
Abstract
Abstract
Background:
Ceftaroline fosamil is a novel cephalosporin approved by the United States Food and Drug Administration (US FDA) for treatment of acute bacterial skin and skin structure infection, including those caused by methicillin-resistant Staphylococcus aureus (MRSA). We evaluated the activity of ceftaroline and comparator agents tested against S. aureus isolated from surgical skin and skin structure infections (SSSI).
Methods:
Clinically substantial isolates (one/patient episode) from SSSI were consecutively collected from 64 medical centers in the United States over a 6-y period (2008–2013) and tested for susceptibility by broth microdilution methods against ceftaroline and several comparator agents.
Results:
Among 794 strains tested, 50.5% were MRSA. Ceftaroline was active against all methicillin-susceptible Staphylococcus aureus (MSSA; minimal inhibitory concentration [MIC]90, 0.25 mcg/mL) and nearly all MRSA (MIC90, 1 mcg/mL). Against MSSA, ceftaroline was 16-fold more potent than ceftriaxone (MIC90, 4 mcg/mL) and the highest ceftaroline MIC was 0.5 mcg/mL. Among MRSA, 97.5% and 100.0% of strains were inhibited at ≤1 and ≤2 mcg/mL of ceftaroline. Furthermore, 27.4% and 67.5% of MRSA were resistant to clindamycin and levofloxacin, respectively. Daptomycin (MIC50/90, 0.25/0.5 mcg/mL), linezolid (MIC50/90, 1/2 mcg/mL), tigecycline (MIC50/90, 0.06/0.12 mcg/mL) and vancomycin (MIC50/90, 1/2 mcg/mL) were also highly active against S. aureus strains.
Conclusions:
Ceftaroline exhibited potent in vitro activity against S. aureus causing SSSI in a large number of US hospitals, including MRSA. On the basis of this in vitro data, ceftaroline fosamil may represent a valuable option for treatment of surgical SSSI, and should be further evaluated as an agent for surgical prophylaxis that would cover MRSA.
S
Staphylococcus aureus is the most common cause of surgical site infection, and methicillin (oxacillin)-resistant strains (MRSA) account for a large proportion of these infections [2]. Furthermore, compared with infections because of methicillin-susceptible Staphylococcus aureus (MSSA), MRSA infections have been associated with increased mortality rates, treatment failure, and increased length of hospital stay and costs [3]. The increasing prevalence of MRSA has resulted in a re-evaluation of the role of vancomycin for surgical prophylaxis. However, the emergence of gram-positive strains resistant to vancomycin and having weaker effectiveness against MSSA have been major reasons not to routinely use this agent for surgical prophylaxis [4,5].
Ceftaroline, the active metabolite of the pro-drug ceftaroline fosamil, is a broad-spectrum cephalosporin with bactericidal activity against resistant gram-positive organisms, including MRSA, multi-drug-resistant (MDR) strains of Streptococcus pneumoniae, and common gram-negative organisms, including non-ESBL-phenotype Enterobacteriaceae [6]. Ceftaroline fosamil is approved by the United States Food and Drug Administration (US FDA) for treatment of acute bacterial skin and skin structure infection, including those caused by MRSA, and community-acquired bacterial pneumonia [7]. Because of its potent anti-MRSA in vitro activity, this new cephalosporin may represent an alternative β-lactam (cephalosporin) option for prevention surgery-related infections (prophylaxis) in institutions with high prevalence of MRSA. In the present investigation, we evaluated the activity of ceftaroline and comparator agents tested against S. aureus strains isolated from surgical skin and skin structure infections (SSSI) in 64 U.S. hospitals.
Patients and Methods
The organism collection included 794 clinically relevant S. aureus isolates (one per patient) consecutively collected from surgical SSSI in 64 U.S. medical centers over a 6-y period (2008–2013). The isolates were collected through the AWARE (Assessing Worldwide Antimicrobial Resistance Evaluation) ceftaroline surveillance program and all medical centers collected the strains following a common protocol [6]. Target numbers of strains for each of the requested bacterial species/genus were pre-determined by study protocol, and only isolates determined to be substantial by local criteria as the reported probable cause of the infection were included in this investigation. The AWARE program monitors many bacteria genus/species from various infection types, but only S. aureus strains deemed to be the cause of a surgical SSSI were included in this investigation.
Isolates were sent to the coordinator laboratory (JMI Laboratories, North Liberty, Iowa) for confirmatory identification and reference susceptibility testing. Species identification was confirmed when necessary by Matrix-Assisted Laser Desorption Ionization-Time Of Flight Mass Spectrometry (MALDI-TOF MS) using the Bruker Daltonics MALDI Biotyper (Billerica, Massachusetts, USA) by following manufacturer instructions.
Isolates were tested for susceptibility to ceftaroline and multiple comparator agents by reference broth microdilution methods as described by Clinical and Laboratory Standards Institute (CLSI) M07-A10 [8] and interpretations were based on CLSI (M100-S25) [9], US FDA (when CLSI breakpoints were not available) [10] and EUCAST [11] breakpoint criteria. Validated MIC panels were manufactured by Thermo Fisher Scientific (Cleveland, Ohio) and isolates were tested in cation-adjusted Mueller-Hinton broth. Concurrent testing of quality control (QC) strains assured proper test conditions.
Results
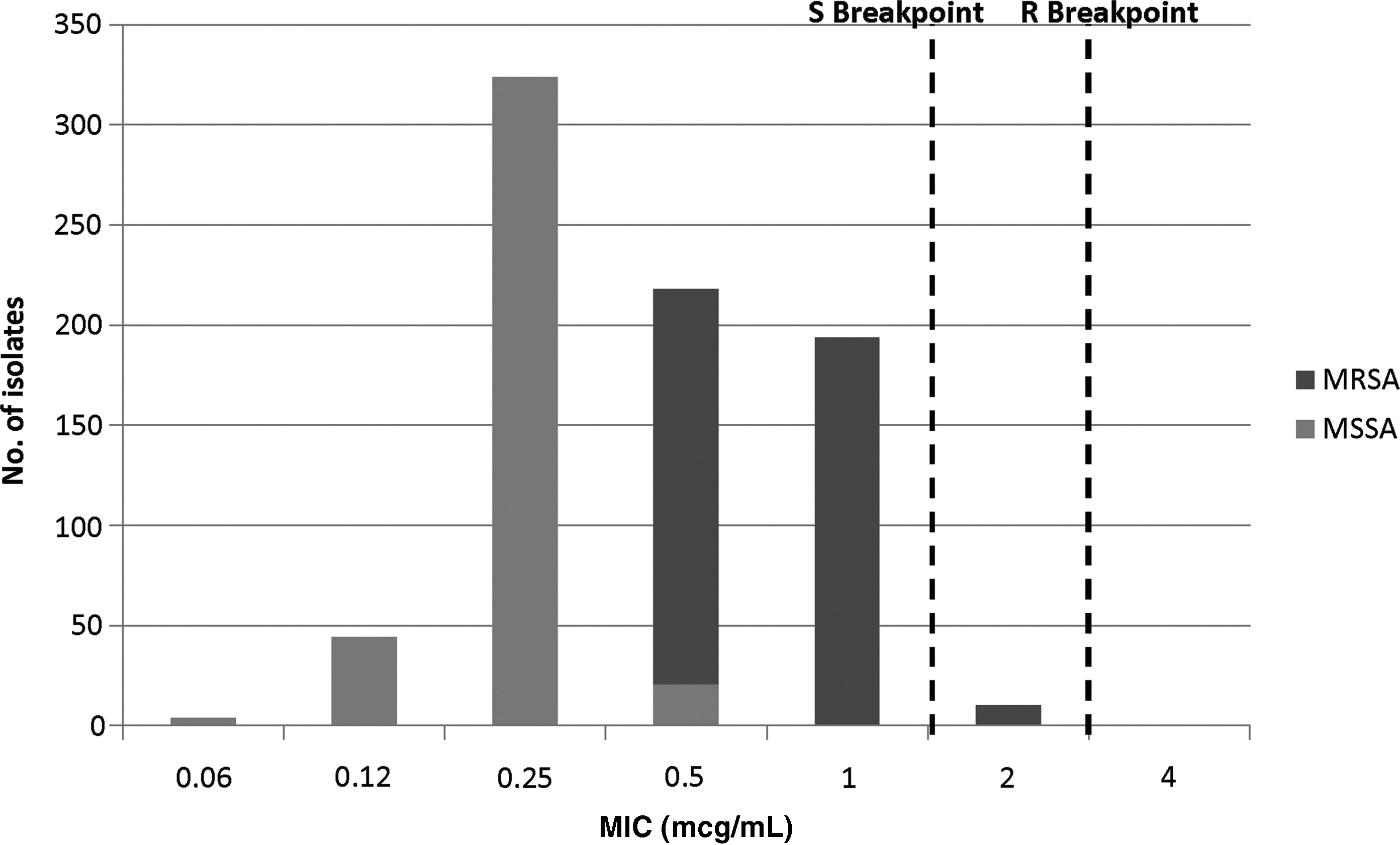
The overall MRSA rate was 50.5% and ceftaroline was active against both MSSA (MIC50 and MIC90, 0.25 mcg/mL; 100.0% susceptible) and MRSA (MIC50 and MIC90, 1 mcg/mL; 97.5% susceptible; Table 1 and Figure 1). Overall, 1.3% of S. aureus isolates were non-susceptible to ceftaroline, with no important variation over the years. The percentages of ceftaroline-non-susceptible isolates were 1.3%, 0.0%, 1.6%, 0.0%, 1.9%, and 0.8% in 2008, 2009, 2010, 2011, 2012, and 2013, respectively, and all ceftaroline-non-susceptible isolates exhibited ceftaroline MIC of 2 mcg/mL (intermediate according to CLSI breakpoint criteria [9]). Susceptibility rates (CLSI [9]) for erythromycin (MIC50 and MIC90, >4 mcg/mL), clindamycin (MIC50, ≤0.25 mcg/mL and MIC90, >2 mcg/mL) and levofloxacin (MIC50, ≤0.5 mcg/mL and MIC90, >4 mcg/mL) were 36.8%, 82.5%, and 58.7%, respectively; and daptomycin (MIC50, 0.25 mcg/mL and MIC90, 0.5 mcg/mL), linezolid (MIC50, 1 mcg/mL and MIC90, 2 mcg/mL), tigecycline (MIC50, 0.06 mcg/mL and MIC90, 0.12 mcg/mL) and vancomycin (MIC50 and MIC90, 1 mcg/mL) were active against all (100.0%) S. aureus isolates at the respective susceptible breakpoint (Table 2).
Ceftaroline activity when tested against 793 Staphylococcus aureus isolates from surgical skin and skin structure infections.
MRSA = methicillin-resistant S. aureus; MSSA = methicillin-susceptible S. aureus; MIC = minimal inhibitory concentration.
Criteria as published by the CLSI [2014] and EUCAST [2014]. S = susceptible, I = intermediate, R = resistant.
TMP/SMX: trimethoprim/sulfamethoxazole.
In the absence of CLSI breakpoint, US FDA breakpoints were applied when available [10].
MIC = minimal inhibitory concentration; CLSI = Clinical and Laboratory Standards Institute; EUCAST = European Committee on Antimicrobial Susceptibility Testing.
When tested against MSSA, ceftaroline (MIC50 and MIC90, 0.25 mcg/mL) was 16-fold more potent than ceftriaxone (MIC50 and MIC90, 4 mcg/mL), four- to eight-fold more potent than vancomycin (MIC50 and MIC90, 1 mcg/mL) and linezolid (MIC50, 1 mcg/mL and MIC90, 2 mcg/mL), and slightly more active than daptomycin (MIC50, 0.25 mcg/mL and MIC90, 0.5 mcg/mL; Table 1). The highest ceftaroline MIC among MSSA was 0.5 mcg/mL and 94.7% of strains had a ceftaroline MIC of 0.25 mcg/mL or less (Table 1).
Among MRSA, 97.5% and 100.0% of strains were inhibited at ≤1 and ≤2 mcg/mL of ceftaroline, respectively (Table 1); whereas all other β-lactams exhibited limited activity against this organism (data not shown). Daptomycin (MIC50, 0.25 mcg/mL and MIC90, 0.5 mcg/mL), linezolid (MIC50, 1 mcg/mL and MIC90, 2 mcg/mL), tigecycline (MIC50, 0.06 mcg/mL and MIC90, 0.12 mcg/mL) and vancomycin (MIC50 and MIC90, 1 mcg/mL) were also active against MRSA strains; whereas resistance to clindamycin (MIC50, ≤0.25 mcg/mL and MIC90, >2 mcg/mL) and levofloxacin (MIC50, 4 mcg/mL and MIC90, >4 mcg/mL) were 27.4% and 67.5% among MRSA strains, respectively (Table 2).
Discussion
Data reported to the National Healthcare Safety Network (NHSN) at the U.S. Centers for Disease Control and Prevention (CDC) indicated that S. aureus represents the leading cause of SSSI in U.S. hospitals [2]. During the 2009–2010 period, S. aureus was isolated from 30.4% of surgical site infections, and 43.7% of isolates were resistant to oxacillin/methicillin (MRSA). Other organisms commonly isolated from SSSI were CoNS (11.7%) and Escherichia coli (9.4%). These three organisms, which are generally susceptible to ceftaroline, accounted for 51.5% of the cases reported to the NHSN [2,6,12].
One of the greatest roles of the antimicrobial agents has been supporting the advancements of surgery. After proper surgical technique, antimicrobial prophylaxis is a major factor in minimizing the risk of post-operative infection morbidity [4]. On the basis of their characteristics of acceptable antibacterial spectrum, low incidence of allergy and safety, the cephalosporins has been the drug of choice for the vast majority of surgery prophylaxis procedures for many years. However, the increasing prevalence of MRSA as a cause of surgical site infections has resulted in the evaluation of other antimicrobial classes for antimicrobial prophylaxis [5]. MRSA and CoNS have become primary cause of SSSI in cardiothoracic, vascular, and neurosurgical procedures in many U.S. medical centers [4,5]. Furthermore, the prevalence of community-acquired MRSA strains have increased substantially in the United States in the last decade and are now responsible for a substantial proportion of SSSI [13,14]. Thus, vancomycin or other anti-MRSA agents have been frequently recommended as either a primary or adjuvant agent for surgical prophylaxis in patients who are presumed or known to have S. aureus colonization in institutions where a high prevalence of MRSA exists, and when surgical procedures involves a prosthetic joint insertion, sternotomy, or vascular graft insertion [15].
Because of its in vitro activity against MRSA and narrow spectrum of antimicrobial activity (i.e., lack of activity against gram-negative organisms); vancomycin has been the anti-MRSA agent of choice for surgical prophylaxis when the risk for MRSA is high. However, data suggest that vancomycin is less effective than cefazolin for preventing surgical site infections caused by MSSA [16,17]. Furthermore, for procedures where gram-negative organisms may cause surgical site infection, an additional agent with activity against these organisms should be considered [4].
Ceftaroline fosamil is the first cephalosporin approved in the United States for treatment of adults with acute bacterial skin and skin structure infection caused by MRSA [7]. In the present study, ceftaroline exhibited potent in vitro activity against S. aureus, both MSSA and MRSA, causing SSSI in U.S. hospitals. Ceftaroline activity against MSSA (MIC50 and MIC90, 0.25 mcg/mL) was 16-fold greater than that of ceftriaxone (MIC50 and MIC90, 4 mcg/mL) and more similar to that reported for cefazolin (MIC50 and MIC90, 0.5 mcg/mL) [18]. Furthermore, ceftaroline retained activity against MRSA with no trend to increase non-susceptibility rates during the study period. Previous studies performed by our group as well as other investigators have shown that amino acid alterations in the non-penicillin-biding or dimerization domain of PBP2a could possibly be responsible for decreased ceftaroline affinity for PBP2a and a slight elevation in the ceftaroline MIC to 2 mcg/mL [19,20]. It has also been demonstrated that additional alterations in the penicillin-biding or transpeptidase domain are necessary to further elevate ceftaroline MIC to the resistance level of ≥4 mcg/mL, and S. aureus isolates with this degree of ceftaroline resistance (MIC of ≥4 mcg/mL) are still rare in the U.S. [6,19,20]. In summary, ceftaroline showed comparable activity against MRSA as standard surgical prophylaxis agents and could possibly be examined further for the use of MRSA surgical prophylaxis.
Footnotes
Acknowledgments
The authors would like to thank all participants of AWARE program for providing bacterial isolates.
This study was supported by Cerexa, Inc., an Allergan affiliate. Forest Laboratories, LLC, an Allergan affiliate provided financial support for the analysis of the data and was involved in the design and decision to present these results. Neither Cerexa, Inc. nor Forest Laboratories, LLC, had any involvement in the collection, analysis, and interpretation of data.
Author Disclosure Statement
JMI Laboratories, Inc., has received research and educational grants in 2012–2014 from Achaogen, Actelion, Affinium, American Proficiency Institute (API), AmpliPhi Bio, Anacor, Astellas, AstraZeneca, Basilea, BioVersys, Cardeas, Cempra, Cerexa, Cubist, Daiichi, Dipexium, Durata, Exela, Fedora, Forest Research Institute, Furiex, Genentech, GlaxoSmithKline, Janssen, Johnson & Johnson, Medpace, Meiji Seika Kaisha, Melinta, Merck, Methylgene, Nabriva, Nanosphere, Novartis, Pfizer, Polyphor, Rempex, Roche, Seachaid, Shionogi, Synthes, The Medicines Co., Theravance, ThermoFisher, Venatorx, Vertex, Waterloo, Wockhardt, and some other corporations. Some JMI employees are advisors/consultants for Astellas, Cubist, Pfizer, Cempra, Cerexa-Forest, and Theravance. In regards to speakers bureaus and stock options-none to declare.