
Abstract
Abstract
Background:
Tuberculous infection has declined in the United States but remains a major infectious disease with morbidity and death for millions of people. Although the primary therapy is drugs, complications of the disease require surgical interventions.
Methods:
The published literature on tuberculosis was reviewed to provide a current understanding of the medical treatment of the disease and to define those areas where surgical intervention continues to be necessary.
Results:
Multi-drug therapy for tuberculosis has become the standard and has reduced the complications of the disease necessitating surgical intervention. However, multi-drug resistance and extensively drug-resistant tuberculosis continue to be major problems and require effective initial therapy with surveillance to define resistant infections. The roles of surgery in tuberculosis are in establishing the diagnosis in extra-pulmonary infection and in the management of complications of disseminated disease. Tuberculosis remains an occupational risk for surgeons and surgical personnel.
Conclusion:
Tuberculosis is still a global problem, mandating recognition and treatment. Surgeons should have an understanding of the diverse presentation and complications of the disease.
T
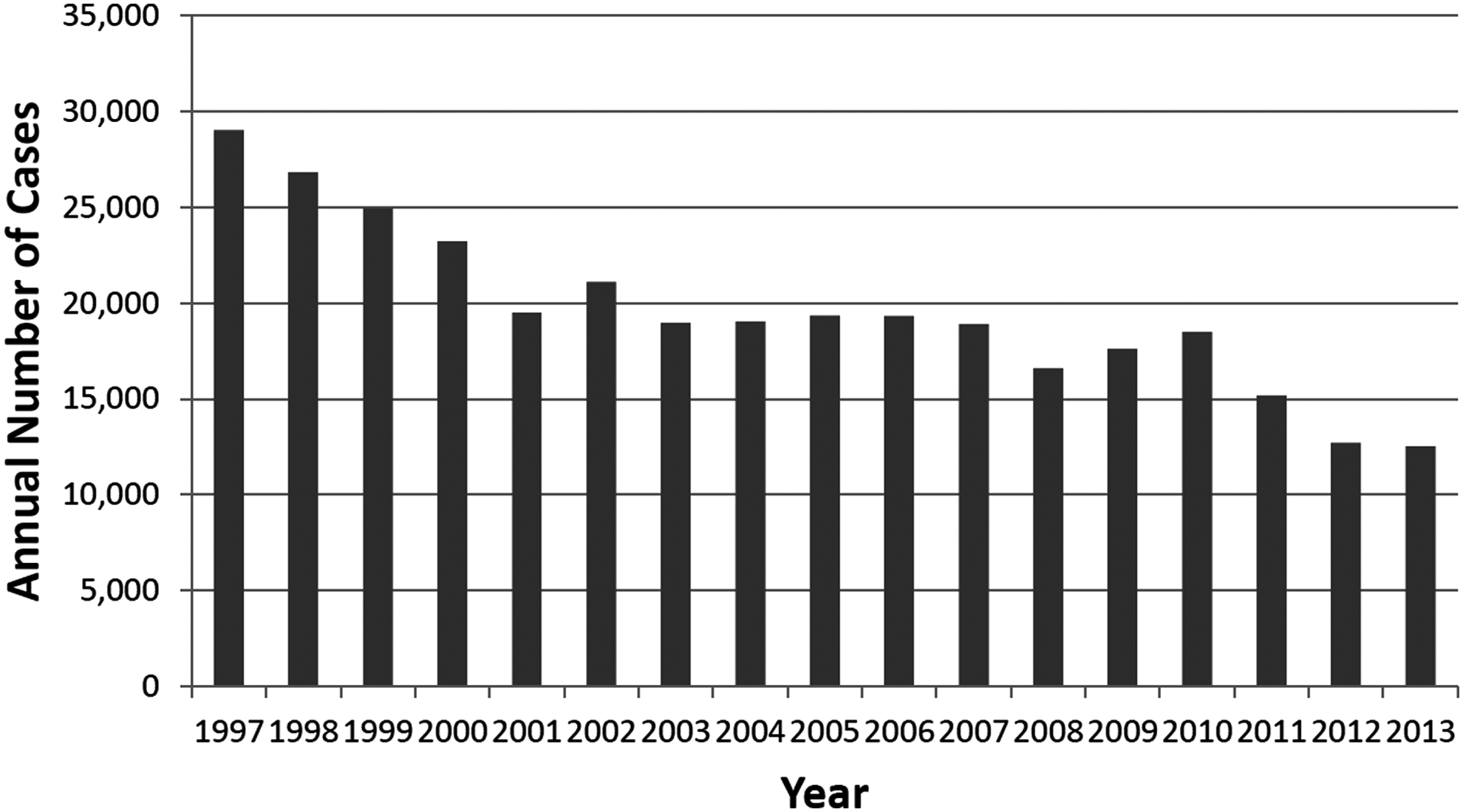
Estimated annual admissions to U.S. hospitals of patients with tuberculosis over the last 17 y [4].
Unfortunately, TB remains a major cause of infection in many third-world countries and globally accounts for millions of new infections and associated deaths. Efficient transportation from one continent to another means that active TB cases from endemic areas can appear anywhere and that transmission to naïve hosts may occur. In those countries where rates of TB have declined to low levels over several decades, many clinicians are not suspicious of these infections even when fairly classic presentations are seen. Complications of advanced pulmonary infection or of miliary spread of the infection may result in surgeons being confronted with clinical dilemmas that require a working knowledge of this formerly common disease.
Pathogenesis and Natural History
Mycobacterium tuberculosis is an aerobic, non-spore forming bacilli with obligate intracellular growth (Fig. 2) that is a pathogen primarily of human beings. It has a high cell-wall lipid content and thus is acid-fast positive. The ability to see the organism by acid-fast staining traditionally has been important because of its growth in culture is so slow as to impede diagnosis.

Electron micrograph of tubercle bacilli (original magnification 21,000×). (Obtained from the Public Health Imaging Library; ID 8437. Contributed by the Centers for Disease Control and Prevention/Dr. Ray Butler; Janice Carr.)
Transmission of the TB bacilli is by inhalation of droplet nuclei that are airborne from an infected human host [6]. A critical inoculum of the pathogen in a susceptible host is required for clinical infection. These droplet nuclei of TB resist the lung mucociliary clearance mechanisms. Inhaled TB bacilli undergo phagocytosis by pulmonary macrophages, but intracellular killing does not occur with the same efficiency seen with other inhaled pathogens. The failure of intracellular killing results in replication of the bacilli within the phagocyte.
In healthy hosts, 70%–90% of exposed individuals do not develop clinical infection. This likely is attributable to the small inoculum of exposure and a robust host. However, as many as 30% of exposures result in either latent or active TB infection. In latent infections, the patient develops a positive hypersensitivity skin test but not immediate clinical disease and is not infectious to others during this period. In latent infection, clinical TB develops within two years in about 50% of patients but may not emerge until many years later in the remainder. Active clinical pulmonary TB without treatment results in a 50% mortality rate within two years.
When acute pulmonary infection occurs, a cellular immune response can be recognized within two weeks and may be detectable in advance of clinical evidence of infection. Infection preferentially is identified in the apices of the lung but can be quite variable, with unilateral single lobe or bilateral lung involvement. When pulmonary infiltrates are apparent, the patient is infectious to others.
Pulmonary infection may be indolent and slowly progressive, or it may be rapidly aggressive. Cavitation within the lung parenchyma may evolve rapidly and result in severe hemoptysis that is acutely life-threatening. Cavitation with immune compromise may lead to secondary infections within the lung caused by Aspergillus fumigatus or other opportunistic pulmonary pathogens [7].
Aggressive pulmonary infections may results in macrophage transport of Mycobacterium tuberculosis to regional pulmonary lymph nodes with resultant huge hilar lymphadenopathy that is characterized histologically by formation of caseating granulomas.
Determinants of Infection and Risk Factors
Transmission does not occur with all exposures to infected tuberculosis patients. Like all infectious events, a larger inoculum of bacteria will increase the probability of infection. The local environment of the lung that has damaged architecture from tobacco exposure and chronic obstructive lung disease will be susceptible to infection by a smaller burden of micro-organisms. Although the frequency of infection may not be increased, there is no doubt that the severity of infection will be greater if the host is infected with multi-drug resistant (MDR) TB.
Impaired host responsiveness influences both the probability of transmission and the severity and progression of disease [8,9]. Patients with HIV infection represent especially vulnerable hosts for conventional TB infections but also for infection with atypical tuberculous organisms. A background of steroid therapy, various immunosuppressive agents used in organ transplantation, and advanced malignant disease increases the probability of TB infection. Chronic lung disease provides not only an enhanced local environment for lodgment of pathogens, but systemic hypoxemia to impair host responsiveness. Similarly, patients with chronic liver disease, chronic kidney dysfunction, diabetes mellitus, and protein–calorie malnutrition are especially susceptible hosts. Environmental issues of tobacco use, alcoholism, and overcrowded living conditions are associated with TB infection. The common theme in these risk factors is a suboptimal host. The more severe the suppression of host responsiveness, the greater the risk of extra-pulmonary spread of the infection.
Diagnosis
The diagnosis of TB requires a high index of suspicion. Patients with active clinical infection will have weight loss, poor appetite, fatigue, night sweats, and intermittent fever. Active pulmonary infections usually cause non-specific chest pain, a new-onset cough, and possibly hemoptysis. Chest roentgenograms usually are performed in suspected cases and will provide evidence that pulmonary TB may be present (Fig. 3). Because various fungal infections, small-cell carcinoma, and unusual presentations of bacterial pneumonia may have the appearance of TB on chest roentgenograms, additional diagnostic methods are necessary.
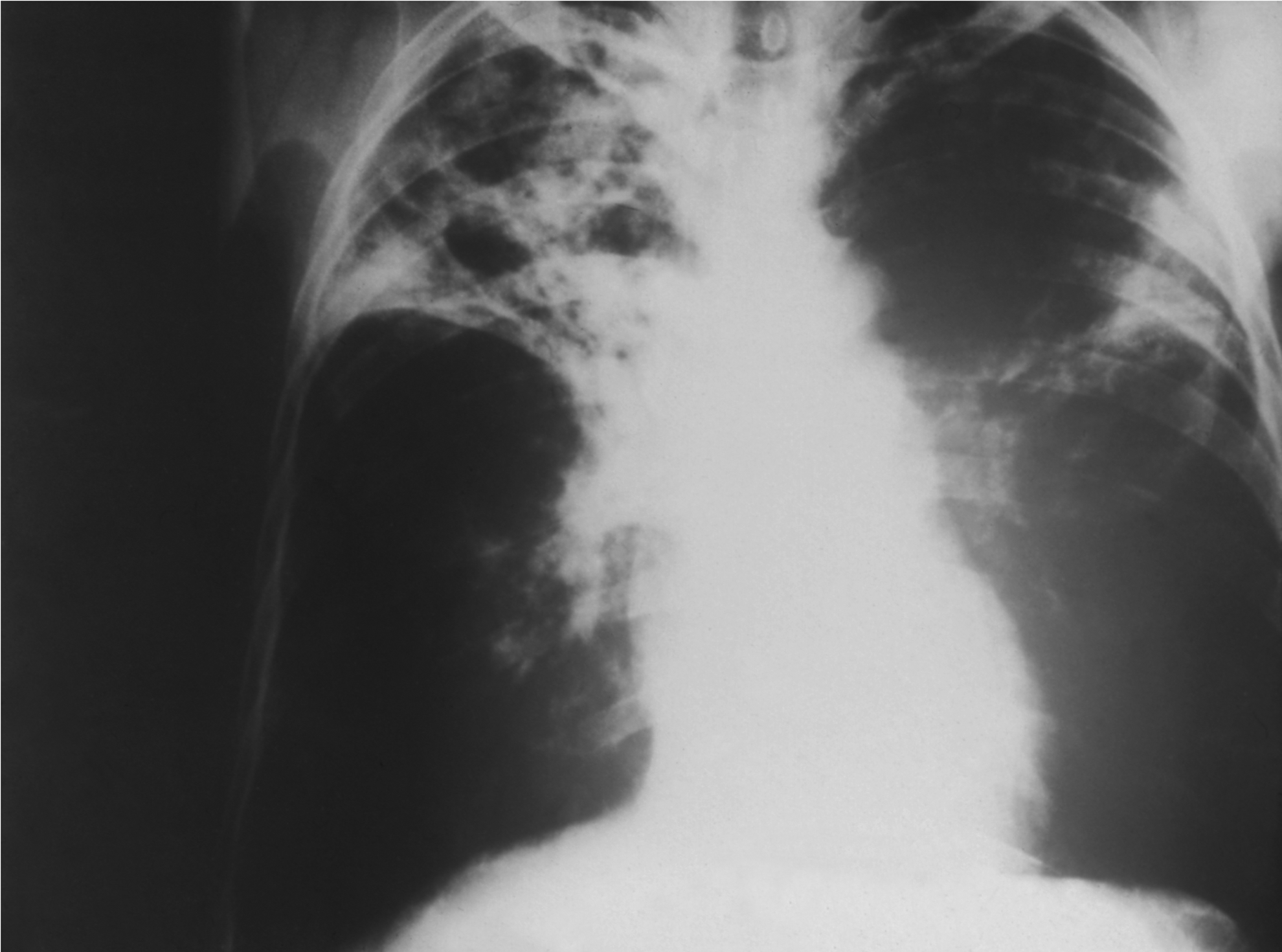
Chest roentgenogram of a patient with active pulmonary TB with far-advanced infection in the right apical area. (Obtained from the Public Health Imaging Library; ID 14804. Contributed by the Centers for Disease Control and Prevention.)
Skin testing remains the primary method for the diagnosis of latent TB [10]. The antigen is injected intradermally to create a wheal that is inspected at 48–72 h to observe the response of the host. A positive test is >5 mm in patients with HIV infection or other immunosuppressed hosts. A positive test is >10 mm in immigrants from high-prevalence countries, intravenous drug abusers, patients with chronic medical diseases, and children less than four years of age. In all others, >15 mm is considered a positive test.
Skin testing may reflect prior infection or may be equivocal, in which case, interferon-detection assays (QuantiFERON-TB Gold test) are employed [11]. This study is performed by incubation of a freshly heparinized blood specimen with a TB-specific antigen protein target, and this permits the recognition of interferon-gamma. The U.S. Centers for Disease Control and Prevention is recommending that interferon detection methods replace skin testing for the establishment of the diagnosis of TB [12].
Identification of the tubercle bacilli in the sputum and then culturing of the organism have been traditional diagnostic methods for TB. The acid-fast or Ziehl-Neelsen stain has been employed for the recognition of the organism. Traditional cultures have been employed for definitive documentation of infection and for the determination of microbial sensitivities. Culturing methods have been laborious and slow, so that DNA sequencing, line probe assays, reverse transcriptase–polymerase chain reaction (PCR) assays, and pyrosequencing are being explored for rapid detection and characterization of the susceptibility profiles of tuberculosis pathogens [13].
A nucleic acid amplification method that is receiving particular attention is the Xpert MTB/RIF assay (Cepheid, Sunnyvale, CA). This method uses molecular probes and PCR to identify M. tuberculosis and the resistance gene for rifampin. The study is performed on the clinical sputum specimen without processing and is technically easy. It is being deployed widely and has the promise of providing rapid detection and identification of extensively drug-resistant (XDR) strains [14,15].
Extra-Pulmonary Infection
This rapid proliferation of TB in lymph nodes in immunocompromised hosts can lead to miliary disease [16]. Erosion of lymph nodes into vascular structures is the common explanation for TB dissemination. Blood-borne organisms cause the diffuse millet-seed appearance in the lung tissue from blood-borne dissemination and result in “metastatic” lesions that are remote from the lung. Extra-pulmonary infection may simply be secondary to direct extension of the disease into adjacent tissues or tissue spaces. Surgical care is not common in extra-pulmonary TB but may be necessary for diagnosis of unusual pathologic lesions or for local complications of invasive TB at the site of dissemination. Extra-pulmonary TB can occur at virtually any anatomic site [17]. All of these sites of infection are associated with a greater mortality rate than is observed with pulmonary TB and require a sustained period of anti-tuberculosis therapy for recovery.
Pleural space, mediastinal, and pericardial infection are observed from local extension of the disease from tuberculous effusions or direct extension from the infected pulmonary parenchyma and lymphatic system. Thoracic operations may be required for either the rare patient with esophageal complications or a case of severe pleuropulmonary infection. Thoracic operations may be required if there has been rupture of pleuropulmonary disease into the pleural space or into a bronchus, bronchopleural fistula, bronchial obstruction secondary to enlarged lymph nodes, or acute hemorrhage from a cavitating lesion [18]. Decortication may still be required for large TB empyemas [19]. Thoracoplasty for reduction of the lung space that was a frequent part of the surgical management of tuberculosis in past decades is not often employed at present. Constrictive pericarditis may require pericardiectomy [20].
Head and neck infection is secondary to a lymphadenitis syndrome from extension of pulmonary infection via the lymphatics. Commonly known as scrofula, these infections usually are treated with anti-TB therapy but may require aspiration for diagnosis or local surgical debridement to excise a fistula or necrotic soft tissue. Occasionally, neck dissection is required [21].
Miliary dissemination is associated with central nervous system infection. Tuberculous meningitis can be an elusive diagnosis because of difficulty in culturing the pathogen, and a brain abscess may require surgical drainage [22]. Surgical decompression of the spinal cord may be necessary because of local extension of Pott's disease in the vertebral bodies [23]. Pott's disease is the most notable of the bone and joint infections from extra-pulmonary TB [24], but other skeletal structures may well be involved by miliary dissemination [25].
Genitourinary infection can be a pyelonephritis syndrome. Pyuria is identified, but identification of TB is elusive [26]. Perinephric abscess may require nephrectomy, and these abscess collections may extend into the retroperitoneum and along the iliopsoas muscles. In males, disseminated disease may result in prostatitis, seminal vesicle infection, or epididymitis [27]. Pelvic inflammatory disease originating from the fallopian tubes is observed in post-menopausal females [28].
Skin and soft tissue infections also may be observed with large cutaneous lesions. Abscesses may occur months after the miliary event [29]. Local drainage and excision of necrotic tissue may be warranted [30].
Intra-abdominal TB infection deserves special attention. Peritonitis is an infrequent complication of TB but one of which all abdominal surgeons must be aware (Fig. 4) [31]. Miliary spread of the tubercle bacilli results in seeding and growth of the pathogen in the peritoneal cavity. Like other forms of primary peritonitis, the presence of ascites and the use of ambulatory peritoneal dialysis are risks for the development of tuberculous peritonitis [32]. In the ambulatory peritoneal dialysis patient, external access to the catheter system by TB pathogens is considered another possible source of these infections in addition to blood-borne dissemination [33].
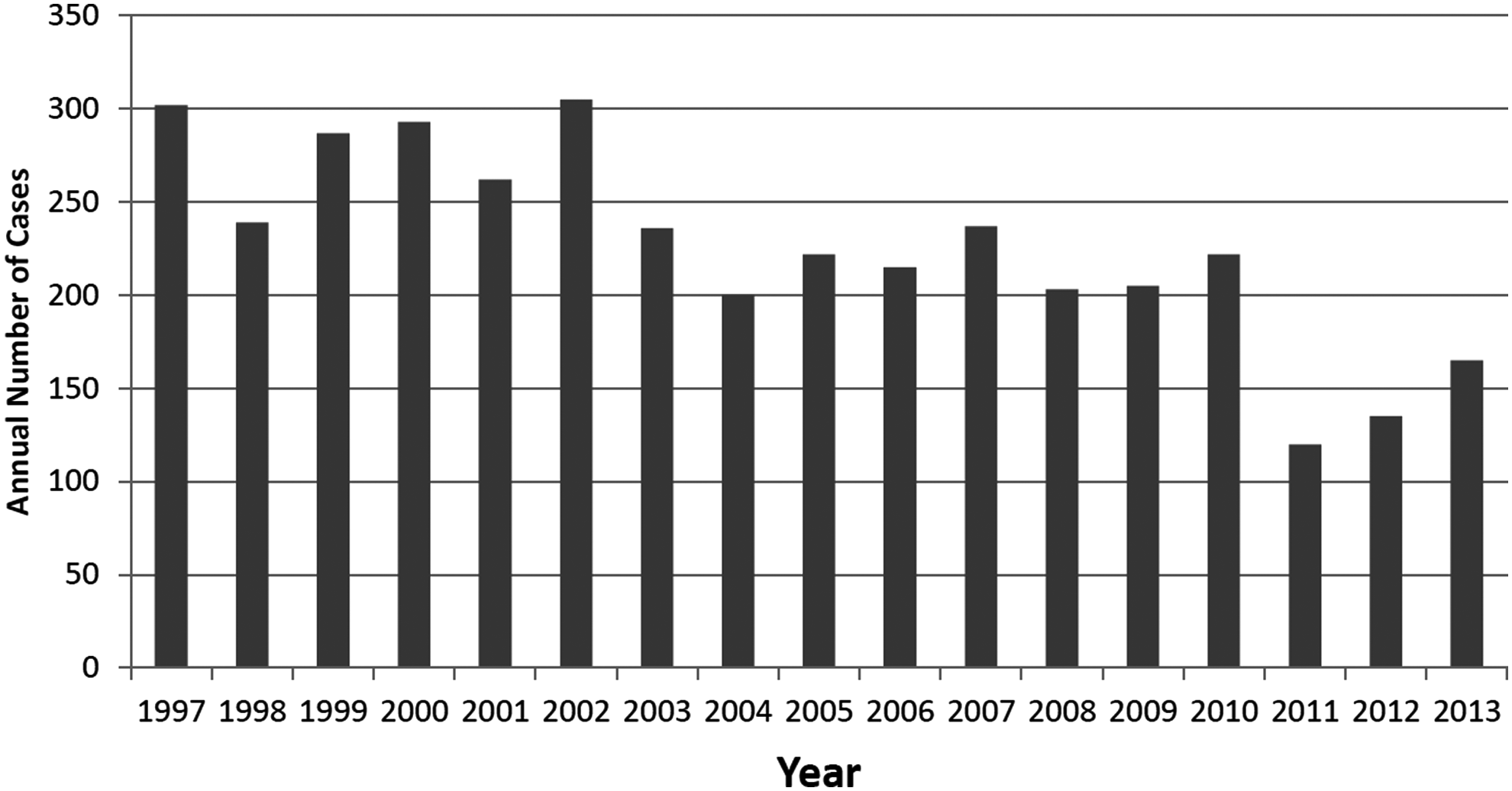
Estimates of the annual number of hospital admissions with tuberculous peritonitis (ICD-9 codes: 01400–01406) over the last 17 y in the U.S. Total U.S. hospitalizations have averaged 36–40 million/ y during this interval [4].
Tuberculous peritonitis has different manifestations [34]. “Plastic” TB peritonitis is characterized by a thickening of the peritoneal tissues and the omentum with cake-like mass formation being identified on abdominal computed tomography (CT) scanning. The masses constitute lymphadenopathy and fibrosis from the infection. “Serous” TB peritonitis is associated with free or loculated ascites and fibrous encasement of intra-abdominal structures. Peritoneal dialysis-associated peritonitis infections have highly variable findings but often are noted to be associated with abnormal enhancement of the mesentery or peritoneal lining with intravenous contrast on abdominal CT scans.
The diagnosis of TB peritonitis can be difficult unless it has been observed previously by the clinician who therefore recognizes it. Pleuropulmonary TB infection may or may not be present synchronously. The infection may be insidious, with limited clinical findings other than the inanition, commonly observed with disseminated TB, or it may present with acute pain and tenderness like bacterial peritonitis [35]. Abdominal CT scans are useful in establishing the diagnosis, but as indicated above, the imaging patterns can be variable. In patients with acute symptoms, the diagnosis often is made at laparotomy, with the characteristic findings of fibronodular studding of the omentum and parietal/visceral peritoneal surfaces. Tuberculous peritonitis is observed more often in females, and the clinical appearance is similar to that of disseminated ovarian carcinoma in the peritoneal cavity [36]. About 90% of cases will be associated with lymphocytic ascites [37]. Acid- fast stains are positive in only about 25% of cases, whereas adenosine deaminase determinations in the ascites fluid are positive in more than 80% [38]. Polymerase chain reaction of the ascites fluid is useful [39]. Biopsy of the fibronodular lesions will demonstrate caseating granulomas on histologic study. Cultures of the tissue will recover the pathogen, but culture of the ascites fluid has a poor yield. This is particularly significant because delays in obtaining culture results have been associated with greater mortality rates when effective anti-TB therapy is delayed [40].
Gastrointestinal infection occurs either from expectorated and swallowed pulmonary pathogens, which then migrate distally in the gut, from direct extension from lymph nodes or adjacent organ structures, or from hematogenous dissemination. The uncommon esophageal lesion may present with obstruction or bleeding and can be diagnosed endoscopically and managed by medical therapy only with complete resolution. Perforation or fistulization into the tracheobronchial tree will necessitate thoracotomy or video-assisted thoracoscopy for management of this highly morbid complication [41], although successful stent management of tuberculosis-associated esophageal perforation has been reported [42]. Intramural gastric tuberculomas may cause outlet obstructions, or ulcerations may present as gastric bleeding. The ileocecal area is the most commonly affected, where bleeding, obstruction, fistulization, or perforation may be observed. These diagnoses affecting the ileocecum or the colon may be confused with Crohn disease [43]. Anorectal TB infection may present as anal fissures, fistulas, or perirectal abscesses. These presentations must be differentiated from the more common clinical presentations of these anorectal conditions.
Medical Treatment
The treatment for culture-positive tuberculosis is multi-drug therapy: Anti-tuberculous drugs always are given in combinations and not as single agents. Patients with latent infection who are identified by a positive skin test or positive assay for interferon-gamma should be treated for three to nine months with isoniazid or rifampin or a combination of the two (Table 1) [44,45]. For clinically active disease in patients with susceptible organisms, various combinations of isoniazid, rifampin, pyrazinamide, ethambutol, and rifapentine are recommended (Table 2) [46]. The recommended dosing schedules for these drugs are detailed in Table 3. Compliance with drug regimens for both latent and active disease have been sufficiently problematic that directly observed therapy is commonly employed for regimens that are administered on a five d/wk regimen and requires second-party documentation that the drugs actually are taken. Directly observed therapy also has been recommended for once-weekly treatment for latent infection with isoniazid and rifapentine [46]. It is unclear whether this policy in such cases has improved the outcomes [47].
Use in directly observed therapy.
Reprinted from Centers for Disease Control and Prevention [43].
The treatment has an initial phase (8 weeks) and several continuous-phase options (18–31 wks). Reprinted from American Thoracic Society [45].
Directly observed therapy.
Numbers in parentheses are the maximum dose to be given.
Reprinted from American Thoracic Society [45].
Each of these drugs has potential toxicities that must be monitored during therapy. Isoniazid, which interferes with mycobacterial cell wall synthesis, requires monitoring of liver enzymes for idiosyncratic hepatic toxicity. It also is associated with dose-related peripheral neuropathy [48]. The rifamycin group of antibiotics (rifampin [49], rifapentine [50], and rifabutin [51]) inhibits the DNA-dependent RNA polymerase in the tubercle bacilli but not the similar mammalian enzyme. The rifamycins are associated with gastrointestinal, hepatic, hematologic, and central nervous system toxicities. Pyrazinamide has an undefined mechanism of action [52]. It is associated with dose-related hepatic toxicity and anemia. Ethambutol is an antimetabolite for TB bacilli that is associated with optic neuropathy and requires monitoring of patients for reduced visual acuity and the development of color blindness [53]. Drug therapy for clinically active disease is usually for eight weeks for the initial phase of treatment followed by a continuation phase of an additional 18–31 weeks. Longer courses of treatment commonly are employed for patients with cavitary pulmonary infection and for those with extra-pulmonary infection.
Monitoring of treatment requires monthly followup cultures until two are consecutively negative. Persistence of positive smears or positive cultures raises the issue of resistant pathogens or inadequate compliance with therapy. Because of the strong association with TB infection, all new cases should be tested for HIV infection.
A major issue in the treatment of patients with active tuberculosis is the emergence of MDR-TB [54], defined as resistance to both isoniazid and rifampin. Such organisms are responsible for more than 600,000 new cases and more than 150,000 deaths annually in the world. Greater death rates are observed in HIV-infected persons and those with immunosuppressive disorders. Patients with MDR-TB require treatment with second-line drug choices that are given in various combinations (Table 4). Strategies for using these agents in MDR-TB infections include the administration of at least four drugs by directly observed therapy throughout the entire course of treatment. Smears and cultures are performed monthly to monitor response. The initial phase of therapy lasts for at least six months and should include an injectable drug. The initial phase is continued for four months after smears and cultures have been negative. The total duration of drug therapy thus is 18–24 months [55].
Therapy requires the simultaneous use of multiple agents.
Reprinted from American Thoracic Society [45].
The problem of emerging resistance has extended into the second-line anti-TB drugs, producing XDR-TB. This is defined as pathogens resistant, not only to isoniazid and rifampin, but also to any fluoroquinolone and at least one of the injectable antibiotics (i.e., amikacin, kanamycin, or capreomycin). These infections have been treated with six-drug regimens that are directed by specific susceptibility testing for 24 months but have a mortality rate of 42% [56]. These organisms are believed to arise primarily from sub-therapeutic treatment of sensitive infections, with resistance being the consequence. Effective treatment of sensitive TB infections and early identification of these highly resistant infections are important for limiting the frequency of XDR-TB.
Surgical Treatment
Surgical therapy is infrequently employed in the management of the TB patient. Surgical interventions are indicated for establishing the diagnosis of extra-pulmonary disease and for the treatment of complications of extra-pulmonary or far-advanced pleuropulmonary infection. Published management of these complex cases is limited to case reports or small retrospective series of patients. Laparoscopy may be required to establish the diagnosis and obtain suitable tissue and ascites samples for culture (or PCR) in the patient suspected of having tuberculous peritonitis [57]. Care must be exercised in the creation, maintenance, and release of the pneumoperitoneum to minimize the risk of aerosolized peritoneal fluid.
Open laparotomy may be required in a few cases for establishment of the diagnosis of peritoneal or gastrointestinal tuberculosis. Gastric outlet obstruction, hemorrhage, or even perforation may occur in the stomach from organisms that have been ingested from the primary pulmonary infection and will require surgical intervention for resection or control of bleeding. Gastric lesions identified by CT scans or contrast studies in patients with active pulmonary TB may avoid operation by endoscopic evaluation and biopsy leading to effective drug therapy [58].
Intestinal or colonic bleeding, obstruction, perforation, abscess, or fistula formation also may require surgical intervention [59,60]. Surgical intervention may be required for management of intestinal obstruction secondary to adhesions and scarring from TB peritonitis, intestinal perforation by a tuberculoma, or a tuberculous abscess [61]. Hepatic and pancreatic lesions from TB can be observed without other evidence of intra-abdominal pathology [62,63]. Biopsy can confirm the diagnosis by the identification of caseating granuloma. No resection of hepatopancreatic tissue is warranted, as the disease is managed by drug therapy [64].
Occupational Risks
Rates of active TB are greater in healthcare workers than in the population in general [65]. Although the overall incidence of TB infection in the U.S. is lower than in past decades, it still poses a threat for occupational infection of surgeons and operating room personnel. This may be especially true when a laparotomy or any of the other operations for extrapulmonary TB is being performed without prior appreciation that infection exists. It is unclear whether open operation on a case of TB peritonitis or any of the other operations discussed here poses a risk of occupational transmission. There is concern that laparoscopic risks may be present from the aerosolization of ascitic fluid with the creation and decompression of the pneumoperitoneum. Exposed personnel should undergo either skin testing or interferon-detection assays. Empiric anti-TB therapy is not justified in the absence of documentation of latent or clinical infection [66].
Summary
Although the overall incidence of TB infection in the U.S. has declined steadily, the worldwide movement of people means that an infected patient can be seen for care at any time. Surgeons who serve high-risk populations of patients and those participating in international surgical relief programs should be especially sensitive to TB as a diagnosis in their patients and as posing a risk of occupational infection. Effective drug therapy is available for the treatment of these patients, but the emergence of MDR-TB and XDR-TB poses a continued threat to further control of these infections. Tuberculosis infection has many patterns of presentation and should not be forgotten.
Footnotes
Author Disclosure Statement
The author has no conflicts of interest with regard to this paper.