
Abstract
Abstract
Background:
There have been several recent studies on the correlation between intra-operative hypothermia and the occurrence of surgical site infection (SSI). Differences in the depth and timing of hypothermia and the surgical procedure may have led to conflicting results.
Methods:
Patients undergoing gastroenterologic surgery with a duration of >3 h were analyzed. Hypothermia was defined as a core temperature <36°C and was classified as mild (35.5–35.9°C), moderate (35.0–35.4°C), or severe (<35.0°C). Hypothermia also was classified as early-nadir (<36°C within two h of anesthesia induction) and late-nadir (after that time). Risk factors for SSIs were analyzed according to these classifications.
Results:
Among 1,409 patients, 528 (37.5%) had hypothermia, which was classified as mild in 358, moderate in 137, and severe in 33. Early-nadir and late-nadir hypothermia was found in 23.7% and 13.8%, respectively. There was no significant difference in the incidence of SSIs between patients with and without hypothermia (relative risk 1.00; 95% confidence interval [CI] 0.80–1.25; p = 0.997). However, there was a significantly greater incidence of SSIs in patients with severe hypothermia (33.3%) than in those with normothermia (19.2%; p = 0.045) or mild hypothermia (17.0%; p = 0.021). The incidence of SSIs also was significantly greater in patients with late-nadir than in those with early-nadir hypothermia (23.7% vs. 16.5%; p = 0.041). The incidence of organ/space SSIs was significantly greater in patients with late-nadir hypothermia (19.6%) than in patients with normothermia (12.7%; p = 0.012). In multivariable analysis, neither severe hypothermia (odds ratio 1.24; 95% CI 0.56–2.77] nor late-nadir hypothermia (OR 0.71; 95% CI 0.46–1.01) was an independent risk factor for SSIs.
Conclusions:
Severe and late-nadir hypothermia were associated with a greater incidence of SSIs and organ/space SSIs. However, neither of these patterns was identified as an independent risk factor for SSIs, possibly because of the small number of patients.
I
To prevent excessive heat loss, various intra-operative warming methods are employed, and the nadir temperature usually is observed within two h of the induction of anesthesia [8]. Some researchers have focused on the management of early hypothermia, and warming before induction of anesthesia has been recommended to prevent phase 1 hypothermia [9–11].
In a randomized clinical trial that confirmed the preventive effect of intra-operative normothermia on SSIs, the mean core temperature at one h after the start of surgery was <36°C even in patients assigned to additional warming, and the mean final intra-operative core temperature was 36.6°C [4]. In addition, the lowest intra-operative temperature (34.7°C) was noted at the end of surgery in patients assigned to poor thermal care. Considering that early hypothermia that reverses during surgery involves simple redistribution of heat, we hypothesized that hypothermia with a late nadir temperature caused by heat loss may have a more substantial impact on SSI.
Seamon et al. [6] conducted a cut-point analysis of the entire range of lowest intra-operative temperatures that best predicted SSIs and found that temperatures <35°C were associated with an increase in SSIs after trauma laparotomy. In the present study, the primary goal was to investigate the impact of hypothermia on the occurrence of SSIs according to its timing and severity during prolonged surgery, while the secondary goal was to identify the factors associated with severe and early- and late-nadir intra-operative hypothermia.
Patients and Methods
This study was approved by the research ethics committees of Hyogo University of Health Sciences and the study institution. Patients who underwent prolonged surgery under general anesthesia (>3 h), including esophageal, gastric, colorectal, hepato-biliary, or pancreatic surgery (except for laparoscopic cholecystectomy) between January 2009 and December 2011 at Hyogo College of Medicine Hospital were included in the study. Patients with a body temperature >38°C prior to surgery were excluded from the analysis. The primary endpoint was the incidence of SSIs, so patients with early hospital death (<5 d) also were excluded. The rectal or esophageal temperature was measured continuously during surgery as a surrogate for core temperature, and the intra-operative nadir was evaluated. Hypothermia was defined as a temperature <36.0°C and was classified as mild (35.5–35.9°C), moderate (35.0–35.4°C), or severe (<35.0°C). Hypothermia also was classified as early or late nadir, depending on the timing of the lowest temperature. Early-nadir hypothermia was defined as detection of the nadir temperature within two h after the induction of anesthesia, and late-nadir hypothermia was defined as detection of the lowest temperature more than two h after induction.
The following variables were examined for association with SSIs and hypothermia: Age >65 y, gender, body mass index (BMI) <18.5 (underweight) or >25 (overweight), American Society of Anesthesiologists (ASA) physical status score >2, co-morbidities, steroid use, smoking (only for SSI), prolonged pre-operative hospital stay (>7 d) (only for SSI), pre-operative anemia (hemoglobin <13.0 g/dL for males and 11.0 g/dL for females) (only for hypothermia), intra-operative fluid administration >75th percentile (only for hypothermia), significant blood loss (>75th percentile for that procedure) (only for hypothermia), hypothermia (only for SSI), contaminated or dirty/infected incision (only for SSI), stoma construction, prolonged surgery (>75th percentile of the duration for each specific operation according to the Japanese healthcare-associated infection surveillance data [12], emergency surgery, laparoscopic surgery, concomitant other surgery, thoraco-laparotomy (only for hypothermia), lithotomy position (only for hypothermia), long incision (exceeding half the length between the xiphoid process and the superior margin of the symphysis pubis) (only for hypothermia), combined epidural and general anesthesia (only for hypothermia), and blood transfusion (only for hypothermia).
Surgical incisions were recorded on SSI surveillance sheets while the patients remained in the hospital until 30 d after surgery, a common practice in Japan. A diagnosis of SSI was made by infection control physicians based on the definitions in the guidelines issued by the National Healthcare Safety Network [13]. Cefazolin or a second-generation cephalosporin was administered intravenously for 24 h in patients undergoing gastric and colorectal surgery or for 48 h in patients undergoing esophageal or hepato-biliary-pancreatic surgery. Patients who underwent colorectal surgery received mechanical bowel preparation, and oral antibiotics were administered to patients with inflammatory bowel disease.
All subjects received standard warming measures to prevent intra-operative hypothermia. A forced-air warming system (Bair Hugger® Model 750, 3M, Minneapolis, MN) was used after the induction of anesthesia. The temperature management blanket was warmed to 38°C and placed over the patient's body and was kept warm during the operation. The temperature management blanket only partly covered patients who were in the lateral and lithotomy positions. For passive warming, the limbs were wrapped from the lower third of the thighs to the feet, and the neck and shoulders were wrapped using pads when patients were in the supine position. The lower half of the body was wrapped in the lateral position, whereas the arms were wrapped when the patient was in the lithotomy position. A HOT LINE® (Smiths Medical, St. Paul, MN) was used to warm fluid and blood products to 37–38°C. Banked blood for transfusion was warmed to 37°C in a water bath for 30 min before use. Fluid for flushing the surgical field also was warmed to 37°C. The temperature of the operating room was set at 26°C. Warming was not done routinely before anesthesia.
The relative risk ratio (RR) and 95% confidence interval (CI) were estimated for each variable by the χ2 test, and potential confounders were examined by cross-tabulation. Variables selected by these univariable analyses (p < 0.2) were subsequently entered in a logistic regression model to estimate the magnitude of the association (odds ratio [OR] and the 95% CI). The Student t-test was employed to assess the difference between mean values when the distribution was approximately normal. If the distribution was skewed, the Mann-Whitney test was performed instead. The SPSS ver. 21.0 for Windows (SPSS, Chicago, IL) was used for all analyses, and significance was set at p < 0.05.
Results
Of the 1,949 patients who underwent relevant abdominal surgery during the study period, 1,409 met the inclusion criteria. The mean age of the subjects was 61.2 ± 15.7 (standard deviation) (range 15–92) y, and 922 patients were men. The surgery was performed for cancer in 1,059 patients. The breakdown was 71 patients undergoing esophageal surgery, 337 having gastric surgery, 611 having colorectal surgery (for inflammatory bowel disease in 289), and 390 having hepato-biliary or pancreatic surgery.
Hypothermia was detected in 528 patients (37.5%) and was classified as mild in 358, moderate in 137, and severe in 33. Underweight (OR 3.87; 95% CI 1.80–8.33; p = 0.001), thoraco-laparotomy (OR 6.65; 95% CI 3.01–14.70; p = 0.001), and <36°C within two h of the induction of anesthesia (OR 7.70; 95% CI 3.36–17.66; p < 0.001) were identified as independent risk factors for severe hypothermia in a multivariable analysis.
There was a significant difference in the incidence of hypothermia measured within two h of anesthesia induction (50.6% [164/324] vs. 7.3% [79/1085]; p < 0.001). In addition, a significantly greater incidence of hypothermia at the end of surgery was found in patients with hypothermia within two h of anesthesia induction compared with patients without such a pattern (18.5% [60/324] vs. 2.2% [24/1085]; p < 0.001]). A further decrease of the temperature after more than two h (late-nadir hypothermia) was observed in 95 of 324 patients who developed hypothermia within two h of the induction of anesthesia.
Early-nadir hypothermia occurred in 334 patients (23.7%) and late-nadir hypothermia in 194 (13.8%). The incidence of severe hypothermia was significantly greater in patients with late-nadir hypothermia (22/194 [11.3%] vs. 11/334 [3.3%]; p < 0.001). Table 1 shows the variables selected by univariable and multivariable analyses as factors associated with early- and late-nadir hypothermia. In multivariable analysis, age > 65 years, massive hemorrhage, thoraco-laparotomy (preventive), male gender, underweight, and hypothermia within 2 h of anesthesia were identified as factors independently associated with early-nadir hypothermia. Analysis of the factors independently associated with late-nadir hypothermia identified an age >65 years, underweight, diabetes mellitus, pre-operative anemia, combined epidural anesthesia, blood transfusion, concomitant surgery, thoraco-laparotomy, and hypothermia within 2 h of anesthesia, while gastric surgery was associated with a lower risk.
BMI = body mass index (underweight = ≤18.5; overweight = >25); CI = confidence interval; HBP = hepato-biliary-pancreatic; OR = odds ratio; RR = relative risk.
The overall incidence of SSIs was 19.2% (270/1,409), with organ/space and incisional SSIs in 13.1% (n = 184) and 7.1% (n = 100) of the patients, respectively. The SSI rate was 42.3% in esophageal surgery, 9.5% in gastric surgery, 20.2% in colorectal surgery, and 22.1% in hepato-biliary–pancreatic surgery. There was no significant difference in the SSI rate between patients with normothermia and patients with hypothermia (169/881 [19.2%] vs. 101/528 [19.1%]; RR 1.00; 95% CI 0.80–1.25; p = 0.997]). However, a significantly greater incidence of SSIs was demonstrated in patients with severe hypothermia than in those with normothermia or mild hypothermia (severe hypothermia 11/33 [33.3%] vs. normothermia 169/881 [19.2%]; p = 0.045; mild hypothermia 61/358 [17.0%]; p = 0.021) (Fig. 1; Table 2).
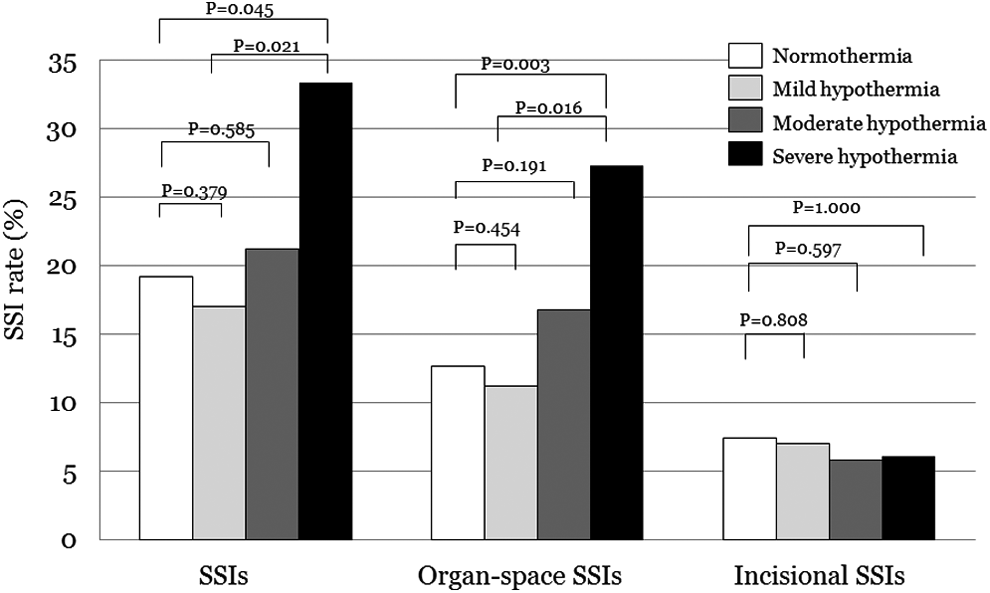
Incidence of surgical site infections (SSIs) in patients with normothermia and mild, moderate, or severe hypothermia.
p = 0.021 vs. mild hypothermia; p = 0.045 vs. normothermia.
p = 0.081 vs. moderate hypothermia; p = 0.012 vs. mild hypothermia; p = 0.024 vs. normothermia.
p = 0.016 vs. mild hypothermia; p = 0.031 vs. normothermia.
p = 0.002 vs. mild hypothermia; p = 0.004 vs. normothermia.
p = 0.153 vs. normothermia.
p = 0.012 vs. normothermia.
There was no significant difference in SSI rate between patients with and without hypothermia within 2 h of the induction of anesthesia [61/324 (18.8%) vs. 209/1085 (19.3%), relative risk 0.98, 95% CI: 0.76–1.26, p = 0.861]. Analysis of the timing of the nadir temperature revealed that the SSI rate was significantly greater in patients with late-nadir hypothermia than in those with early-nadir hypothermia (46/194 [23.7%] vs. 55/334 [16.5%]; p = 0.041]. There was no significant difference in the SSI rate between patients with either early- or late-nadir hypothermia and patients with normothermia. However, the incidence of organ/space SSIs was significantly greater in patients with late-nadir hypothermia (19.6%) than in those with normothermia (12.7%; p = 0.012) or those with early-nadir hypothermia (10.2%; p = 0.002). In addition, the incidence of SSIs and organ/space SSI was significantly greater in patients with severe hypothermia concomitant with late-nadir hypothermia than in those with mild hypothermia or normothermia (SSI 40.9% vs. 17.0% [p = 0.012]; 19.1%; p = 0.024; organ/space SSI 36.4% vs. 11.2% (p = 0.002); 12.7% (p = 0.004)] (Fig. 2, Table 2). However, the incidence of incisional SSIs did not differ among these three groups.
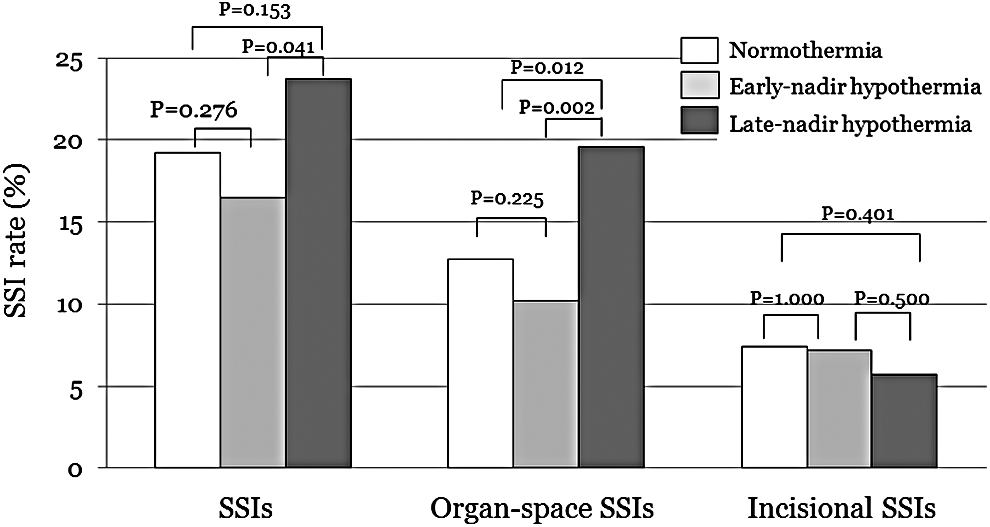
Incidence of surgical site infections (SSIs) in patients with normothermia and early- or late-nadir hypothermia.
Table 3 shows the variables associated with SSIs. According to univariable analysis, there was a significantly greater incidence of SSIs in patients with severe hypothermia (p = 0.036) and severe hypothermia concomitant with late-nadir hypothermia (p = 0.009), and late-nadir hypothermia tended to increase the risk (p = 0.083). Analysis of organ/space SSIs showed a significantly greater incidence of in patients with severe hypothermia, late-nadir hypothermia, and severe hypothermia concomitant with late-nadir hypothermia. However, none of these patterns was found to be an independent factor for SSIs or organ-space SSIs in an exploratory multivariable analysis (Tables 3 and 4).
ASA = American Society of Anesthesiologists; BMI = body mass index (underweight = ≤18.5; overweight = >25); CI = confidence interval; HBP = hepato-biliary-pancreatic; LOS = length of stay; OR = odds ratio; RR = relative risk.
ASA = American Society of Anesthesiologists; BMI = body mass index (underweight = ≤18.5; overweight = >25); CI = confidence interval; HBP = hepato-biliary-pancreatic; LOS = length of stay; OR = odds ratio; RR = relative risk.
Discussion
In the present study, we classified hypothermia according to its severity and the timing of nadir hypothermia. Underweight, thoraco-laparotomy, and <36°C within two h of the induction of anesthesia were independent risk factors for severe hypothermia. In the analysis of risk factors for early- and late-nadir hypothermia, underweight was a risk factor for both types. Redistribution of heat occurs in patients receiving epidural anesthesia, and we found that combined neuraxial and general anesthesia increased the risk of either type of hypothermia. Other risk factors differed between early-nadir and late-nadir hypothermia. Male gender and the lithotomy position were risk factors for early-nadir hypothermia. Billeter et al. [14] reported that male gender was an independent risk factor for hypothermia in patients undergoing elective operations. A relatively long time in the lithotomy position with greater skin exposure before surgery might cause early-nadir hypothermia.
Unlike early-nadir hypothermia, the independent factors for late-nadir hypothermia were related to the surgical procedure (thoraco-laparotomy and concomitant other surgery). It is well established that hypothermia is more pronounced with extensive than with smaller procedures, with most of the difference presumably resulting from evaporative loss [15]. Roe [16] demonstrated that approximately half of the total heat loss is evaporative in rabbits with large abdominal incisions. With regard to host factors, an age >65 years, diabetes mellitus, and pre-operative anemia had an independent influence on late-nadir hypothermia. Mehta et al. [17] demonstrated that patients aged >70 years had a lower core temperature during surgery than did those <70 years old.
Several reports have raised questions about the greater risk of SSIs in patients with intra-operative hypothermia, defined as a temperature <36°C [4,6]. Investigation of the occurrence of SSIs according to the severity of hypothermia identified a significantly greater incidence only in patients with severe hypothermia. However, the small number of patients with severe hypothermia in the present series (33/1409 [2.3%]) might have resulted in the absence of an association between severe hypothermia and SSIs on multivariable analysis. Compared with normothermia and early-nadir hypothermia, there was a significantly greater incidence of organ/space SSI in patients with late-nadir hypothermia. Severe hypothermia was significantly more common among patients with late-nadir than in patients with early-nadir hypothermia. Twenty-two of 33 patients with severe hypothermia were in the late-nadir hypothermia group, and a high incidence of SSIs (40.9%) was observed in patients with severe hypothermia concomitant with late-nadir hypothermia. Thus, late-nadir hypothermia associated with net heat loss had a substantial impact on SSIs.
In contrast, a lower risk for SSI was demonstrated in patients with early-nadir hypothermia (OR 0.74; p = 0.078). Simple redistribution of heat from the core to the subcutaneous tissue in the early phase of surgery does not seem to have a significant impact on SSIs if hypothermia resolves with intraoperative warming. It should be noted that early appearance of hypothermia does not necessarily mean early-nadir hypothermia. In 50.6% of patients who developed hypothermia within 2 h after the induction of anesthesia, it persisted beyond 2 h, and 95 patients who initially developed hypothermia within 2 h were included in the late-nadir hypothermia group. Hypothermia within 2 h of anesthesia induction was an independent risk factor for not only early-nadir hypothermia but also late-nadir hypothermia. In addition, hypothermia within 2 h of anesthesia induction was an independent risk factor associated with severe hypothermia. Although early development of hypothermia itself did not cause greater incidence of SSI, these observation emphasize the importance of pre-warming to prevent early hypothermia.
Compared with the National Healthcare Safety Network data [13], the SSI rate in our series was relatively high, but the incidence (except in esophageal and colorectal surgery) was similar to data from the Japanese healthcare-associated infection surveillance [12]. A reason for the high SSI rate in colorectal surgery is that 289 of 611 patients undergoing such surgery had inflammatory bowel disease. Thoraco-laparotomy is the standard procedure for esophageal cancer in Japan, and 28 of 30 SSIs after this operation were organ/space infections caused by suture insufficiency.
Our study had several limitations. First, we did not warm the patients before anesthesia. This approach may have caused our results to differ from those of current practice. Second, we investigated SSIs only as a possible complication of intra-operative hypothermia. Although early-nadir hypothermia was not associated with a greater risk of SSIs, this does not discourage the performance of warming to optimize the core temperature during the early phase of surgery and prevent complications such as cardiac events [9–11,18].
In conclusion, severe hypothermia and late-nadir hypothermia were associated with a greater incidence of SSIs and organ/space SSIs. However, these types of hypothermia were not identified as independent risk factors for SSIs by multivariable analysis, possibly because few patients developed such hypothermia because we used appropriate intra-operative warming. Early hypothermia caused severe hypothermia and late-nadir hypothermia. This observation validates the importance of warming before induction of anesthesia.
Footnotes
Acknowledgments
We are grateful to the following physicians from the participating surgical wards: Dr. M. Sasako, Dr. N. Tomita, and Dr. J. Fujimoto. We also are indebted to Dr. M. Hirose, Dr. T. Tatara, and Dr. R. Ueki. We thank Dr. H. Matsuda for supporting this study at Hyogo University of Health Sciences.
This work was supported by a grant from 3 M Healthcare Inc. The funder had no role in study design, data collection and analysis, the decision to publish, or preparation of the manuscript.