pulmonary infiltrates requiring antibiotic therapy according to the criteria reported by several investigators [3,5,12]. Based on the literature [3–17], we defined the predictor variables as: (1) patient factors: Age, gender, body mass index, smoking habits, drinking habits, diabetes mellitus, hypertension, pre-operative serum creatinine concentration, pre-operative serum albumin concentration, and forced expiratory volume (FEV) 1%; (2) tumor factors: Site and stage; (3) treatment factors: Thoracotomy, operation time, blood loss, neoadjuvant chemotherapy, and post-operative dysphagia; and (4) oral care intervention. Patients who had not smoked for >1 year were classified as not having a smoking habit. The tumor sites were divided into the upper, middle, and lower esophagus. Tumor stage was classified according to the Japan Esophageal Society's criteria [18]. Post-operative dysphagia was defined by the medical record as choking when the patient started a paste diet after surgery, aspiration during swallowing (via videofluoroscopic examination), or continued tube feeding at the time of discharge.
Statistical analysis
Statistical analyses were performed using SPSS software (version 22.0; Japan IBM Co., Tokyo, Japan). Univariable analysis was performed using the χ2 test. Multivariable analysis using logistic regression was performed to evaluate the associations between the predictor variables and the occurrence of post-operative pneumonia. Further, the differences in mean hospital days and mortality rate in the oral care and control groups were analyzed by the Student t-test. All predictor variables were included in the multivariable analysis. In all analyses, a two-tailed p value of <0.05 was considered statistically significant.
Results
Post-operative pneumonia occurred in 65 (23.2%) of the 280 patients, and four patients died from complications during their hospitalization. The rate of occurrence of pneumonia did not differ among the three hospitals, being 6/29 (20.7%), 33/145 (22.6%), and 26/106 (24.5%), respectively, in the hospitals listed above. There were no differences in background factors between the groups except that the operation time of the oral care group was longer than that of the control group (Table 1).
FEV = forced expiratory volume.
The frequency of pneumonia was significantly lower in the oral care group (33/173: 19.1%) than in the control group (32/107: 29.9%) (p = 0.037). The average length of hospital stay and mortality rate did not differ between the groups. In the univariable analyses, age, post-operative dysphagia, and absence of pre-operative oral care were significantly associated with pneumonia. Multivariable analysis revealed that diabetes mellitus, post-operative dysphagia, and absence of oral care were independent risk factors for post-operative pneumonia (Table 2). Some other factor, such as poorer pulmonary function, greater blood loss, or neoadjuvant chemotherapy, tended to correlate with the frequency of pneumonia, although there were no statistical differences (Fig. 1).
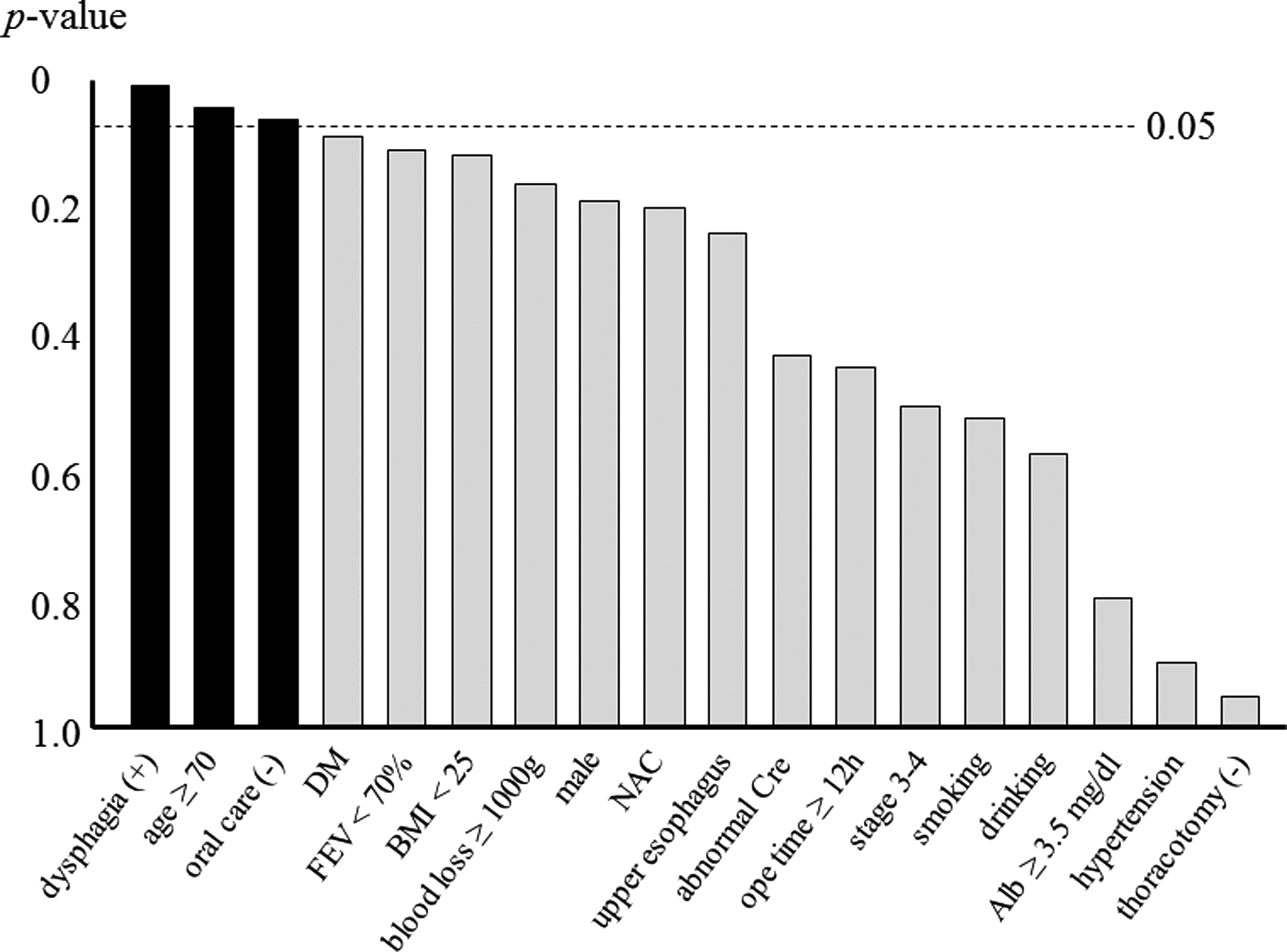
Univariable analysis shows that age, post-operative dysphagia, and absence of pre-operative oral care are significantly associated with pneumonia. Some other predictor variables tend to correlate with the frequency of pneumonia, but the p value is >0.05.
CI = confidence interval; FEV = forced expiratory volume.
Discussion
Post-operative pneumonia frequently develops after esophagectomy and is associated with prolonged hospital stays, greater medical costs, and a substantial operative mortality rate. Authors who investigated the risk factors for post-operative pneumonia after esophagus surgery reported that the incidence rate was 7.4%–50%, and that various factors such as regular smoking, decreased pulmonary function, diabetes mellitus, age, greater surgical stress (operation time, blood loss, and thoracotomy), and general condition (performance status and complications) was correlated with the complication (Table 3) [3–17]. In the present study, we observed that the frequency of post-operative pneumonia was 23.2%. The relatively high incidence of post-operative pneumonia, despite the recent advances in surgical procedures and antibiotic therapy, indicate that new preventive measures may be needed. Bágyi et al. [1] reported that aspiration of oral fluid containing micro-organisms played role in pneumonia after brain surgery. Also, one of the main causes of ventilator-associated pneumonia (VAP) is believed to be aspiration of oropharyngeal fluid containing pathogenic organisms, such as Staphylococcus aureus, Streptococcus pneumoniae, or gram negative bacilli [19–22]. However, few reports have evaluated the influence of oral hygiene or dysphagia on post-operative pneumonia in patients with esophageal cancer. Akutsu et al. reported that instruction by a surgeon to encourage brushing the teeth five times per day decreased the frequency of post-operative pneumonia among patients who underwent esophagectomy with right-sided thoracotomy [23]. Hiramatsu et al. found that a pre-operative care bundle of deep breathing, breathing exercise, respiratory muscle stretching, professional oral cleaning and teeth and tongue brushing, eating proper food, and quitting smoking prevented post-operative pneumonia among patients who underwent esophageal resection [24]. However, those studies were single-center historically controlled studies that evaluated a small number of patients, and no other risk factors for post-operative pneumonia were analyzed. We performed a multi-center retrospective cohort study with a considerable number of patients. To the best of our knowledge, this is the first large-scale clinical study regarding the preventive effects of oral care on post-operative pneumonia among patients undergoing esophagectomy.
S = significant.
Our univariable analysis revealed that age, post-operative dysphagia, and absence of oral care were associated with the rate of post-operative pneumonia. Among these factors, oral care and post-operative dysphagia were most strongly correlated with the occurrence of pneumonia. Furthermore, our multivariable analysis revealed that the absence of pre-operative oral care and the presence of post-operative dysphagia and diabetes mellitus were independent risk factors for post-operative pneumonia. Some other factors, such as poorer pulmonary function, blood loss, or neoadjuvant chemotherapy may be correlated with the incidence of post-operative pneumonia, although these factors were not statistically significant in this study. The length of the hospital stay did not differ between the oral care and control groups. This result probably was attributable to the fact that the duration of hospitalization was affected by other factors, such as adjuvant radiotherapy or chemotherapy.
Previous studies have reported that pneumonia after esophagectomy was associated with various factors, including age [3–5,7,12,16], smoking [3,7,10–14], poorer pulmonary function [3–5,7,8,10–15], diabetes mellitus [3,10,13], greater surgical stress [3,9,12,15,17], and general complications [5,10–12]. However, those factors cannot be improved by the surgeon during the peri-operative period. In contrast, oral care can be administered easily to patients with esophageal cancer during the peri-operative period. The present study is the first to reveal the preventive effects of oral care on post-operative pneumonia after esophageal resection. However, the evidence level is not high because of the non-randomized design. However, it would be difficult to conduct a randomized controlled trial regarding the preventive effect of oral care, because such care has been covered by the Japanese medical insurance system since 2012, and most Japanese patients now receive oral care before surgery. Therefore, we are planning a more extensive retrospective cohort study based on the results of the present study.
Footnotes
Author Disclosure Statement
No competing financial interests exist.