
Abstract
Abstract
Background:
Major resections for esophageal, gastric, hepatic, pancreatic, and colorectal cancer continue to be associated with a high peri-operative morbidity of up to 30%–40%. To a large extent, this morbidity is caused by infectious complications that add up to a considerable burden to patients and hospital costs. The objective of this large retrospective cross-sectional study was to determine independent patient and operation-related risk factors for infectious complications after major abdominal cancer operations to elucidate how infection rates can be reduced and improve health-care quality.
Patients and Methods:
In 1,389 cancer patients who underwent a major resection procedure between 2009 and 2013, infectious complications and their independent determinants were analyzed by multivariable logistic regression (p < 0.05).
Results:
Male gender was a risk factor for infections in general, whereas patients ≥65 y (odds ratio [OR] 1.75; p = 0.008), urinary tract infection (OR 0.51; p = 0.004), American Society of Anesthesiologists score (OR 1.55; p = 0.004), overall (OR 1.70; p = 0.037), vascular (OR 1.59; p = 0.020), and neurologic comorbidity (OR 2.22; p = 0.001) were associated significantly with pneumonia. Intra-abdominal drainage (OR 1.41; p = 0.024) and a duration of surgery of ≥180 min (OR 1.85; p = 0.001) were risk factors for surgical site infections. Total parenteral nutrition was significantly associated with intravascular catheter-induced infections (OR 18.09; p < 0.001) and sepsis (OR 6.69; p < 0.001).
Conclusions:
In this study, several independent risk factors for infectious complications in major abdominal cancer operations were identified, providing opportunities for further reducing peri-operative infections. General awareness and focus on preventing infectious complications may have a significant impact on health-care outcomes and costs.
M
Post-operative infections in patients who have undergone surgical procedures can lead to prolonged surgical incision healing, disability, increased length of hospital stay, increased overall cost of hospital care, and even death [8–10]. Over time, such consequences have decreased with the advent of prophylactic as well as therapeutic antibiotic agents. Another potential way to reduce complications may be to concentrate complex surgical procedures in dedicated hospitals. Several studies have shown a decreased mortality rate after centralization of complex abdominal operations [11,12]. Studies addressing the potential effect of centralization on morbidity and infections, however, are scarce.
Risk factors for post-operative infections after surgical procedures in general have been determined previously. Increasing age, increasing body mass index (BMI), more severe American society of Anesthesiologists (ASA) score, comorbidity, and prolonged duration of operation are known predictors of SSI [13].
Recent literature has reported on infectious complications, however diagnosed after general surgical procedures or colorectal operations only and with a limited scope to merely SSI [7,14–19]. We are unaware of any studies to date that focused on all types of infectious complications after major abdominal cancer operations. To prevent or minimize infectious complications, it is important to gain insight into their risk factors [6–8].
Therefore, as part of a quality improvement project, to assess which risk factors are eligible for improvement, we determined the pre-operative, intra-operative, and post-operative independent risk factors for infectious complications after major abdominal cancer resection procedures at a large Dutch teaching hospital.
Patients and Methods
Study area and design
A retrospective, cross-sectional study was performed in Isala, an 883-bed tertiary care hospital in Zwolle, The Netherlands. The study population consisted of 1,389 patients (N) who between 2009 and 2013 underwent at least one of five types of complex, elective operations: Pancreatic, gastric, esophageal, liver, or colorectal resection procedure. If more than one surgical resection was performed during the surgical intervention, the main surgical resection was included in this study. Patients with gastric, esophageal, or rectal cancer always received neo-adjuvant therapy. In cases of colorectal cancer, adjuvant therapy was only used for stage N1 tumors. Patients were excluded if an infection already existed before the operation.
Data collection
Demographic data, health status, operation reports, and infectious complications information were obtained from patient records, the clinical microbiology laboratory, and the patient database kept by the surgery department. The use of the obtained data was approved and judged to be exempt from ethical review procedures by the Isala Ethical Review Board.
Determinants
Determinants were selected a priori based on the literature (Fig. 1). Of the pre-operative determinants, age was classified into two categories: <65 y and ≥65 y [20]. The determinant gender was analyzed. The BMI was divided into three classifications: Underweight (BMI <18.5), normal (BMI ≥18.5 – <30), and overweight/obese (BMI ≥30) [21]. The ASA score indicates the health status of patients before surgery (1–5) [22]. The determinant patient comorbidity comprised cardiac, vascular, gastrointestinal, pulmonary, neurologic, endocrine, urogenital, thrombotic, musculoskeletal, and diabetic disease. In addition, cardiac, vascular, pulmonary, neurologic, and diabetic comorbidities were analyzed as separate determinants.
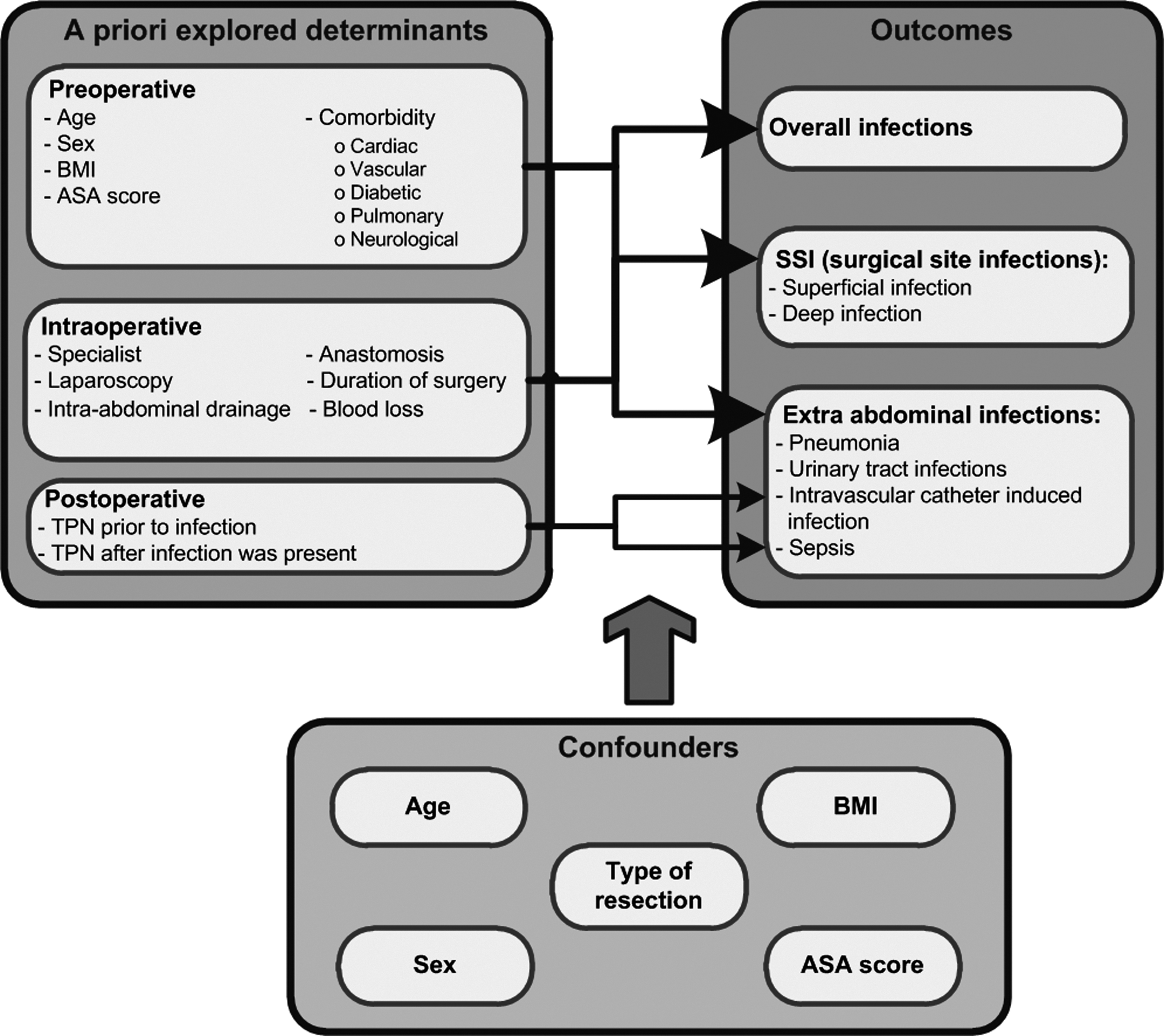
Pre-operative, intra-operative and post-operative determinants were selected a priori based on the literature. The pre-operative and intra-operative determinants were analyzed by multivariable logistic regression for all outcomes (overall infections, surgical site infections, and extra-abdominal infections). The post-operative determinants were analyzed only for intravascular catheter-induced infection and sepsis. Within the stepwise-backward multivariable logistic regression model, potential confounders such as age, gender, type of resection, body mass index, and American Society of Anesthesiologists (ASA) score were examined. BMI = body mass index; TPN = total parenteral nutrition.
Of the intra-operative determinants, the determinant “specialist” was defined as a qualified, highly experienced surgeon as opposed to a resident still in training. The type of operation was scored (laparoscopy or laparotomy) as was the use of intra-abdominal drains. An anastomosis of the digestive tract was only determined for patients who underwent colorectal surgery, because in other organ resection procedures, an anastomosis was always constructed. The duration of surgery was categorized as <120 min, 120–180 min, and >180 min, the volume of blood loss as ≤299 mL, 300–999 mL, and ≥1,000 mL [14,15,23].
Total parenteral nutrition (TPN) was determined as the start of TPN up to 30 d after the surgical procedure. In addition, patients receiving TPN were divided into two groups: Patients who did not have a post-operative infection before receiving TPN and, respectively, patients in whom a post-operative infection was already present before receiving TPN. TPN was only studied as a risk factor for TPN-related infections such as intravascular catheter-induced infections and sepsis.
Outcomes
Infectious complications (Fig. 1) up until and including 30 d after the surgical procedure were diagnosed by the treating physician, based on at least one of the following symptoms: Pain, fever, purulent drainage, swelling, redness and warmth of the surgical incision, increased C-reactive protein and leukocyte count.
Whether a sample needed to be taken and sent to the microbiology laboratory for diagnosis was at the discretion of the physician. SSI, following the Centers for Disease Control and Prevention guideline, included superficial infections of skin and subcutaneous tissue, deep infections involving fasciae and or or muscles, and deep organ/space infections (Table 1) [24]. Extra-abdominal infections were diagnosed based on radiologic imaging and relevant laboratory protocols, and whether a patient had one or more of the following infections: Pneumonia, UTI, intravascular catheter-induced infection or sepsis, according to standard protocols (Table 2) [25–27]. Supporting information for the diagnosis of infectious complications was provided by other diagnostic procedures such as diagnostic imaging, endoscopy, puncture, or a biopsy. Further, overall infection was defined as present if a patient had at least one type of SSI or any extra-abdominal infection.
SSI = surgical site infections.
Statistical analysis
Descriptive statistics were used for baseline characteristics and percentages of infectious complications. The statistical analysis was a combination of a predicted and an associated approach, in which the a priori selected determinants were entered in a univariate logistic regression model separately. A multivariable logistic regression model was used to examine the association between determinants and infectious complications. The determinants with p ≤ 0.10 in the univariate logistic regression were included into the multivariable logistic regression model with statistical significance at p < 0.05.
Within the stepwise-backward multivariable logistic regression model, potential confounders (Fig. 1) were examined and considered as confounders if the difference between the crude and adjusted β-coefficient of the determinant was ≥10%. All statistical analyses were performed using SPSS software version 22 for Windows (IBM SPSS Statistics, IBM Corporation, Armonk, NY) and expressed by odds ratios (OR) with 95% confidence intervals (CI).
Results
The characteristics of the pre-, intra-, and post-operative determinants in our study population (N = 1,389) are shown in Table 3. The median age of the study population was 69 (interquartile range 61–77) y, and 806 (58%) patients were male.
IQR = interquartile range; BMI = body mass index; ASA = American Society of Anesthesiologists.
In total, 389 (28%) patients had post-operative infectious complications (Table 4). Of these, 216 (15.6%) patients had a type of SSI, classified in 146 patients (10.5%) as a superficial infection and in 112 (8.1%) patients as a deep infection. Further, a total of 247 (17.8%) patients had an extra-abdominal infection.
Extra-abdominal infection was classified as pneumonia present in 132 (9.5%) patients, as UTI present in 80 (5.8%) patients, intravascular catheter-induced infection in 40 (2.9%) patients), and sepsis in 52 (3.7%) patients.
Univariate analysis results are summarized in Tables 5a and 5b. Table 6a shows the associations in multivariable analysis between the eight independent variables and overall infection, SSI, superficial, and deep infections.
Bold values indicate statistical significance (p < 0.10)
Anastomosis was only determined for patients who underwent colorectal surgery.
SSI = surgical site infections; OR = odds ratio; CI = confidence interval; BMI = body mass index; ASA = American Society of Anesthesiologists.
Bold values indicate statistical significance (p < 0.10).
Anastomosis was only determined for patients who underwent colorectal surgery.
OR = odds ratio; CI = confidence interval; BMI = body mass index; ASA = American Society of Anesthesiologists; TPN = total parenteral nutrition.
Bold values indicate statistical significance (p < 0.05).
All analyses were adjusted for gender, age, ASA score, type of resection, and BMI. In addition to this, a confounder was omitted only if the determinant was equal to the confounder.
Anastomosis was only determined for patients who underwent colorectal surgery.
SSI = surgical site infections; OR = odds ratio; CI = confidence interval; BMI = body mass index; ASA = American Society of Anesthesiologists.
Age ≥65 y, male gender, increased ASA score, neurologic comorbidity, specialist, and intra-abdominal drainage yielded an OR between 1.25 and 1.51. Duration of surgery of >180 min measured against 120–180 min was an important risk factor for SSI (OR 1.85), superficial infections (OR 1.94) and deep infections (OR 1.67). Duration of surgery of 120–180 min versus <120 min was significantly associated with overall infections only. Finally, laparoscopy was identified as a significant protective factor of overall infections (OR 0.55).
The multivariable analysis (Table 6b) disclosed the following risk factors for extra-abdominal infections: Age ≥65 y, male gender, being underweight or overweight, ASA score, having any type of comorbidity, cardiac, vascular, pulmonary, and neurologic comorbidity specifically, and TPN. TPN given before infection as well as TPN given after onset of infection was highly associated with intravascular catheter-induced infections (OR 18.09; OR 7.08) and sepsis (OR 6.69; OR 12.84). Finally, laparoscopy and an anastomosis were identified as protective factors for extra-abdominal infections (OR 0.36) and UTI (OR 0.44), respectively.
Bold values indicate statistical significance (p < 0.05).
All analyses were adjusted for gender, age, ASA score, type of resection, and BMI. In addition to this,
a confounder was omitted only if the determinant was equal to the confounder.
Anastomosis was only determined for patients who underwent colorectal surgery.
OR = odds ratio; CI = confidence interval; BMI = body mass index; ASA = American Society of Anesthesiologists; TPN = total parenteral nutrition.
A specialist surgeon as opposed to an operating resident (supervised by a specialist surgeon) was found to be a risk factor for SSI. After recalculating the association between specialist and SSI while considering duration of surgery as a confounder, however, it was no longer statistically significant (OR 1.24, p = 0.175).
Discussion
In the present study, we identified several independent patient and operation-related risk factors associated with infectious complications after major abdominal cancer resection procedures. These include factors known from other studies such as age ≥65 y, male gender, a higher ASA score, comorbidity, abnormal BMI, intra-abdominal drainage, and prolonged duration of surgery [7,14–19]. These studies, however, focused on a few types of infectious complications, mainly SSI, occurring after general or colorectal surgical procedures but not on complications of major abdominal cancer resection procedures.
For SSI and the specific types of SSI, our study showed a significantly higher risk of infection when the operation lasted 180 min or longer compared with operations of 120–180 min, which is consistent with other studies [14,15]. This is explained by the on average longer operating times needed for more complex and extensive resection procedures (e.g., for large T4 tumors). The risk resulting from a prolonged duration may be reduced by strictly administering antimicrobial prophylaxis at correct repeated time intervals during the operation [28].
The determinant laparoscopy was a protective factor of overall and extra-abdominal infections. We expected laparoscopy to be a significant protective factor for overall SSI and its specific types separately [29,30]. Our study could not corroborate this, however. The reason for this could be that the use of a laparoscope is associated with a longer duration of surgery, which is in accordance with a meta-analysis from 2010 [31]. Laparoscopic procedures embedded in complex operations could be a protective factor for post-operative infections.
An abnormal BMI is known to be related to SSI [7]. In our study, either underweight or overweight was associated with intravascular-induced catheter infections but not with SSI. Both associations with catheter infections were found by others [7,32,33]. Patients who are underweight will be prescribed TPN more frequently after surgery. If the patients would be supplemented in the pre-operative phase to achieve a target weight, this would allow less use of TPN and subsequently less use of intravascular catheters. The recommendation to overweight and obese patients would be to achieve a healthier weight before operation as well, because obesity and a subsequent prolonged duration of operation lead to higher SSI rates [7,18,34]. We realize however, that this in general will not be feasible.
TPN administered before infection as well as TPN administered after onset of infection were highly associated with intravascular-induced infections and sepsis, which is consistent with other studies [35–37]. The high risk of intravascular-induced catheter infections and sepsis is a major factor leading to an overall preference for enteral nutrition over parenteral nutrition [38]. If parenteral nutrition cannot be avoided, however, other modifiable factors must be taken into consideration. Increased parenteral caloric intake is an independent risk factor for sepsis in patients receiving TPN [39]. If underweight patients had obtained their target weight by supplementation in the pre-operative phase, low doses instead of high doses of TPN could have been administered.
Intra-abdominal drains induce an open connection, so dirty abdominal fluid (alias pus) is drained from the body. This can prevent deep infections, but still superficial infections can occur easily [16]. Within our hospital, no protocol was available indicating the conditions for using a drain. The use of these supportive therapies during surgical procedures is usually at the discretion of the treating surgeon but could, together with our obtained results, be standardized in the form of best practices as established by the treating surgeons [16]. This standardization may permit better evaluation and subsequent improvement of in-hospital quality.
Colorectal surgical procedures specifically resulted in UTI more often, although laparoscopy was identified as a protective factor for UTI in this type of surgery [40]. Laparoscopy is increasingly applied in these cases, unless impossible because of tumor size, growth into adjoining (organ) tissue, or adhesions as a result of previous operation. Another way to reduce UTI rates in surgical patients would be to remove an indwelling urinary catheter within two days after surgery and to implement standardized catheter management [41–43].
In our study, smoking as a risk factor was not included as a separate determinant of infectious complications, but we analyzed the resulting potential risk factor pulmonary comorbidity. Because the effectiveness of antibiotic prophylaxis has been proven extensively for a large number of surgical interventions previously, we also did not study this as a separate determinant [29,44].
Reducing infectious complications of complex surgical procedures can be achieved in various other ways. Registering infectious complications will by itself lead to an increased awareness of ways of prevention, stimulating protocol adherence, resulting in lowering SSI incidence. Following the implementation of national surveillance programs to this end in different countries, SSI rates have significantly decreased [45–49]. Another “soft value” that translates into hard quality results is the behavior of the surgical team. Good teamwork leads to better patient outcomes [50]. Installing a quality management system, with regular feedback of the achieved rates of infectious complications, also stimulates the surgical team to achieve better results [50–52]. In addition, in recent years the implementation of a so-called care bundle has been shown to reduce SSI further [53–55].
Another source of improvement lies in the modifiable, improvable risk factors of the patients, the operation, and, respectively, the post-operative care, which was the reason for undertaking this study. Also, efforts could be made to deploy the most able surgical team to reduce infectious complications in patients in the highest not modifiable risk bracket. A typical example would be the elderly, male patient with a high ASA score and cardiovascular comorbidity who undergoes colorectal surgery.
To our knowledge, this is the first multivariable study that evaluated risk factors specifically for all types of infectious complications after complex cancer operations. A limitation of our study could be that, in practice, the recognition of symptoms and subsequent diagnosis of infectious complications is based partly on subjective perceptions and experiences of physicians, which might lead to subtle differences in follow-up. In our study, we analyzed patient data up to 30 days after operation; however, infectious complications occurring after this arbitrary period were not included, permitting underestimation bias.
Conclusion
This study identified several independent risk factors for infectious complications in major abdominal cancer surgical procedures, providing opportunities to further reduce perioperative infections. Careful registration of morbidity, general awareness by internal and external audits, and focus on preventing infectious complications may have a significant impact on health-care outcomes and cost.
Footnotes
Author Disclosure Statement
No competing financial interests exist.