
Abstract
Abstract
Background:
Colorectal cancer surgery is associated with a high incidence of post-operative infections, the outcome of which may be improved if diagnosed and treated early enough. We compared white blood cell (WBC) count, C-reactive protein (CRP), and procalcitonin (PCT) as predictors of post-operative infections and analyzed their impact on long-term survival.
Methods:
This retrospective study included 186 patients undergoing colorectal surgery. Post-operative values of WBC, CRP, and PCT were analyzed by the receiver operating characteristic (ROC) analysis. We followed infections 30 d after the surgery. A five-year survival was analyzed by Kaplan-Meier method and prognostic factors by Cox regression model.
Results:
Fifty-five patients (29.5%) developed post-operative infection, the most frequent of which was surgical site infection (SSI). C-reactive protein on post-operative day three and PCT on post-operative day two demonstrated the highest diagnostic accuracy for infection (area under the curve [AUC] 0.739 and 0.735). C-reactive protein on post-operative day three was an independent predictor of infection. Five-year survival was higher in the non-infected group (70.8%), compared with the infected group (52.1%). The worst survival (40.9%) was identified in patients with organ/space SSI. Post-operative infection and tumor stage III–IV were independent predictors of a worse five-year survival.
Conclusions:
C-reactive protein on post-operative day three and PCT on post-operative day two may be early predictors of infection after colorectal cancer surgery. Post-operative infections in particular organ/space SSI have a negative impact on long-term survival.
C
Colorectal surgery is associated with a high rate of infectious complications, especially surgical site infections (SSIs). The incidence of SSIs after elective procedures is 5%–30% [4–7] and is higher in rectum surgery than in colon surgery [6,8]. Post-operative infections are well established as predictors of adverse clinical outcome in patients with colorectal cancer and other malignancies [9–13]. They are associated with increased morbidity, length of hospital stay, treatment costs, and mortality [4,14]. Peri-operative mortality after elective colorectal surgery has been reported to be 3%–4% [15,16]. The implementation of the National Surgical Quality Improvement Program (NSQIP) methods in major surgery has proven to have a positive effect shown as a substantial decrease of SSIs, renal complications, and overall 30-day morbidity [17].
Post-operative infective complications are clinically silent initially. Usually they are diagnosed late, on the median post-operative day eight [4,18–22] when many patients already exhibit clinical signs of a serious illness or even sepsis. A common obstacle to early detection of ongoing post-operative infection is inflammation, which is markedly activated by colorectal surgery. It may induce systemic inflammatory response syndrome (SIRS), which may be self-limiting or may progress to sepsis and septic shock. During the early post-operative period non-septic SIRS is difficult to distinguish from sepsis [23,24]. At-risk patients should be identified early because pre-emptive antibiotic treatment may decrease the incidence and severity of post-operative infections and improve outcome [25]. Unnecessary antibiotic therapy is undesirable because it induces the development of bacterial resistance. C-reactive protein (CRP) and procalcitonin (PCT) could be helpful in the early diagnosis of infection after surgery.
C-reactive protein is the first acute-phase protein to be described. It is a non-specific, sensitive systemic marker of inflammation, infection, and tissue damage. The synthesis in hepatocytes is stimulated by cytokines interleukin (IL)-6, IL-1β, and tumor necrosis factor-α (TNF-α). Its half-life is approximately 19 h. The primary role of CRP is to regulate acute inflammation by activating complement system, increasing clearance of apoptotic cells and enhancing the adaptive immune response [26–31]. Several studies have found CRP to be an early predictor of infections after esophageal [32,33], pancreatic [34–36], and colorectal resections [4,18–21,37–42].
Procalcitonin is a precursor for the hormone calcitonin, produced in small amounts in neuroendocrine cells of the thyroid gland, lungs, and gastrointestinal tract [43,44]. In response to inflammation or bacterial/fungal infection it is produced in all tissues throughout the body [45]. Bacterial endotoxins are potent stimuli for the synthesis of PCT. Its half-life is 24–30 h [46]. The biologic role of PCT remains unknown, but experimental studies show it may accelerate inflammation [43]. Procalcitonin concentration may increase after surgery, mostly after intestinal, cardiac, and thoracic operations. Its release may be induced by translocation of endotoxins or bacteria across the gut wall or by bacterial contamination of the operative field [43,46]. Maximum post-operative PCT plasma concentrations were observed mostly on post-operative day one and were higher in patients who developed post-operative infections [47–49].
In recent years only a few studies have compared the diagnostic accuracy of CRP and PCT for early detection of infectious complications in patients undergoing colorectal surgery. Two studies showed PCT was a more reliable marker for the early diagnosis of SSIs [50,51], whereas three others did not show any advantage of PCT over CRP for prediction of post-operative infections [52–54].
The aim of this study was to compare white blood cell (WBC) count, CRP, and PCT as predictive markers of post-operative infections in patients with cancer after colorectal surgery. Understanding the post-operative kinetics of inflammation markers may improve our ability to use them as an early diagnostic tool and treat the infections early and therefore more effectively. We also wanted to establish the influence of post-operative infections on long-term survival.
Patients and Methods
The present study was a retrospective, observational one conducted in the surgery department of Institute of Oncology Ljubljana during a 28-m period, between September 2006 and December 2008. It was approved by the ethical commission of the hospital.
A total of 186 consecutive patients with colorectal cancer and elective colon or rectum resection were included. Fourteen had simultaneous removal of hepatic metastases. Some patients were treated with pre-operative (neo-adjuvant) chemotherapy and/or radiotherapy. The carcinoembryonic antigen (CEA) blood concentration was measured before the start of treatment. The patients’ medical records were reviewed retrospectively with regard to the detail analysis of post-operative infectious complications.
Before the surgery each patient was assessed according to American Society of Anesthesiologists (ASA) physical status classification, which predicts morbidity and mortality accurately [55,56]. All patients were given anti-thrombotic and antibiotic prophylaxis. A standardized anesthesiologic protocol was used including general and epidural anesthesia. During the operation type of operation, the length of the procedure, blood loss, and volumes of blood transfusion were recorded. The TNM classification was used for staging colorectal cancer disease [57]. The stage of tumors treated with neo-adjuvant chemotherapy and/or radiotherapy was evaluated clinically at the beginning of the treatment according to the nuclear magnetic resonance investigation, whereas the stage of tumors without neo-adjuvant treatment was diagnosed by pathohistologic examination.
After surgery, values of WBC, CRP, and PCT on post-operative days one, two, three, five, and seven were recorded. We recorded SIRS from post-operative day one to post-operative day three and post-operative infections up to 30 d after surgery. We followed SSIs (superficial, deep, organ/space), pneumonia, central venous catheter-related bloodstream infections (CRBSIs), and urinary tract infections (UTIs). We used criteria for SIRS updated in the year 2001 by the SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference [58] and criteria for nosocomial infections defined by U.S. Centers for Disease Control and Prevention (CDC) [59]. Only a single modification was made to this classification, namely combining the superficial and deep SSIs into one group because it was difficult to establish the depth of an infection based on retrospective data. After discharge the patients were examined again in the outpatient clinic in order to detect any complications. On the basis of the data from medical records and data in Cancer Registry of the Republic of Slovenia we followed the patients’ long-term five-year survival.
Biomarker measurements
The WBC count (reference range, 4–10 × 109/L) was analyzed with the use of a hematologic blood analyser (LH 75, Beckman Coulter, Holliston, MA). Serum concentration of CRP (normal range, 0–5 mg/L) was measured by the immunoturbidimetric method. Concentrations of PCT (normal range, 0–0.5 mcg/L) and CEA (normal range, 0–3.4 mcg/L) were measured by the electrochemiluminiscence method. The same analyzer was used for the last three parametres (Modular Analytics SWE, Roche Diagnostics, Indianapolis, IN).
Statistical analysis
We used medians and interquartile ranges to summarize non-normally distributed continuous parameters. The χ2 test was used for comparing category parameters and the Mann-Whitney U test for continuous parameters. The diagnostic accuracy of biomarkers CRP and PCT was assessed with the receiver operating characteristic (ROC) curve analysis. The ROC curve is obtained by plotting the sensitivity (fraction of true-positives, y-axis) and specificity (fraction of false-negatives, x-axis). The point on the ROC curve closest to the left upper corner represents the best cutoff value. The area under the receiver operating characteristic curve (AUROC) is a direct measure of the diagnostic accuracy of the test. The AUROC value greater than 0.50 indicates the ability of the test to significantly discriminate between positive and negative cases, whereas a test with an AUROC greater than 0.80 is considered to have a high diagnostic accuracy. The missing data were dealt with using available-case and complete-case approach.
Logistic regression analysis was used to predict the probability of infection. The survival analysis was performed using the Kaplan-Meier method and the differences among the patient groups were tested by the log-rank test. Prognostic factors were investigated by univariate and multivariable Cox proportional hazard model. The p values less than 0.05 (two-sided) were considered statistically significant. All analyses were performed with R statistical software, version 3.0.2 [60].
Results
A total of 186 patients were included in our study (107 males and 79 females) whose average age was 64.7. They underwent elective curative-intent rectal (62%) or colon (34%) resection. Baseline characteristics are shown in Table 1. Most patients were classified in ASA class II (61%) or III (18%). One hundred and twelve patients (60.2%) were treated with neoadjuvant radiotherapy and/or chemotherapy. Most of the tumors were classified as stage III (57%) with one or more positive regional lymph nodes, followed by stage II (25%), stage IV (12%), and stage I (6%). One hundred and forty-seven patients (79%) underwent large intestine resection with anastomosis and 14 patients (8%) underwent a synchronous liver metastases surgery.
t test.
χ2 test.
Fisher exact test.
TNM classification.
IQR-interquartile range
Mann-Whitney test.
Intra-operative.
SD = standard deviation; ASA = American Society of Anesthesiologists; BMI = body mass index; PRBC = packed red blood cells; SIRS = systemic inflammatory response syndrome; POD = post-operative day; SSI = surgical site infection; CVC = central venous catheter; IQR = interquartile range.
Infectious complications
Fifty-five patients (29.5%) developed infectious complications (infected group) and 131 patients did not (non-infected group). Sepsis was diagnosed in 23 patients (12.3%), which represents 41.8% of patients with infection. The most frequent post-operative infection was SSI. It was diagnosed in 43 patients (23.1%), followed by UTIs in five patients (9%), sepsis of unknown origin in four patients (7%), pneumonia in two patients (4%), and CRBSI in one patient (2%). The median day of the diagnosis of the infection was post-operative day six (interquartile range [IQR] 5–8.75). Re-operation was necessary in 15 patients (8%). Important risk factors for infection in univariate analysis were duration of surgery (p = 0.001) and intra-operative blood loss (p = 0.002). Liver resection was significantly associated with post-operative infection (p = 0.028), whereas the site of tumor resection was not (p = 0.232). Post-operative SIRS was significantly associated with later infection on post-operative day one (p = 0.042), post-operative day two (p = 0.008), and post-operative day three (p = 0.007). We did not include inter-operative hypothermia because we were not able to obtain reliable data from documentation. The Foley catheters were removed five to 10 d after surgery and central venous catheters one to two days before the end of hospitalizaton. The hospital stay of 17 d (IQR 15–23) in the infected group was significantly longer compared with 11 d (IQR 9–13) in the non-infected group (p < 0.001).
One patient with no post-operative infection died in the first month after surgery. The 30-d mortality was 0.5%. One-year mortality was higher in the infected group (13%) compared with the non-infected group (4%; p = 0.044). There was also a significant difference in five-year mortality between the infected (47%) and the non-infected groups (29%; p = 0.017).
Inflammatory markers
White blood cell counts increased on post-operative day one with no significant difference between the infected and the non-infected group (p = 0.327) and after post-operative day one gradually declined. The values in the infected group increased again on post-operative day five and were significantly higher compared with the non-infected group on post-operative day five (p = 0.002) and post-operative day seven (p < 0.001; Fig. 1). The numbers of available data for the inflammatory markers are presented in Figure 1.
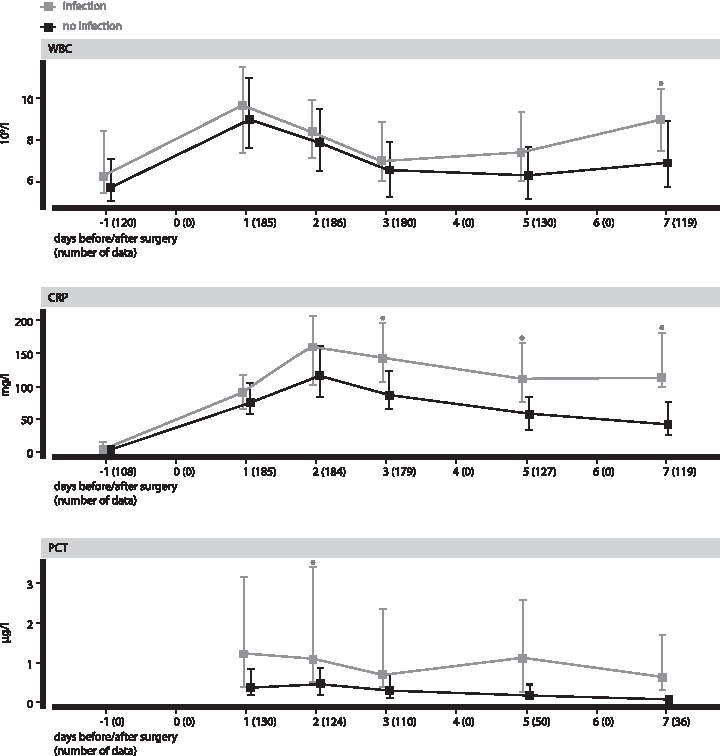
Post-operative values of WBC (109/L), CRP (mg/L), and PCT (mc/L) on the day before surgery (−1), post-operative day one, post-operative day two, post-operative day three, post-operative day five, and post-operative day seven in patients with infection and no infection. The squares represent the median values. The lower and upper limits of the vertical lines represent the 25th and 75th percentiles. The highest statistical difference between infected and non-infected groups is indicated by an asterisk (p < 0.001). WBC = white blood cell count; CRP = C-reactive protein; PCT = procalcitonin.
C-reactive protein concentration increased after the surgery and reached its peak on post-operative day two 160.0 mg/L (IQR 100.0–207.5) in the infected group and 117.0 mg/L (IQR 85.0–162.0) in the non-infected group (p = 0.001). C-reactive protein in the infected group increase from post-operative day one to post-operative day seven compared with the non-infected group, but the lowest p values were on post-operative days three, five, and seven (p < 0.001). In the infected group the decrease of CRP after post-operative day two was slower and slightly increased again after post-operative day five. In the non-infected group CRP decreased continuously to post-operative day seven and reached values that were still above normal. The lack of decrease in CRP concentrations is a predictor of post-operative infections in patients after colorectal surgery [52].
Procalcitonin reached its peak concentration on post-operative day one 1.2 mcg/L (IQR 0.4–3.2) in the infected group and 0.4 mcg/L (IQR 0.2–0.9) in the non-infected group (p = 0.002). Procalcitonin in the infected group increased from post-operative day one to post-operative day seven compared with the non-infected group, but the lowest p value was on post-operative day two (p < 0.001). In both groups PCT decreased after post-operative day one and in the infected group increased on post-operative day five again.
The ROC analysis was used to asses WBC, CRP, and PCT as early predictors of post-operative infections. The results are shown in Table 2. White blood cell counts were not found to be a good predictor of infection in the first three days after surgery. The cutoff value of 5.75 × 109/L on post-operative day three provided a sensitivity of 81% and low specificity of 37%. The AUROC was 0.575. The highest diagnostic accuracy for CRP was noticed on post-operative day three and for PCT on post-operative day two (AUROC 0.739 and 0.735, 95% confidence interval [CI] 0.66–0.82 for CRP and 0.64–0.83 for PCT; Figs. 2 and 3).
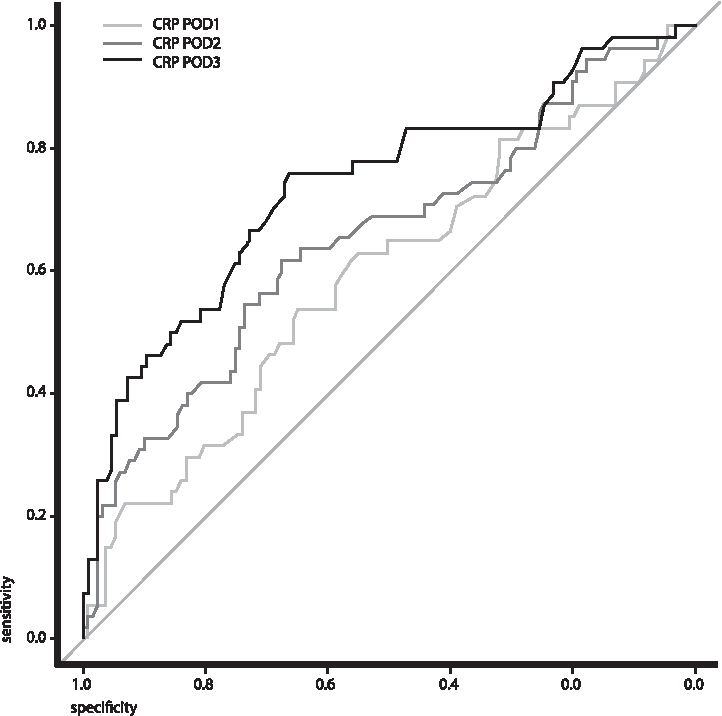
Receiver operating characteristic curve analysis of C-reactive protein (CRP) in the first three days after colorectal surgery. POD = post-operative day.
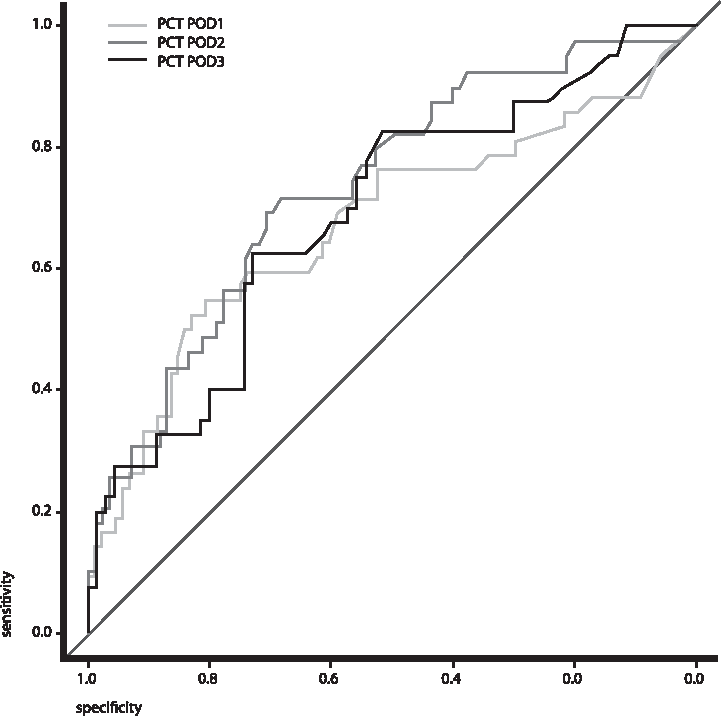
Receiver operating characteristic curve analysis of procalcitonin (PCT) in the first three days after colorectal surgery. POD = post-operative day.
AUC = area under the curve; CI = confidence interval; WBC = white blood cell count; CRP = C-reactive protein; PCT = procalcitonin.
A CRP cutoff value of 105.0 mg/L on post-operative day three provided a sensitivity of 66% and specificity of 76%. A PCT cutoff value of 0.685 mcg/L on post-operative day two provided a sensitivity of 68% and specificity of 72% in detecting post-operative infections.
The multiple logistic regression analysis included a total of five parameters, namely neo-adjuvant radiotherapy and/or chemotherapy, duration of surgery, loss of blood, CRP on post-operative day three, and WBC on post-operative day one. The results showed that only CRP on post-operative day three was an independent predictive factor for post-operative infections (odds ratio [OR] 1.18, 95% CI 1.11–1.27). Figure 4 shows the relation between CRP values on post-operative day three and the probability of a post-operative infection. CRP value of 175 mg/L on post-operative day three indicates a 50% probability (95% CI 0.39–0.62) and a value of 275 mg/L indicates an 85% probability of an infection (95% CI 0.66–0.94).
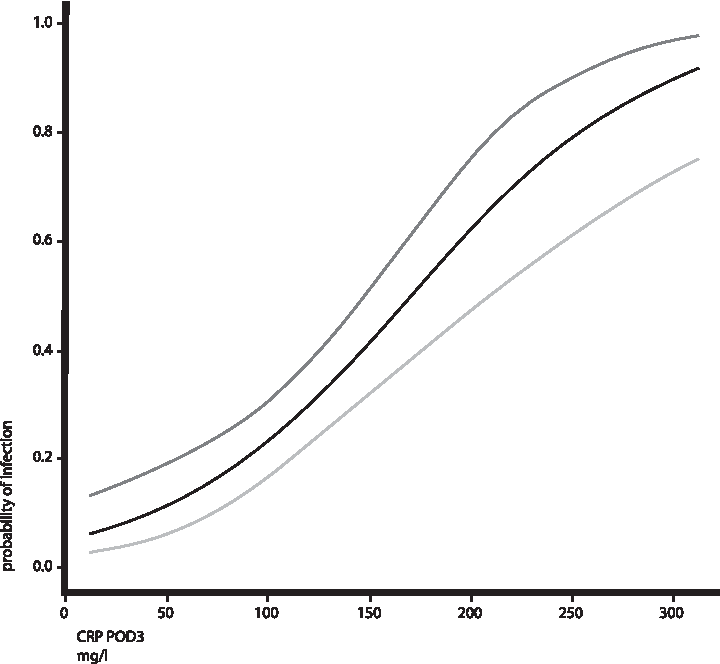
Relations between C-reactive protein (CRP) value on post-operative day three and probability of infection based on univariate logistic regression model. Dashed lines represent 95% confidence limits. POD = post-operative day.
Survival
The Kaplan-Meier analysis showed one-year survival in the non-infected group was 96.2% (95% CI 0.93–0.99) and 85.5% (95% CI 0.76–0.95) in the infected group. Five-year survival was higher in the non-infected group (70.8% [95% CI 0.63–0.79]) compared with the infected group (52.1% [95% CI 0.40–0.67]). The p value in log-rank test was 0.004.
We studied survival in different types of infection (incisional SSIs, organ/space SSIs, other infections). The lowest five-year survival was in the group with organ/space SSIs (40.9% [95% CI 0.24–0.67]), much higher in the group with incisional SSIs (66.7% [95% CI 0.49–0.90]), and in between was the group with other infections (46.3% [95% CI 0.24–0.87]). The p value in log-rank test was 0.002 (Fig. 5).
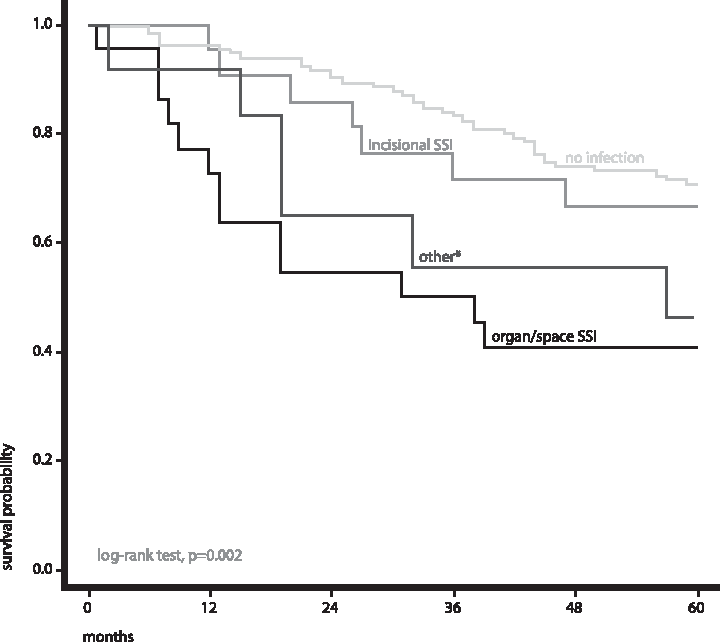
Five-year survival rate after colorectal surgery in patients with different types of infection. *Other infections include 12 patients with rare infections in the present study CVC sepsis, sepsis of unknown origin, pneumonia and urinary tract infection). CVC = central venous catheter; SSI = surgical site infection.
We studied survival also according to the stage of the disease. We coupled stage I and II, both with negative regional lymph nodes into one group. There was a significant difference among stages in the five-year survival. In stage I–II there was 87.5% survival (95% CI 0.793–0.966), in stage III 63.1% (95% CI 0.545–0.732), and in stage IV 15.3% (95% CI 0.0542–0.433). The p value in log-rank test was <0.001. We analyzed survival according to the stage of the disease and the post-operative infection combined. In stage I–II there was 90% survival in the non-infected group (95% CI 0.81–1.00) and 81% in the infected group (95% CI 0.64–1.00). The difference was 9%. In stage III there was a larger difference (19%) between survival in the non-infected group (68% [95% CI 0.58–0.79]) and 49% in the infected group (95% CI 0.33–0.73). In stage IV the survival in both groups was low: 21% in the non-infected group (95% CI 0.06–0.70) and 10% in the infected group (95% CI 0.02–0.64). p value in stratified log-rank test was 0.011 (Fig. 6). The effect of infection on survival in stage I and II is observed only after 24 months, but in stages III and IV already much earlier. This is probably because of an advanced cancer disease in stages III and IV and a high percentage of infections in this group of patients. There were 71% of all infections and 86.3% of organ/space SSIs in stages III and IV. We believe the post-operative chemotherapy did not influence survival.
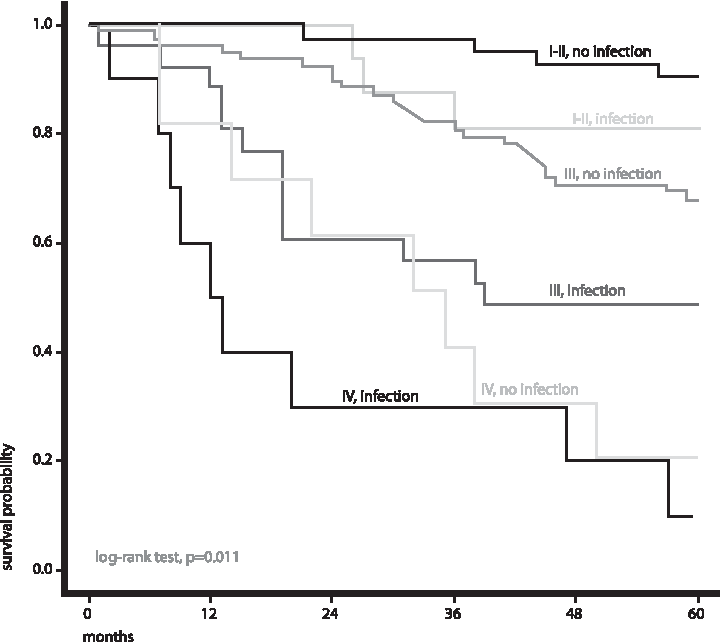
Five-year survival rate after colorectal surgery according to the post-operative infection and stage of disease. Stages I and II are coupled together. The method is stratified log-rank test.
Prognostic factors were analyzed by univariate and multivariable Cox proportional hazard model (Table 3). Multivariable analysis showed that independent factors associated with a worse five-year survival were post-operative infection (hazard ratio [HR] 2.11, 95% CI 1.22–3.68), age (HR 1.04, 95% CI 1.02–1.07), tumor stage III (HR 3.64, 95% CI 1.52–8.68), and tumor stage IV (HR 14.29, 95% CI 5.02–40.69). The pre-operative CEA value was a good prognostic factor in univariate Cox model (HR 1.02, 95% CI 1.01–1.03), however, in the multivariate model it was not.
HR = hazard ratio; CI = confidence interval; ASA = American Society of Anesthesiologists; CEA = carcinoembryonic antigen; PRBC = packed red blood cells.
Discussion
The aim of the present study was to compare WBC, CRP, and PCT as early predictive markers of post-operative infections after elective colorectal cancer surgery. We followed all types of post-operative infections. An important finding was that the highest diagnostic accuracy was observed for CRP on post-operative day three and for PCT on post-operative day two. Patients with CRP higher than the cutoff value 105 mg/L on post-operative day three or PCT higher than the cutoff value 0.685 mcg/L on post-operative day two should be followed strictly. Diagnostic procedures should be performed to confirm or exclude infection. In univariate logistic regression models, CRP concentration of 275 mg/L on post-operative day three was found to be a predictive factor for post-operative infection with an 85% probability. White blood cell count was not found to be a good early predictor for infection. We noticed late increase in WBC count only on post-operative day seven when clinical signs of infection have already started.
In recent years only few studies have compared the diagnostic accuracy of CRP and PCT for early detection of post-operative infections after colorectal surgery. The study reported by Oberhofer et al. [54] included 79 patients and showed similar results to the present study. C-reactive protein on post-operative day three and PCT on post-operative day two had similar predictive values for post-operative infections (AUROC 0.746 and 0.750) with the best cutoff values of 99 mg/L for CRP (sensitivity, 75.9%; specificity, 68.0%) and 1.34 mcg/L for PCT (sensitivity, 69%; specificity, 78.7%) [54]. Silvestre et al. [52] reported a pilot study that included 50 patients undergoing colorectal surgery. C-reactive protein time course from post-operative day one to post-operative day two was different in infected and non-infected patients, whereas PCT time course was not. C-reactive protein concentration greater than 50 mg/L on post-operative day six was predictive of post-operative infection with a sensitivity of 85% and a specificity of 62%. Procalcitonin was not helpful as a diagnostic marker [52]. Both of these studies were prospective. They included a much smaller number of patients than our study and they did not study WBC as a predictor of infection.
Lagoutte et al. [53] researched CRP and PCT as predictive markers of anastomotic leakage after elective colorectal surgery. They reported that in 100 patients CRP was a more accurate predictive marker than PCT for the detection of this serious infective complication. The best accuracy was obtained on post-operative day four (AUROC 0.869 for CRP and 0.750 for PCT) [53]. Garcia-Granero et al. [51] demonstrated that in 205 patients undergoing elective colorectal surgery, PCT was better than CRP for the early prediction of major anastomotic leak on post-operative days three, four, and five. An AUROC greater than 0.80 for both PCT and CRP showed that both are useful for early exclusion of anastomotic leak. The best predictor was PCT on post-operative day five with AUROC 0.867 and a cutoff value of 0.31 mcg/L, resulting in a 100% sensitivity, 72% specificity, 100% negative value, and 17% positive predictive value [51]. Takakura et al. [50] reported that in 114 patients with colorectal resection PCT on post-operative days one and three was an early predictor for surgical site infection (AUROC 0.76 and 0.77) and a more reliable marker compared with CRP. Multivariable analysis showed PCT on post-operative day one and post-operative day three was an independent predictor for SSIs (OR 14.41 and 9.79) [50]. More recently, in the Dominguez-Comesana et al. [61] study with 67 patients it was observed that PCT on post-operative days one, two, and three was a good marker of post-operative intra-abdominal infection with a high negative predictive value after surgery for gastrointestinal cancer. The quotient between value of CRP on post-operative day three and CRP on post-operative day two combined high negative and high positive predictive values [61]. In comparison with the present study the last four studies were prospective but they studied inflammation markers only as predictors of intra-abdominal infections and one of them all SSI.
Another important finding of the present study was that post-operative infection was an independent predictive factor of a worse five-year survival after colorectal cancer surgery. This applies specifically to stage III of the disease. In contrast to other studies the present study compared long-term survival among groups of patients with different types of infection. The Kaplan-Meier analysis showed the worst survival was in the group with organ/space SSIs. Organ/space SSI is often related to anastomotic leakage and is manifested as abscess, local, or diffuse peritonitis. In our study it was proved to be an important risk factor for a worse outcome. Some studies report anastomotic leakage is an independent risk factor for local and distant cancer recurrence and is associated with a worse long-term survival [62–64]. The retrospective study by Artinyan et al. [65] used data from large databases and included 12,075 patients with colorectal surgery. It reported the presence of any post-operative complication as being independently associated with a decreased long-term survival (HR 1.24, 95% CI 1.15–1.34). Multivariable analysis by complication type demonstrated an increased risk of infectious complications (HR 1.31, 95% CI 1.21–1.42), predominantly with severe infections (HR 1.41, 95% CI 1.15–1.73) [65]. Nespoli et al. [13] and Tsujimoto et al. [9] also reported that post-operative infection in patients after colorectal surgery was an independent predictive factor for a worse outcome. In a study of 1,657 patients undergoing resection of colorectal cancer, Law et al. [66] demonstrated that the presence of infectious or non-infectious post-operative complications was an independent factor associated with a high recurrence rate and a worse overall survival.
The unique aspect of the present study is that it analyzes the inflammation markers as predictive factors of post-operative infection and their impact on long-term survival in the same group of patients. The precise mechanisms relating post-operative infection and long-term survival are not completely clear. It is known that a major surgery causes global immunosuppression, related to the tissue injury, loss of blood, transfusion, anesthetic agents, opioids, pain, hormonal changes, age, and comorbidities [67,68]. Immunosuppression depends at least partially on the production of IL-6, which triggers an acute phase response, acts as a tumor growth factor, and decreases anti-cancer immunity [69]. There is a decrease in number and activity of cytotoxic T lymphocytes, natural killer (NK) cells, and dendritic antigen presenting cells [13,70]. Natural killer cell clearance of tumor cell emboli after surgery is believed to be vital in preventing post-operative metastases. Immunosuppression predisposes the patient to developing post-operative infections and progression of cancer [13,71,72]. Post-operative infections and peri-operative transfusion exaggerate cytokine response and cause further suppression of cell-mediated immunity [73,74]. Patients with peri-operative blood transfusion and subsequent development of post-operative infectious complications represent a group with a particularly poor prognosis, independent of tumor stage [75].
In the future, new treatment strategies may improve the survival of patients with colorectal cancer. In pre-clinical models it was found that pre-operative administration of oncolytic viruses could reverse NK cell suppression and reduce metastatic recurrence in surgical patients with cancer [76,77].
Conclusions
In the present study we found CRP on post-operative day three and PCT on post-operative day two were the best early predictors of post-operative infection complications after colorectal cancer surgery. We demonstrated that post-operative infection and tumor stage III–IV were independent factors associated with a worse five-year survival. Among the infections, organ/space SSI was proven to be the worst prognostic factor for long-term survival.
Footnotes
Author Disclosure Statement
No competing financial interests exist.