
Abstract
Abstract
Background:
There is still uncertainty regarding the use of prophylactic drainage in abdominal surgical procedures. This meta-review aimed to summarize systematic reviews and meta-analyses evaluating abdominal drain placement in patients undergoing abdominal procedures, with a focus on surgical site infection and death from infections.
Methods:
Systematic reviews and meta-analyses identified in MEDLINE, EMBASE, CINHAL, Cochrane Central Register of Controlled Trials, World Health Organization Regional Medical Databases, and African Index Medicus were reviewed.
Results:
Fifteen systematic reviews and meta-analyses concerning prophylactic abdominal drainage in abdominal operations were included in this analysis. The median score of methodologic quality was eight (6–10). The majority of meta-analyses found no benefits of prophylactic drainage in reducing surgical site infection, but no significant differences were identified. Three studies demonstrated a significant difference in favor of no drainage, with two regarding cholecystectomy and one on appendectomy (p < 0.05). The quality of evidence provided by each review was mainly low and very low.
Conclusions:
Most reviews fail to detect an increased incidence of surgical site infection in the setting of drainage placement but also fail to attribute any specific benefits to the presence of a drain in abdominal procedures.
S
The use of drainage devices after various operative procedures is still controversial, although it has a long history [4]. Prophylactic drain placement has been practiced widely, with the dictum of Lawson Tait, the 19th century British surgeon, “When in doubt, drain,” well known to all surgical trainees. The prophylactic placement of abdominal drains in abdominal operations is used widely either to detect early complications, such as postoperative hemorrhage or leakage, or to remove collections that might be toxic, such as bile, and could become infected.
Any foreign body, however, can promote inflammation at the surgical site and may increase the probability of SSI [5]. Some studies have questioned the benefit of routine drainage [6,7]. It is argued that drains might adversely affect surgical outcomes—e.g., affecting anastomotic healing by causing inflammation in the anastomotic area and in the abdominal surgical incision [8,9].
Several systematic reviews have investigated the effectiveness of prophylactic drainage in abdominal operations [10–24]. Despite these studies, there remains uncertainty about the evidence base for drain use. A critical appraisal and synthesis of systematic reviews and meta-analyses is required to ensure that decision-making is informed by the best available accumulated evidence.
A “meta-review” can appraise and synthesize the findings presented in individual systematic reviews and meta-analyses [25,26]. It uses a similar review process as the traditional systematic review, including comprehensive literature searches and quality assessment by two reviewers. The major difference, however, lies in the fact that it considers only results reported in systematic reviews and meta-analyses, rather than results from individual studies.
Our aim was to appraise and synthesize systematic reviews that have focused on the benefits or consequences of abdominal drainage placement. Hence, we conducted this meta-review to compare routine drainage with no drainage in abdominal procedures using SSIs and death from infections as the outcomes.
Methods
This study followed the recommendations for systematic reviews of healthcare interventions [27]. This meta-review was based on clearly defined inclusion criteria, a comprehensive search of the literature, an assessment of the methodologic quality of the eligible reviews, and a synthesis and critical appraisal of the evidence. In addition, this review was granted an exemption from requiring ethics approval by the Institutional Review Board Ethics Committee at Jinling Hospital.
Search strategy
We performed a comprehensive search in MEDLINE, EMBASE, CINAHL, Cochrane Central Register of Controlled Trials (CENTRAL), World Health Organization Regional Medical Databases, and African Index Medicus. The time period was set from January 1990 to February 2015. The search strategy for MEDLINE is presented in Table 1. The language of publication was restricted to English, Spanish, French, and Chinese. Further, the reference lists of the retrieved articles and review articles were searched manually for other relevant studies.
The main search strategy was developed for use in MEDLINE. This search strategy was adapted to suit other databases. Details about the search strategy in other databases can be obtained by contacting the corresponding author.
Study selection
Two authors (XW, NZK) independently screened the titles and abstracts and assessed the full texts of the potentially eligible abstracts for inclusion. Differences were resolved through discussion or consensus with a third author (JR). Systematic reviews and meta-analyses were included if they compared drainage and no drainage and reported SSIs as the outcomes after abdominal operations in populations of any age. Abdominal surgical procedures in this study included but were not limited to gastroduodenal resection, liver resection, biliary operations, pancreatectomy, and colorectal surgical procedures.
Systematic reviews were defined as reviews that had been prepared using a systematic approach, in an attempt to minimize biases and random errors, that was documented in the Materials and Methods section. Meta-analyses were defined as reviews that statistically combined the results of different primary studies to obtain an overall estimate of effects [27].
Outcomes
The outcomes of interest were SSI rates, death attributed to SSI, and the cost, if provided. Other outcomes in each systematic review and meta-analysis were all listed.
Data extraction and quality assessment
We designed standardized data collection forms, piloted and revised them, and extracted information on the bibliographic details of the review, the aims, participants, type of operation, type of surgical incisions, comparisons, outcomes, type and number of studies included, and the cost. The definitions of SSI considered in the systematic reviews were also listed. Two authors extracted the data, and one author cross-checked all extracted data. Differences were resolved through discussion. All data were extracted from the systematic reviews; we did not extract any data from individual study reports. No meta-analysis was performed.
The 11-item Assessment of Multiple Systematic Reviews (AMSTAR) instrument was used to assess the methodologic quality of the systematic reviews and is recommended for this purpose [28,29]. The quality of the evidence of the included reviews was further assessed according to the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach [30].
Results
Identification of eligible reviews
Our search of the electronic databases and reference lists identified a total of 2,313 unique citations, of which 2,144 were excluded based on titles and abstracts. The full text of 171 articles was examined in detail. After excluding 136 articles, 35 reviews met the inclusion criteria. Of those, systematic reviews or meta-analyses on orthopedic surgical procedures (n = 9), breast operations (n = 4), cesarean delivery (n = 2), thyroid operations (n = 2), vascular operations (n = 1), extremity surgical procedures (n = 1), and mixed-category surgical procedures (n = 1) were excluded. Finally, a total of 15 reviews addressed abdominal drain placement in abdominal operations and were included in the analysis (Fig. 1).
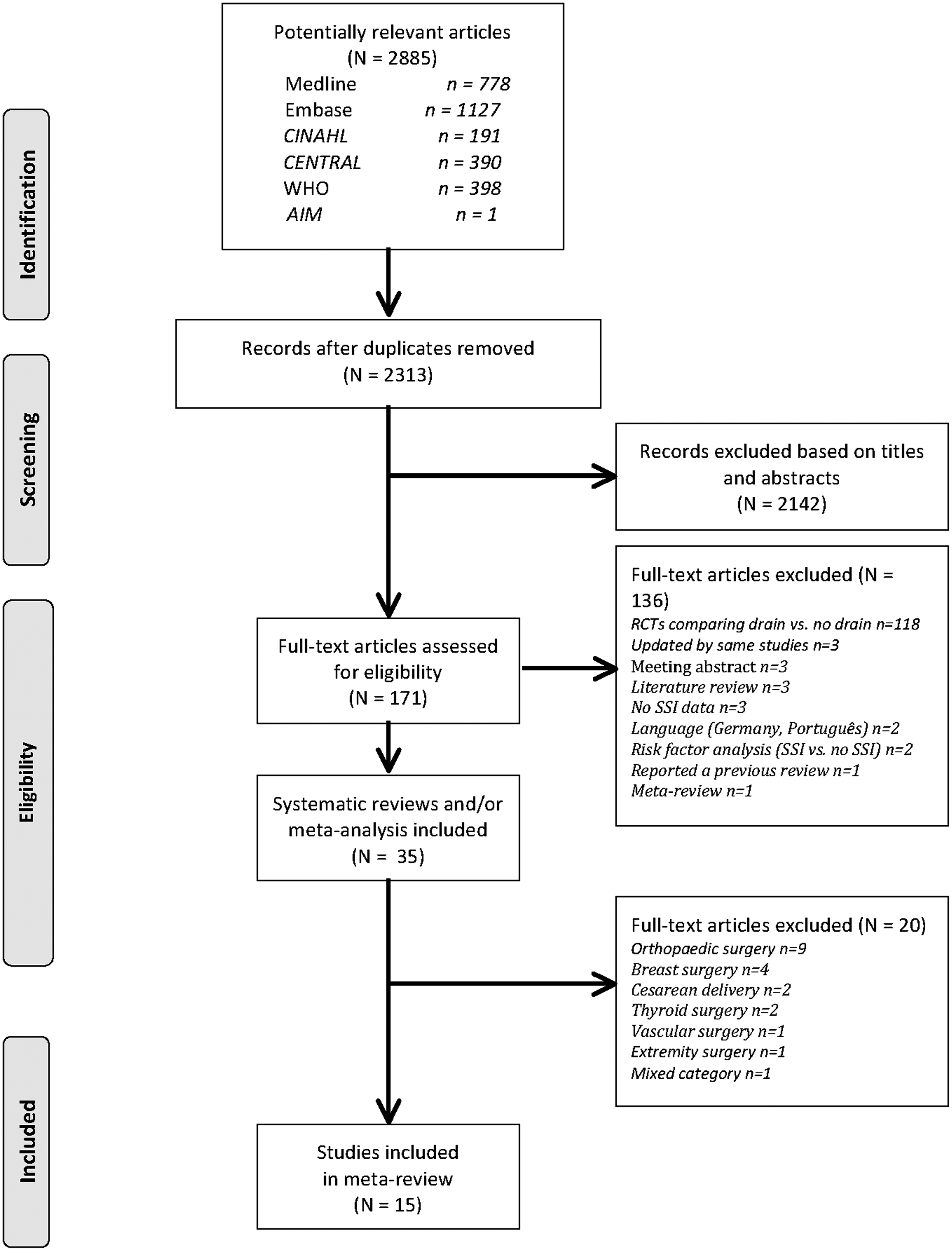
Study selection process. RCT = randomized controlled trial; SSI = surgical site infection.
Characteristics of reviews
A total of 90 primary studies (range 2–17 per review) had been included in the reviews. The 15 included reviews were published from 1999 to 2015; the median year of publication was 2011. All reviews reported on SSI, and the total number of study participants ranged from 278 to 3,090 patients. There were 12 reviews that reported in addition on overall death occurrence [11–15,18–22,24], but none of them provided information on death from SSI. Little evidence was found on the cost of drain insertion. Cholecystectomy [10,11,15,19] and colorectal operations [13,16,20,22] were the most common surgical procedures analyzed, followed by gastrectomy (n = 3) [18,23,24], appendectomy (n = 2) [12,17], liver resection (n = 1) [14], and pancreatic resection (n = 1) [21].
Most reviews exclusively focused on randomized controlled trials (RCTs) or quasi-RCTs, with the exception of two reviews that also included non-RCTs [20,21]. A detailed description of the 15 reviews, with the aims (specific participants), operative procedure(s), search strategy, primary and secondary outcomes, type and number of studies included, and number of participants enrolled, is given in Table 2.
SSI = surgical site infection; RCT = randomized controlled trial; CENTRAL = Cochrane Central Register of Controlled Trials; SCI-E = Science Citation Index Expanded; CBM = Chinese Biomedical Literature Database; LILACS = Literatura Latino Americana em Ciências da Saúde; CNKI = Chinese National Knowledge Infrastructure; SCI = Science Citation Index.
Quality of systematic reviews
The methodologic and reporting quality of the reviews varied widely (Fig. 2). The median number of AMSTAR criteria met was 8 (range 6–10). Ten (66.7%) reviews defined a priori research questions and inclusion criteria, 14 (93.3%) used duplicate study selection and data extraction, 12 (80.0%) performed a comprehensive literature search, two (13.3%) searched for grey or non-English literature, nine (60.0%) provided a list of the included and excluded studies, and 14 (93.3%) described the characteristics of the included studies. All studies assessed and documented their quality, used the data on the quality of the primary studies appropriately when formulating conclusions, used appropriate statistical methods, and assessed publication bias. There were no reviews that considered potential conflicts of interest.
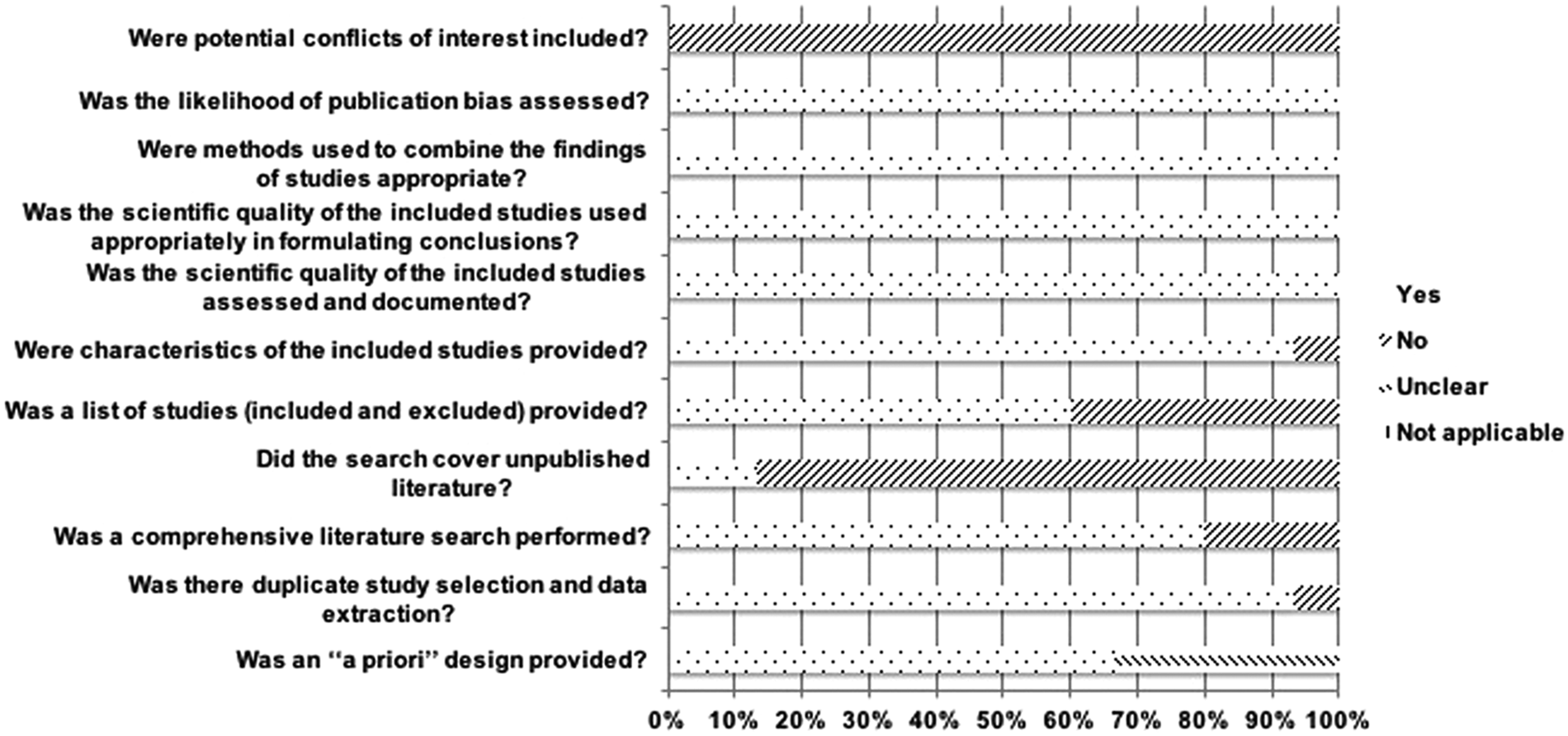
Proportion of systematic reviews that addressed each of the methodologic quality items of the AMSTAR tool.
Outcomes
All included systematic reviews used SSIs as one of the examined outcomes, but not all of them clarified whether they considered incisional SSIs only (superficial and deep SSIs) or all SSIs, which would include organ-space SSI. Cheng et al [12] clearly demonstrated that superficial and deep incisional SSIs, rather than all three types of SSI, were the outcome assessed in their review. Their definitions of incisional SSI were determined according to the Centers for Disease Control and Prevention criteria [31]. Jesus et al. [13] defined SSI as a discharge of pus from the abdominal surgical incision within 30 d after operation. The remaining reviews accepted the definitions of SSI that were reported by each individual study, with the understanding that there may be differences in these definitions between studies. Other assessed outcome variables included overall death, hematoma, seroma, fluid collection, hospital stay, pain, anastomotic leakage, and the cost (Table 2).
The effects of postoperative drainage found in the 15 systematic reviews and meta-analyses are summarized in Table 3, along with the types of operation and types of surgical incisions. Most meta-analyses (12/15) showed no significant differences in the occurrence of SSI, regardless of whether prophylactic drains were inserted or not. Three meta-analyses on the specific procedure type, however, demonstrated a significant difference in favor of no drain (p < 0.05), with two investigating cholecystectomy [15,19] and one investigating appendectomy for severe appendicitis [17]. The type of surgical incision varied from clean-contaminated surgical incisions in two elective non-complicated cholecystectomies [15,19] to contaminated wounds in one appendectomy after severe appendicitis [17].
CI = confidence interval; GRADE = Grading of Recommendations Assessment, Development and Evaluation; OR = odds ratio; RR = risk ratio.
Regarding outcomes other than SSIs, drain placement was found further to substantially delay hospital discharge [12,17,18,24], increase postoperative pain [10,19], and aggravate postoperative intestinal adhesion [17]. The primary outcome, SSI, in each review is described below according to anatomic location.
Cholecystectomy
In a Cochrane review by Gurusamy et al [15], no drainage after open cholecystectomy was found to lower the rates of SSI significantly in the main analysis (odds ratio [OR], 0.61; 95% confidence interval [CI], 0.43 to 0.87; p = 0.0061) [15]. For the sub-group analyses—e.g., no drain versus suction drain or passive drain, despite the fact that many of the studies did not reveal a statistically significant difference—the SSI rates continued to remain lower in the no drain group than in the drain group.
The results of three reviews on laparoscopic cholecystectomy varied [10,11,19]. A non-significant correlation was found between drain placement and infection rates in the reviews of Antoniou et al [10] and Bugiantella et al [11] on elective uncomplicated laparoscopic cholecystectomy, which included five and four RCTs, respectively. A review by Picchio et al [19] was an update of the two reviews above. It included nine RCTs and covered almost all primary studies analyzed in the above two reviews. A meta-analysis by Picchio et al. [19] showed that the SSI rate was significantly greater in the drain group (OR, 2.35; 95% CI, 1.22–4.51; p = 0.01) after elective uncomplicated laparoscopic cholecystectomy.
Appendectomy
Two systematic reviews regarding severe or complicated appendicitis were included in this review, but their results differed completely. Li et al [17] reported that there were significant differences between drainage and non-drainage in the incidence of SSI based on a meta-analysis of 15 RCTs and quasi-RCTs (p < 0.0001). The quality assessment of the included trials showed that all primary studies were of low quality. Moreover, there was significant heterogeneity between studies (I2 = 5 4%, p = 0.007).
Another Cochrane review by Cheng et al [12] included four trials and concluded that there were no significant differences between drain use and lack of drain use in the rates of SSI. All trials were reported to have a high risk of bias. Taken together, these two systematic reviews showed the lack of effectiveness of abdominal drainage in preventing SSI after complicated appendicitis.
Other abdominal procedures
The other systematic reviews and meta-analyses showed that the routine use of abdominal drains was not beneficial for SSI prevention in patients undergoing colorectal surgical procedures [13,16,20,22], gastrectomy [18,23,24], liver resection [14], or pancreatic resection [21].
Quality of the included evidence
To classify the direction and strength of the conclusions, we rated the quality of evidence from the studies with clear results by GRADE. Most studies only included RCTs, which would suggest that their quality of evidence started high. Two systematic reviews, however, included both RCTs and non-RCTs [20,21]: A total of three retrospective studies compared the outcomes between a drain group and a no drain group. For one individual study discussing operative drainage after pancreatic resection, the surgeons were categorized according to their operative drainage practices into routine drainers (operative drains placed >95% of cases), selective drainers (drains placed ∼50% of cases), and routine non-drainers (drains placed <15% of the time) [32].
In a retrospective cohort study conducted by Fisher et al [33], the patients underwent different clinical practices in separate periods. During Period I (2004–2009), drains were routinely placed at the time of pancreatic resection, whereas in Period II (2009–2010), intraperitoneal drainage was not routinely placed for all patients requiring resection.
The third retrospective study categorized the patients in the operating room before the operation according to the surgeons' choice [34]. In this way, the classification of patients between the two groups (drainage vs. no drainage) in all three non-RCTs was designed to not mislead the results and conclusions. The selection bias was minimized in the above three retrospective cohort studies.
Four of the 15 reviews could not evaluate the quality of their evidence because of the lack of description of the quality of each individual study [16,20–22]. The other systematic reviews included only RCTs, and their quality of evidence ranged from moderate to very low. The reviews by Gurusamy et al [15] and Li et al [17] were identified as moderate quality because of a serious risk of bias. Five reviews were downgraded to low because of serious imprecision [10,11,13,14,19]. Evidence from three other meta-analyses was downgraded to very low because of both a serious risk of bias and serious imprecision [18,23,24]. Most studies included in these reviews had an unclear or high risk of random sequence generation, allocation concealment, blinding, and incomplete outcomes.
Discussion
In this meta-review of systematic reviews and meta-analyses, we identified 15 high-quality reviews comparing drainage with no drainage in patients undergoing abdominal surgical procedures. The review showed that the routine use of abdominal drains after abdominal operations did not benefit the patient in any way, although most of them did not report significant differences in SSI outcomes. Moreover, in participants undergoing open-laparoscopic cholecystectomy and appendectomy for complicated appendicitis, drain placement significantly increased the rates of SSI.
Drains are commonly placed in the operative setting to prevent abscesses, hematoma formation, and post-operative leakage [35]. The widespread application of drainage as a standard practice has been examined, however, given concerns about the potentially increased incidences of SSIs, pulmonary complications, and post-operative pain. Accordingly, this meta-review evaluated the necessity and safety of this practice, especially focusing on the association between drain usage and SSI.
In accordance with the multi-disciplinary review of Reiffel et al [36], no studies attributed a decrease in the incidence of SSI (including organ/space SSI) to drain placement. Drain-associated complications such as post-operative pain, foreign-body reactions, and enterocutaneous fistula require concern, however. As for how drains might lead to adverse outcomes, the physical disruption caused by the negative pressure may be causative [37]. Moreover, external or luminal contamination and subsequent retrograde bacterial migration along the drain surface could also lead to SSI [38].
A high methodologic quality is a pre-requisite for the valid interpretation and application of review findings. The AMSTAR is reported to be a reliable and valid measurement tool to assess the methodologic quality of systematic reviews [28]. In this review of systematic reviews and meta-analyses, the methodologic and reporting quality of the included studies had high scores when evaluated by AMSTAR criteria. The quality of evidence provided by each review, however, was mainly low and very low, although most studies only included RCTs or quasi-RCTs. The downgrading of evidence in each systematic review was from mainly serious risks of bias and imprecision.
Several limitations of this review should be acknowledged. First, most of the systematic reviews included, with the exception of one, did not clarify whether SSI pertained to the incision (superficial and deep SSIs) only or all SSIs including organ-space SSIs [12]. The disadvantages of prophylactic drainage are clearer with respect to organ-space SSIs compared with incisional SSIs [39]. Second, a meta-analysis pooling data from all systematic reviews and meta-analyses was not performed to compare drainage and non-drainage. Third, we graded the quality of evidence according to each review's descriptions, rather than those of the primary studies. Further, because of the language restrictions, two systematic reviews, one in Portuguese [40] and one in German [41], were excluded. All these limitations may make this meta-review insufficiently reliable, and thus controversy still exists regarding whether to place abdominal drains prophylactically.
Clinically, the main goal of using drains is to detect early complications after abdominal operations, such as hemorrhage or anastomotic leak. Various studies on the use of drains after abdominal operations failed to show any difference between patients receiving drains and those who did not; however, three studies on cholecystectomy and appendectomy showed a significant correlation between drain placement and increased SSI rates.
With the development of medical technology, more and more minimally invasive or non-invasive methods to detect early post-operative complications are being applied. This may further make the prophylactic placement of drains after abdominal surgical procedures unnecessary.
Conclusions
On the basis of the present data, studies evaluating the risk of SSI associated with routine drain placement have yielded conflicting results. Most reviews fail to detect an increased incidence of SSIs in the context of drainage placement, but they also fail to attribute any specific benefit to the presence of a drain during the abdominal procedures. Future well-designed studies on abdominal drainage should provide a detailed description of the interventions and examine SSIs to ensure that they can be used by systematic reviews and meta-reviews to identify the value of drains in surgical procedures.
Footnotes
Acknowledgment
The work was supported by grants from the National Natural Science Foundation of China (81270478).
Author Disclosure Statement
No competing financial interests exist.