
Abstract
Abstract
Background:
Surgical site infections (SSI) remain a significant problem to both the patients and the healthcare system. Value care and standardized quality measures continue to promote improvement in surgical asepsis, but certain debates remain unresolved in the field of surgical hand antisepsis.
Methods:
Review of relevant accounts and literature.
Results:
Controversy has existed regarding the U.S. Food and Drug Administration (FDA)'s 1994 Tentative Final Monograph (TFM), which defined how surgical hand antisepsis products are assessed. Issues involving neutralizers and demonstration of a cumulative effect were addressed in the FDA's Proposed Rule in 2015. Few studies have used SSI as a primary outcome and instead have used a surrogate marker (colony-forming units [CFU]). Quantitative microbiology studies suggest a minimum bacterial inoculum of 105–107 CFU/mL is necessary to cause a clinical infection. Outcomes of antisepsis likely are driven by both active ingredient(s) and overall product formulation. Povidone–iodine aqueous scrubs are inferior to chlorhexidine gluconate (CHG) 4% aqueous scrubs and alcohol-based rubs (ABR). The SSI and CFU outcomes studies support the equivalence or superiority of ABR over CHG.
Conclusions:
Both ABRs and CHG 4% are preferred to povidone–iodine for surgical hand antisepsis. Well-powered randomized controlled trials measuring SSI as a primary outcome, as well as those designed according to either TFM or European methodology, with appropriate controls and neutralizers, are warranted. These trials should incorporate different ABR formulations and CHG 4%, as well as skin tolerance assessments and a cost analysis.
H
Scope and Background
Approximately 16 million surgical procedures are performed in the U.S. annually [6,7]. From 2006–2008, the National Healthcare Safety Network identified the overall risk of SSI at the primary incision site as 1.9% (range 0.26%–13.83%), with earlier studies estimating 2%–5% [8.9]. A multi-state point-prevalence survey estimated for 2011 that 4.0% of patients had at least one healthcare-associated infection (HAI); SSIs and pneumonia (both 21.8%) were the most common non-device-related infections [10]. Surgical site infections carry as much as an 11-fold higher risk of death. Importantly, an estimated 60% of SSIs are deemed preventable if evidence-based guidelines are followed [9,11]. It has been estimated that SSIs and other HAIs increase length of stay up to 2.5-fold at a cost nearly three times higher than non-infected patients [12,13]. Lastly, annual SSI healthcare expenditures may reach $10 billion [9].
Surgical site infections are classified as superficial incisional, deep incisional, or organ/space, as defined by the U.S. Centers for Disease Control and Prevention (CDC)'s National Nosocomial Infections Surveillance system [4,14]. Superficial and deep incisional SSIs (two-thirds of all SSIs) are likely caused by the transfer of skin flora into the surgical site from either the patient or surgical personnel [4]. By contrast, the cause of organ/space SSIs is more likely entry into a contaminated body cavity or a delayed consequence of poor surgical technique. The focus of surgical hand antisepsis therefore is the prevention of superficial and deep incisional SSIs.
Role of Surgical Hand Antisepsis in Preventing SSI
The 19th century ushered in an era of microbiology, led by Louis Pasteur and Robert Koch; aseptic surgery and steam sterilization, led by Ernst von Bergmann; and surgical hand antisepsis, led by Ignaz Semmelweis and Joseph Lister. Semmelweis, a Hungarian obstetrician, demonstrated a reduction in maternal death from puerperal sepsis with the use of chlorinated hand wash; and Lister, an English surgeon, later introduced dilute carbolic acid solution for the same purpose [15–17]. Surgical gloves, developed by William Halsted, followed [18]. Despite further product development over more than a century since these pioneering efforts, SSIs persist.
The most recent CDC guidelines for prevention of SSIs, published in 1999, recommend that surgical hand antiseptic agents display a broad spectrum of activity, be fast acting, and have a persistent effect [4]. The elimination and reduction of transient and resident skin flora, respectively, should occur immediately; thereafter, persistent or residual activity combats proliferation of microorganisms on the gloved hand [19,20]. Both immediate and residual activity limit the consequences of breaks in aseptic technique (e.g., glove perforations), which occur in more than 30% of procedures and increase with the duration of surgery [18,21–23]. As an example, a single surgeon performing unconventional surgical hand antisepsis caused an outbreak of Staphylococcus epidermidis incision infections and endocarditis when the surgeon's colonized hands suffered breaches in aseptic technique [24]. Following the restoration of proper surgical hand antisepsis, with the daily use of a chlorhexidine (CHG)-containing surgical scrub for two weeks, the pathogen was eradicated; no subsequent infections with the same bacterial strain occurred. Additionally, Misteli et al. observed among patients not receiving surgical antimicrobial prophylaxis a higher adjusted odds of developing an SSI (odds ratio [OR] 4.2; 95% confidence interval [CI] 1.7–10.8) with glove perforation compared with cases when asepsis was not breached [22]. With the established benefit of surgical hand antisepsis, various product-types and protocols exist.
Surgical Hand Antisepsis Testing and Product Options
In the United States, an over-the-counter (OTC) drug is covered by the OTC Drug Review if its conditions of use (e.g., active ingredient, dosage form and strength, route of administration, and specific use/indication) existed in the OTC marketplace on or before May 11, 1972 [25]. Ineligible drugs otherwise require approval through the New Drug Application (NDA) process. The U.S. Food and Drug Administration (FDA) established an Advance Notice of Proposed Rulemaking or Monograph for OTC Topical Antiseptic Drug Products in 1974 and for Alcohol Drug Products for Topical Antimicrobial Use in 1982 [26]. Prior to this, an Advisory Review Panel of non-FDA scientific experts performed an initial review that categorized drugs as either Generally Recognized as Safe and Effective (GRAS/E) and not misbranded (category I), not GRAS/E or misbranded (category II), or indeterminate because of insufficient information (category III) [26].
In 1978, a Tentative Final Monograph (TFM) for OTC Topical Antimicrobial Drug Products was published and was amended once in 1991 to establish a Monograph for First Aid Antiseptic Products and again in 1994 to establish a Monograph for OTC Healthcare Antiseptic Drug Products [27]. A Proposed Rule in 2013 amended the 1994 TFM calling for additional safety and effectiveness data for active ingredients in consumer antiseptic washes. Lastly, a Proposed Rule was issued May 1, 2015, to establish conditions under which OTC antiseptic products for use by healthcare professionals are GRAS/E [25]. This rule says that additional safety data, incorporating in vitro data and in vivo clinical simulation, are required before a final determination can be made. Also, productive effectiveness standards, as measured by log10 reduction standards, were revised on the basis of the March 2005 Nonprescription Drugs Advisory Committee (NDAC) meeting and comments following the 1994 TFM (see Criticisms of the 1994 TFM below). Pertinent to this review, the new Proposed Rule states that ethyl alcohol (EA) 60%–95%, isopropyl alcohol (IPA) 70%–91.3%, and povidone–iodine (PVP-I) 5%–10% are eligible for OTC drug review, whereas CHG 4% is not. Furthermore, all three eligible drugs will be re-categorized as IIISE for safety (S) and efficacy (E); prior categorizations from the 1994 TFM were I, IIIE, and I, respectively.
Until a Final Rule is set forth, the most up-to-date TFM remains in effect; however, most evidence was guided by the 1994 TFM. This document states that the testing procedure to be used is a modification of the American Society for Testing and Materials (ASTM) Standard Method for Evaluation of Surgical Hand Scrub Formulation, Designation E-1115, published in 1986 [28]. Of note, ASTM International (formerly the American Society for Testing and Materials) in the United States and Canada, and the European Committee for Standardisation in Europe, outline in vivo test methods for surgical hand antiseptics.
The TFM methodology requires bacterial log10 reduction standards as a means of measuring immediate, residual (persistent or substantive), and cumulative activity in order to regulate product effectiveness. The test subjects first undergo a period of two weeks when they abstain from using antimicrobial agents followed by a one-week baseline period. Subjects exhibiting a minimum baseline hand population of 1.5 × 105 organisms are eligible. Next, subjects apply the product over the course of five days, applying once on days 1 and 5 and three times on days 2, 3, and 4 with at least a one-hour interval between applications. The following thresholds are requisite: A single log10 reduction of bacteria on each hand within one minute of application; the bacterial cell count on each hand should not exceed the baseline within six hours on the first day, a two-log10 reduction of bacteria on each hand within one minute of use after the first wash on the second day, and a three-log10 reduction of bacteria on each hand within one minute of use by the end of the fifth day (Note: The Proposed Rule from 2015 requires only a two-log10 reduction of bacteria on each hand within one minute after a single application, and the bacterial cell count on each hand should not exceed the baseline value at six hours).
The glove juice method is employed for bacterial sampling whereby a sampling solution is aseptically added to the glove and hand to be sampled. The glove is fastened securely above the wrist, and all surfaces of the hand, including the subungual areas and interdigital spaces, are uniformly massaged for one minute. A measured volume of the fluid is then retrieved aseptically in preparation for bacterial enumeration, and the log10 reduction is calculated using the established baseline.
The majority of currently marketed antiseptic products for pre-operative hand and forearm application comply with the 1994 TFM, although this is not required by the regulations. This is because enforcement of product compliance with the described methodology will follow the establishment of a Final Rule. Surgical hand antisepsis products reviewed through the NDA or abbreviated NDA (ANDA) process, as well as those associated with previously established (A)NDAs, or which are otherwise marketed, are presented in Fig. 1. Included is information regarding the method and duration of application for each product.
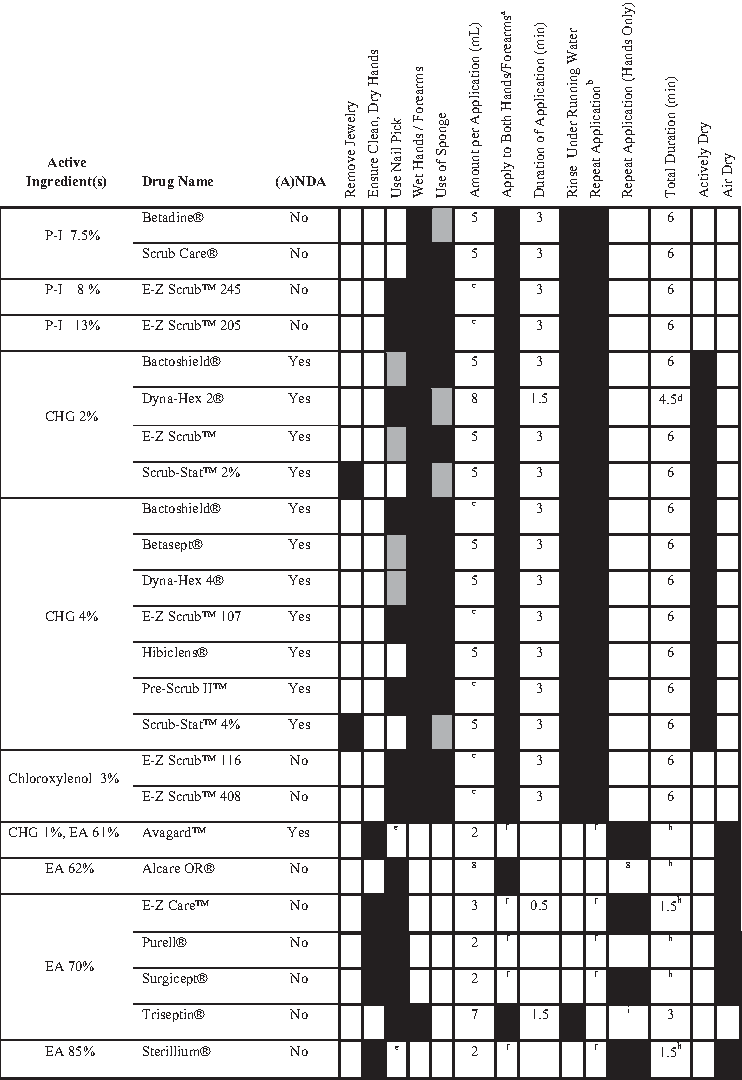
Surgical hand antisepsis product application per manufacturer's instructions.
Criticisms of the 1994 TFM
In response to the 1994 TFM criteria, the Soap and Detergent Association, together with the Cosmetic, Toiletry, and Fragrance Association, formed a coalition that proposed the Health Care Continuum Model—a model for the classification of topical antiseptics that hosts lower bacterial log10 reduction criteria. The Coalition called the TFM criteria overly stringent and commented that demonstration of a persistent or cumulative effect is not applicable for alcohol-based products, as alcohol is not a persistent antimicrobial ingredient [29]. Any prolonged effect induced by alcohol is likely the result of an initial sub-lethal insult to some bacteria, which is unrecoverable after donning a surgical glove [30]. The need for demonstration of a cumulative effect on day 5 also has been challenged by arguing that a product's performance on a Monday should be equal to its performance on a Friday [31,32]. The concept that a product must reduce microorganism counts more on Friday than it was able to do on Monday would seem disadvantageous for the Monday patient. Furthermore, the 1994 TFM cumulative benchmark implies that an individual would scrub 11 times over five days to achieve the required effect, but in a clinical context, how does this relate to an individual with a less robust surgical schedule [33]? In Europe, in vivo testing described by EN-12791 does not require a cumulative test but rather compares the test agent with a reference surgical rub, n-propanol, immediately and after three hours under gloved hands [34].
On November 5, 2004, the FDA's Division of Over-The-Counter Drug Products reviewed literature submitted by the Coalition in a citizen petition arguing that the TFM proposed effectiveness criteria warranted revision. However, the reviewer found no strong evidence among the 84 references (81% were abstracts or technical reports or used a non-standard method for surgical scrub) by the Coalition on the following active ingredients: CHG 2% and 4%, EA, and PVP-I [35]. More specifically, the ASTM (16%) and TFM (n = 2) methods were seldom reported, and these studies were deficient or deviated from standard methods. The NDAC met early in 2005 and agreed that insufficient evidence existed at that time to justify alteration of the 1994 TFM efficacy standards [27].
Additional criticism has been voiced regarding the misuse or neglect of neutralizing agents, which stop test solution activity in sampling fluid, diluent, or growth media. The 1994 TFM dictates that the sampling solution used after the final wash should contain an antimicrobial inactivator (neutralizer) specific to the test formulation [28]. It adds, however, that there is no final recommendation about whether an inactivator should be added to the sampling solution prior to the final wash, as this might skew bacterial counts higher on subsequent washes if residual neutralizer remains. Of similar concern is whether prompt processing of samples is sufficient to avoid falsely reduced bacterial counts secondary to the continued action of the test formulation. Over several decades, it has been argued that neutralizers should be incorporated in all sampling steps to assess the activity of the test solution more accurately under the specific conditions [36,37]. Kampf et al. in 2005 demonstrated in a cross-over trial that the absence of neutralizing agents can lead to a falsely greater reduction in test bacteria [38]. This was again observed using modified 1994 TFM methodology, when a higher degree of bacterial log10 reduction was observed in the absence of sampling fluid neutralization (diluent only) compared to when both sampling and diluent fluids were neutralized [39]. Of note, both the 2011 update of ASTM E-1115 and methodology described in the FDA's Proposed Rule from 2015 include the use of neutralizers in the sampling fluid [25,40].
Current Guidelines
Surgical hand antisepsis guidelines are widely published without uniformity (Table 1) [4,9,19,20,41–49]. This is, in part, attributable to the multitude of variables associated with surgical hand antisepsis: A pre-antisepsis hand wash; use of brushes, sponges, or nail picks; antiseptic agent selection; duration of scrubbing or rubbing; and differences between initial and subsequent applications. It also can be attributable to a lack of conclusive clinical trials.
There are still critical and largely unanswered questions. Does a reduction in CFUs, in accordance with regulatory standards, translate into reduced SSIs? What is the threshold below which CFUs need to be reduced to translate into a clinical effect? What is the product and protocol most adept at achieving this threshold?
Approaching the Critical Questions
Colony-forming units
A review of quantitative bacteriology by Krizek and Robson in 1975 commented that because all incisions are contaminated with bacteria, progression to infection is a result of the initial inoculum of bacteria defeating systemic and local defenses [50]. Those authors commented on several studies involving acute wounds, delayed incision closure, or clinical skin grafting in human beings, which all resulted in poor site outcomes when more than 105 bacteria/g were present at the time of intervention. Nearly 20 years earlier, Elek and Conen provided data detailing the minimum pus-forming dose for virulent staphylococci in human volunteers [51]. This study was the first to correlate the size of an inoculum with a clinical infection in human beings. The authors estimated 2–8 × 106 organisms were required and said that the mode of inoculation, strain origin (e.g., lesions, healthy volunteers, epidemic strains), presence of excess staphylococcal toxin, mucin, human plasma or starch, or age of the organism did not alter the minimum pus-forming dose. The presence of a foreign body (e.g., suture) did, however, result in a lower minimum pus-forming dose. More recent literature says that an inoculum of at least 10 × 106 CFU/mL was found in more than 75% of culture-positive specimens (average 2 × 108 CFU/mL) obtained from pus and infected peritoneal fluid [52]. Additionally, 76% of culture-positive samples from this study were polymicrobial, averaging 3.1 species for intra-abdominal infections and 1.9 species for soft tissue infections from 56 and 21 bacterial isolates, respectively. This evidence may help to link experiments driven by mean log reduction of CFUs on the hands with the clinical outcome of SSIs.
Product selection
Although the data presented suggest a correlation between quantitative bacteriology and clinical infection, a definite threshold remains unclear. Furthermore, this lack of evidence makes product selection even more difficult for the user and is also why governing bodies and societies have difficulty recommending one product or product type over another. The preponderance of scientific evidence in this field has been reviewed extensively and critiqued elsewhere [4,19,20,42,53–56], so only essential remarks will be made here.
The traditional aqueous-based surgical scrubs (TAS), which are most familiar to currently practicing surgeons and operating room staff, are CHG and iodophors. Others, such as hexachlorphene, triclosan, and para-chloro-meta-xylenol (PCMX, chloroxylenol), have fallen out of favor because of toxicity, inferiority, or both and will not be discussed.
Chlorhexidine gluconate was developed in England at Imperial Chemical Industries in 1954 and made its way to the United States in the second half of the 20th century [20,57]. It is a cationic bisbiguanide that elicits antimicrobial activity through the binding and disruption of microbial cell membranes and is not inactivated in the presence of blood or serum proteins [4,20]. It is capable of binding the stratum corneum, allowing sustained release and residual activity [58]. An iodophor is a complex of iodine and a carrier (e.g., povidone) that increases solubility and serves as a reservoir for free iodine, the factor that contains the antimicrobial properties of cell wall penetration, oxidation, and substitution of microbial contents [20]. Despite the common use of both products, CHG is superior to PVP-I [59–64]. Initial reductions in bacterial counts are similar or more pronounced; however, CHG promotes a residual and persistent effect that is not demonstrated by PVP-I [31,37,59,64]. Furthermore, iodophors are harsher, cause more skin sensitivity, and are neutralized in the presence of organic matter [20,58].
In a 1988 study by Aly and Maibach, 42 healthy volunteers underwent a 14-day pre-test period followed by a one-week baseline period and were then randomized to either CHG 4% (Hibiclens®), PVP-I 1% (E-Z Scrub™ 201), or chloroxylenol 3% (ParaSoft™) [65]. Subjects were included if their baseline hand flora amounted to more than 106 organisms. The scrub protocol involved removing all jewelry and clipping the fingernails to 2 mm or less. Subjects then cleaned under their nails with a nail stick and performed a non-medicated soap wash. A two-minute scrub followed. Samples were then collected at immediate (right hand), three-hour (left hand of half the subjects), and six-hour time points (left hand of remaining half of the subjects) on days 1, 2, and 5 using the glove juice method; neutralizers were added to the culture medium and studies were performed confirming that adequate neutralization had been obtained. Subjects scrubbed for an additional time after sampling on days 1 and 2 and for a total of three times on days 3 and 4 (11 total scrubs). Dermal irritation assessments were made before and after the test period.
Among the 39 subjects studied, CHG had significantly higher bacterial mean log10 reductions at all sampling times than PVP-I and chloroxylenol. The reductions increased progressively on successive days. Although PVP-I demonstrated reductions from the baseline count immediately, it failed to do so at the three- and six-hour sampling times. All six-hour counts for PVP-I and chloroxylenol exceeded the baseline counts, and no cumulative activity was noted for either product. Although mean irritation score differences among the test groups were not statistically significant, dermal irritation scores worsened by one grade for CHG (n = 1), PVP-I (n = 4), and chloroxylenol (n = 2) and improved by one grade for PVP-I (n = 1) and chloroxylenol (n = 1). In this study, neutralizers specific to each test agent were utilized but were added to the culture medium only (not the sampling fluid), and the data validating neutralizer efficacy were not reported. Furthermore, this study utilized healthy nonsurgical volunteers who may not have had hand flora representative of actual product users, and hand sampling was not randomized. Lastly, the degree of activity performed by the gloved hand for either three or six hours after the scrub procedure was not specified.
The advent of alcohol-based hand rubs (ABR) has challenged tradition and hastened the surgeon's ritualistic moments before surgery [66,67]. As traditional scrubs have been criticized for the negative effect of friction on the hands, EA has been criticized for its drying effects [42]. The appropriate type and concentration of EA has remained a point of contention among users.
In 1950, Price performed a series of experiments with the intention of identifying the most efficacious concentration and application time of EA both in vitro and on the hands and arms of human subjects [68]. He concluded that concentrations of 70%, 80%, 90%, and 92.3% by weight (95% by volume) were comparable in both types of experiments, although the germicidal activity was slower on the skin. A concentration of 70% by weight was deemed most advantageous, as it was no less effective and yet possibly less irritating and dehydrating to the skin. Altogether, Price recommended the following: A preliminary scrub, a brief wash of the hands and arms in EA 95% by volume to ensure all traces of water are removed, and a two–three minute scrub with washcloth friction of EA 70% by weight. Regardless of the original flora characteristics, this method would reduce bacterial counts to 1%–2% of the initial values.
In the same year, Morton measured in vitro bactericidal action of various concentrations of EA [69]. His goals were to refute the literature at that time, which stated that EA 95% was worthless as a disinfectant, and also to use the customary procedure of his time as opposed to the outdated experiments of testing germicides against microorganisms dried on threads or garnets. He found that EA 40%–100% by volume killed Escherichia coli, Salmonella typhosa, and Serratia marcescens in 10 seconds or less. Pseudomonas aeruginosa was killed in a similar time by EA 30%–100% by volume, and EA 60%–95% by volume killed Micrococcus pyogenes, Staphylococcus aureus, and Streptococcus pyogenes in 10 seconds or less.
Looking at comparative studies, Rotter et al. in 1980 evaluated the mean log10 reduction of resident bacteria by n-propanol 60%, isopropanol 60%, CHG 4% (Hibiscrub™), and PVP-I 0.75% (Betaisodona™) [31]. Bacterial counts were established before and immediately after product application on one hand and three hours after product application on the opposite gloved hand. Hand selection for immediate or residual testing was randomized. Fifteen volunteers in a Latin square experiment performed each procedure once, each separated by one week. Baseline values were obtained after washing with non-medicated soap for two minutes, drying both hands, and then rubbing the fingertips of each hand for one minute on the base of a Petri dish. Neutralizing agents were used for CHG and PVP-I but not alcohol. The PVP-I was applied for approximately five minutes, CHG for three minutes, and isopropanol and n-propanol for five minutes. Post-treatment testing was performed by fingertip sampling similar to the baseline method described.
The mean log10 reduction of n-propanol was significantly superior (p < 0.05) to isopropanol, CHG, and PVP-I at the immediate (3.43 vs 1.65, 0.78, and 0.92, respectively) and three-hour (2.94 vs. 1.04, 0.75, and 0.24, respectively) time periods. The superiority of CHG to PVP-I was statistically significant at three hours (p < 0.05). The volunteers were non-surgical personnel, and no efficacy or toxicity studies regarding the neutralizers utilized were referenced. Also, no activity during the gloved period was described. Unpublished results from Rotter ranked mean log10 reductions of test bacteria by type of alcohol and found n-propanol 60% superior to isopropanol 70%, which in turn was superior to EA 85%; all alcohols were superior to CHG 4% [70]. It is suggested, however, that EA is less cytotoxic and irritating than isopropanol and n-propanol [42,56].
Larson in 1990 looked at EA 70% plus CHG 0.5% (ALC), triclosan 1%, CHG 4%, and PVP-I 7.5% (Betadine®) [58]. Following a three-day baseline period during which the subjects were given non-medicated soap for daily use, subjects were randomized to either one of the four treatment groups or to a control group (non-antimicrobial liquid soap). Each subject removed all jewelry and nail polish and clipped the fingernails to no longer than 2 mm. Subjects scrubbed once daily for five minutes over five days using a standardized and observed scrub technique. Micro-organisms on the hands were assayed on days 1 and 5 using a modification of the glove juice technique both immediately after the scrub and four hours later.
Bacterial mean log10 reductions immediately after scrubbing on day 1 were significantly greater (p < 0.01) than in the control group (0.39) for all treatment groups (ALC 1.98, CHG 0.86, and PVP-I 1.08) except triclosan (0.56). Similarly, immediately after the final scrub on day 5, all treatment groups (ALC 2.85, CHG 1.56, and PVP-I 1.57) had better results than the control group (0.42), with ALC demonstrating a significantly greater mean log10 reduction than CHG, PVP-I, and triclosan (p = 0.009). No mean log10 CFU count at four hours on day 1 reached or exceeded baseline, and all counts remained significantly lower than in the control group (p < 0.03) except for PVP-I (p = 0.41). After four hours on day 5, all antiseptic groups had significantly lower mean CFU counts than the control group (p < 0.0001). With regard to skin effects, subjects who used triclosan and CHG reported higher ratings for skin appearance, sensation, intactness, and moisture content post-scrub compared with baseline. The iodophor was rated as the harshest and the alcohol between the iodophor and other formulations. These subjects were non-surgical volunteers of the study institution, and there was no evidence of neutralizers in the sampling fluid. Also, it was unclear if randomization occurred as to which hand would be gloved in preparation for the four-hour sample or what activity was performed during that time. Lastly, the baseline period was likely insufficient to allow for complete restoration of resident skin flora.
In 1998, CHG 1% plus EA 61% (Avagard™) was compared with CHG 4% (Hibiclens®) in a single-center, randomized, parallel-group, partially blinded study, as required in their NDA [71]. Subjects were healthy volunteers age 18–65 y without cuts, abrasions, or irritation on the hands who had baseline culture counts of ≥1.0 × 105 CFU/hand. Subjects were excluded if they were exposed to topical or systemic anti-microbial agents; if they had bathed in chlorinated water; if they exhibited any form of dermatitis, open wounds, or other skin disorders; if they had a sensitivity to CHG or alcohol or latex allergy; if they were pregnant or nursing or of child-bearing potential and not using adequate birth control; or if they had artificial nails or nail tips. The study followed the 1994 TFM methodology. The ABR was applied as follows: A nail stick was used for the first scrub of each day, three aliquots of 2 mL were applied to first rub one hand/forearm, then repeated for the other side, and the third aliquot was applied to the hands only. The product was allowed to dry before gloves were donned. The TAS was applied as follows: A nail cleaner was used for the first scrub of each day, the hand/forearms were wet, 5 mL of product was applied with a scrub brush for three min followed by a 30-sec rinse, after which the process was repeated and the hands dried with a sterile towel before donning gloves. The incidence of adverse experiences was compared for the groups, and the subjects evaluated the conditions of their hands through a questionnaire.
Results showed mean baseline log10 counts of 6.3 and 6.4 for the ABR and TAS, respectively. Mean log10 reduction factor TFM criteria after the first, second, and eleventh wash were met for both the ABR (2.5, 3.0, and 3.7, respectively) and TAS (1.8, 2.6, and 3.7, respectively). No statistical superiority was noted for either product [72]. Adverse events included two subjects who withdrew for reasons unrelated to drug use, and one subject who developed a maculopapular rash lasting 23 days while using the ABR. For skin ratings, the ABR was noted as having more moisture content, whereas the other comparisons revealed no differences. A separate neutralization validation study was submitted in the year 2000 with a satisfactory result.
Bryce et al. in 2001 published a prospective clinical trial comparing IPA 70% (Manorapid®) with CHG 4% and PVP-I 7.5% in an in-use evaluation [73]. Because of its in-use design, subjects were not asked to abstain from anti-microbial products nor were glove use or other operative practices modified. Operations of a less than two hours duration (Phase 1) were selected from one site, where three surgical nurses and 22 surgeons participated, and cases of more than three hours (Phase 2) were selected from a second site, where 10 surgical nurses and six surgeons participated. In Phase 1, subjects used their preferred TAS product for a two-week period. Fingertip impression cultures and 15 sets of pre-operative and post-operative cultures were obtained using the glove juice method. The subjects then switched to the ABR for an additional two weeks. Skin integrity was evaluated before and after use for each product, and acceptability questionnaires were completed.
Once results revealed that the ABR was as effective as the TAS, Phase 2 was initiated. In Phase 2, subjects used the ABR for the initial two-week period then switched. Fingertip impression and glove juice cultures, skin integrity evaluations, and questionnaires were collected as described for Phase 1. Traditional scrubs were applied for three minutes following use of a nail pick. Then IPA 70% (5 mL) was placed in a cupped palm, and the opposing fingernails were dipped into the solution. The solution was then transferred to the opposite palm and the procedure repeated. The remaining solution was rubbed into the hands/wrists. A second aliquot of solution was then rubbed into both arms up to the elbow. Lastly, a third aliquot was applied to both hands. Total rub duration was three minutes. Prior to the first case of the day, subjects performed a one minute pre-wash with neutral soap and dried their hands prior to IPA 70% application.
Fingertip impression cultures were collected after application of either product, as well as after the surgical procedure, whereby all five digits of a dry hand were placed on a blood agar plate (a nail print was included). A glove juice culture was obtained after application of either product by the usual method except that sampling fluid was withdrawn via syringe from the middle finger after the outside of the glove was cleaned with an alcohol swab. The subject then dried that hand with a sterile towel and donned new sterile gloves. At the completion of the procedure, the previously un-sampled hand was sampled by the glove juice method. Samples were plated within four hours, and negative growth controls of the sampling and neutralizing solutions were included with each set. Neutralizing agents were incorporated into the diluent and agar plates. Bacterial counts were made by two individuals independently. Neutralizer efficacy and toxicity studies were performed.
There was no evidence of significant toxicity for the neutralizers. In Phase 1, no significant difference between the groups was found from the fingertip impression cultures (CFU/mL) either pre-operatively (TAS 16.8 vs. ABR 12.8) or post-operatively (TAS 29.6 vs. ABR 9.0). Similarly, there was no difference in glove juice cultures (log10 count) pre-operatively (TAS 3.5 vs. ABR 2.9) or post-operatively (TAS 3.1 vs. ABR 2.7). For the longer cases, in Phase 2, alcohol proved significantly better (log10 count) pre-operatively and post-operatively (TAS 4.5 vs. ABR 3.5 and TAS 5.2 vs. ABR 4.7). However, when a matched-control analysis using subjects from both phases was performed for glove juice cultures, no difference (log10 count) was noted pre-operatively or post-operatively (TAS 3.5 vs. ABR 3.2 and TAS 3.8 vs. ABR 3.3). Skin integrity evaluations and product assessment questionnaires also revealed no difference between the product types. This study did not randomize TAS use and did not incorporate neutralizers in the sampling fluid. A four-hour window was allotted for plating, which may have led to falsely low bacterial counts after TAS use, as the ABR could have been neutralized by dilution.
A similar prospective observational study was performed by Shen et al. in a Taiwanese 2,388-bed medical center [74]. Surgeons and nurses with pre-operative hand antisepsis experience were allocated to either the intervention ABR group (CHG 1% + EA 61%; Avagard™) or the conventional TAS group (CHG 4%; Hibiscrub® or PVP-I 7.5%) based on user preference. Subjects were excluded if both pre-operative and post-operative samples were not obtained or if baseline data were missing. The ABR was applied in three aliquots of 2 mL each to include both hands and forearms, with the third aliquot rubbed on the hands only (rub duration two min). The TAS application utilized 6 mL of product applied over five min, which was then rinsed off. This process was repeated except that the hands were dried with a sterile towel rather than rinsed. Samples were obtained from each subject both pre-operatively and post-operatively by wiping every aspect of both the ventral and dorsal sides of the hands and the interdigital spaces as well as the wrists using a saline-moistened sterile cotton swab, which was inoculated onto sheep agar plates. A blinded bacteriologist read the plates, and all pathogens were identified.
Of 154 subjects invited to participate, 128 were enrolled. There were no differences in the demographic characteristics of the two groups, but the ABR group was involved in more orthopedic operations (6 vs. 0; p = 0.002) and the TAS group in more neurologic procedures (9 vs. 0; p = 0.014). The ABR showed a significantly higher amount of allergies than PVP-I (p = 0.016), and the median blood loss was 10 mL and 20 mL for the ABR and TAS groups, respectively (p = 0.036). Positive pre-operative cultures were found in 6.2% and 47.6% of the ABR and TAS samples, respectively (p < 0.001). Similarly, post-operative positive cultures were noted in 10.8% and 25.4% of the ABR and TAS samples, respectively (p < 0.031). Univariable analyses comparing positive and negative culture samples showed that ABR was associated with more negative cultures than was TAS (p < 0.001). Similarly, subjects involved in cardiovascular operations had more negative samples (p = 0.043), whereas those involved in ear-nose-throat procedures had more positive cultures (p = 0.036). Furthermore, positive sample cultures were more apt to be observed in clean-contaminated cases (p = 0.012) or when subjects had injuries on their hands (p = 0.024). All significant covariables were then added to a multivariable regression analysis; ABR was the only protective factor among the group with positive samples (p < 0.001). This study utilized a non-randomized cohort and did not include neutralizers in the growth medium. Also, TAS products were not rinsed off after the repeat application, and the sample collection technique was atypical.
In a non-inferiority study by Olson et al. in 2012, three ABRs were compared: CHG 1% + EA 61% (Avagard™), EA 80% (Sterillium®), and EA 70% (Surgicept®) [75]. The study was conducted on 129 healthy male and female volunteers using modified 1994 TFM criteria. Subjects participated in a one-week washout period following which, baseline samples were secured using the glove juice method on three separate days. Subjects qualified for the study if the mean baseline counts were ≥5 log10 CFU/hand. Next, subjects were randomized to one of the three products, and the hands were randomized to the sampling time points. Subjects refrained from washing their hands or applying lotion within two hours of product application or sampling. Also, fingernails were maintained with a ≤2 mm free edge, and all jewelry was removed. A total of 12 applications according to the manufacturer's instructions ensued over five days, with samples collected twice on days 1 and 5, with the first being taken immediately after the product had air-dried and the second at 6–6.5 hours. The glove juice method was again used and incorporated a neutralizer on which the authors performed separate efficacy and toxicity testing according to ASTM E-1054 method.
Of the 129 subjects, 83 qualified, and 82 completed the study. Subjects were predominantly female and white. The mean baseline bacterial counts were similar for CHG 1% + EA 61%, EA 80%, and EA 70% (6.11, 6.24, and 6.14, respectively; p = 0.26). Non-inferiority was demonstrated between the bacterial log10 recoveries of CHG 1% + EA 61% and both EA 80% and EA 70% at the immediate time point on days 1 (3.62 vs. 3.75 and 4.00, respectively) and 5 (3.47 vs. 3.71 and 3.65, respectively). Additionally, CHG 1% + EA 61% was superior to EA 80% at six hours on days 1 (3.21 vs. 5.13; p < 0.0001) and 5 (3.13 vs. 4.56; p < 0.0001) as well as to EA 70% at six hours on days 1 (3.21 vs. 4.55; p < 0.0001) and 5 (3.13 vs. 3.74; p = 0.026). No adverse reactions were reported for any product. Criticisms of this study include that the volunteers were non-surgical personnel and that there was no reported standardized activity for the volunteers to engage in while awaiting the six-hour sampling point. Furthermore, data were not presented as mean log10 CFU reductions, as dictated by the 1994 TFM, which, when calculated, revealed that a three-log10 reduction was not accomplished immediately after the wash on day 5 by any of the products. Thus, the TFM criteria were not met. Lastly, validation of neutralizer effectiveness and toxicity was not presented.
Macinga et al. designed a study using TFM methodology, which included a 14-day pre-test period, a five-day baseline period, and a five-day test period comparing CHG 4%, CHG 1% + EA 61%, EA 70%, EA 80%, and an EA 70% control (EAC) [76]. Participants applied the randomly assigned test product according to the product manufacturer's instructions once on days 1 and 5 and three times on days 2, 3, and 4 (11 applications). Additional randomization (Phase 1) was made for EA 70%, where patients either applied a 2-mL sample to each hand and forearm only (total 4 mL) or used a third sample of 2 mL (6 mL total) to both hands after the first two applications had dried. The CHG 4% scrub (5 mL) was applied using a scrub brush for 1.5 minute per hand followed by a 30-second rinse, after which the process was repeated but with a one-minute rinse per hand. In Phase 2, application of EA 80% utilized two aliquots of 2 mL each, as previously described, but in order to keep the subject's hands wet throughout the entire period (∼two minutes), additional aliquots were dispensed as needed (average 8 mL total). Also, CHG 1% + EA 61%, EA 70%, and EAC were applied using the three-aliquot technique described above. A minimum of one hour elapsed between product applications. After gloving, samples were obtained immediately and at three hours and six hours on day 2 and immediately and six hours after application on days 1 and 5. Bacterial recovery was measured using the glove juice method; gloved hands were randomized to collection time. Neutralizers were used in the diluent and culture medium.
In Phase 1, both EA 70% and CHG 4% met all FDA criteria. The immediate mean log10 reduction produced by CHG 4% started low and increased throughout the test period (1.35 vs. 3.77; p < 0.001), whereas EA 70% started higher and did not increase (3.08 vs. 3.02 and 2.31 vs. 3.15 for three-aliquot and two-aliquot applications, respectively). Comparing the products, three aliquots of EA 70% produced a significantly higher mean log10 reduction than did CHG 4% immediately on day 1 (3.08 vs. 1.35, respectively; p < 0.0001). Using either two or three applications of EA 70% produced a higher mean log10 reduction than did CHG 4% at six hours on day 1 (2.18 and 2.29 vs. 0.49, respectively; p < 0.0001) and day 2 (2.46 and 2.51 vs. 1.33, respectively; p < 0.05) but not on day 5 (2.87 and 2.64 vs. 2.75, respectively).
In Phase 2, the remaining products, including EAC, met the FDA criteria on days 1 and 2, but only EA 70% met the three-log10 reduction immediately after use on day 5 (3.06 vs. EAC 2.07, EA 80% 2.43, and CHG 1% + EA 61% 2.7). Also, EA 70% was the only test product to demonstrate significantly greater mean log10 reductions than EAC at the immediate time point on days 1, 2, and 5 (2.71 vs. 1.76, 2.87 vs. 1.91, and 3.06 vs. 2.07, respectively). On all three sampling days, at six hours, EA 70% (2.55, 2.57, and 2.53 for days 1, 2, and 5, respectively) and CHG 1% + EA 61% (2.65, 2.76, and 3.06 for days 1, 2, and 5, respectively) produced significantly greater (p < 0.05) mean log10 reductions than EA 80% (0.88, 1.07, and 1.48 for days 1, 2, and 5, respectively) and EAC (0.5, 0.26, and 0.68 for days 1, 2, and 5, respectively). No significant differences were noted between EA 70% and CHG 1% + EA 61%. This study used non-surgical, healthy volunteers, of which 18 per study arm were targeted, but no information was given as to how many were recruited or completed the study. Neutralizers were not used in the sampling fluid, and neutralizer efficacy and toxicity testing results were not reported.
All preceding studies used CFUs as a surrogate endpoint for SSI. They have demonstrated the comparative effectiveness (in descending order) of alcohol, CHG, and PVP-I. In contrast, limited data exist using SSI as an endpoint. A Cochrane review was performed in 2008 and was updated in 2016 [77,78]. In the 2008 publication, only one equivalence, cluster, cross-over trial randomized by surgical service measured SSI rates within 30 days [79]. Parienti et al. compared a five-minute scrub with either aqueous PVP-I 4% (Betadine®) or CHG 4% (Hibiscrub®) with a five-minute rub of propanol-1 30%, propanol-2 45% + mecetronium ethylsulfate 0.2% (Sterillium®); the ABR was preceded by a single hand wash with non-medicated soap at the start of each day or when the hands were soiled [79]. Users assigned to the TAS group were allowed to choose between PVP-I or CHG. Six surgical services from teaching and non-teaching hospitals in France were randomized to use either the TAS or ABR for one month, at which point, they switched to the other intervention. This continued for 16 months and involved the entire surgical team in each hospital. A total of 4,387 patients undergoing consecutive clean or clean-contaminated cases were included. The SSIs were assessed at 30 days using the CDC definition via observation, medical record review, outpatient visits, or telephone calls by a surgeon, infectious disease specialist, or hygiene specialist.
The SSI rates for TAS and ABR were 2.48% and 2.44%, respectively (risk ratio [RR] 1.02; 95% CI 0.70–1.48). Criticisms of this study include that it was powered only for equivalence and not to demonstrate a statistically significant difference. Also, it does not appear as though clustering was accounted for in the analysis. Furthermore, detection bias was possible, as the surgeon or in-charge physician confirming SSIs was un-blinded to the surgical antisepsis protocol. The study also did not provide information on patient co-morbidities, pre-operative antibiotic use, post-operative care, breaks in aseptic technique intra-operatively, or SSI microbiology, which may have helped to link the SSI to particular surgical personnel.
In 2009, Al-Naami et al., also in an equivalence trial, compared either a three–five-minute hand scrub using either PVP-I 7.5% (Betadine®) or CHG 4% (Hibiscrub®) with EA 62% (Purrel®) [80]. A total of 500 patients undergoing clean or clean-contaminated procedures were randomized. All procedures utilized standardized skin preparation, and certain cases warranted prophylactic antibiotics. Identification of SSIs using the CDC definition occurred before discharge, approximately one week post-operatively and at 30 days. Surgeons who identified SSIs were blinded to the hand antisepsis protocol. Regardless of group, surgeons scrubbed with an aqueous solution for the first procedure of the day.
The SSI rates were 5.3% in the TAS group and 2.9% in the ABR group (OR 1.833; 95% CI 0.68–5.01). Additional findings included skin reactions (e.g., itching, redness, urticaria, or dryness) in 17.5% and 11.4% of surgeons in the TAS and ABR groups, respectively (OR 1.65; 95% CI 0.97–2.83) and that 64% preferred the ABR. Also, there was no difference in the distribution of the organisms cultured from the SSI (p = 0.71). It was noted that to achieve a power of 0.8 and an alpha of 0.05, 4,003 patients would have been required. Also, following randomization, additional exclusions (24% from TAS and 9% from ABR) were made because of information obtained from histopathological examination, incomplete forms, or failed follow-up. It also was unclear whether there was a statistically significant difference in the distribution of case types between groups (e.g., open inguinal hernia 13.1% and 5.1% in the TAS and ABR groups, respectively).
In 2010, Vergara-Fernandez et al. compared CHG 4% using a brush and sponge with CHG 1% + EA 61% (Avagard™) in a single institution [81]. Four hundred staff members operated on 100 patients undergoing clean and clean-contaminated procedures who were randomized to one of the two groups. All members of the operative team used the assigned product. An observing physician, independent of the surgical group, noted application duration and technical and dermatologic concerns. Satisfaction was measured using a visual analog scale (0 dissatisfied to 10 satisfied) designed by the institution. Estimates of water consumption were made in 10% of the TAS group by utilizing the observed application duration and known flow rate (6 L/min). Following product application, the hands of 20% of the subjects from each group were cultured. Surgical site infections were assessed by medical personnel at 30 days using the CDC criteria.
The duration of application (mean ± standard deviation) for TAS and ABR was 3.9 ± 1.07 minute and 2.0 ± 0.47 minute, respectively (p = 0.00001). The mean water consumption per TAS application was 2.9 L; extrapolated for the whole cohort, this yielded a total of 580 L at a cost of 6,035 pesos. This was compared with a cost of 4,687 pesos in the ABR group. Positive hand cultures were reported in 25% of the TAS group and 12.5% of the ABR group (p = 0.152), and the SSI rates were 2% in the TAS group and 4% in the ABR group (RR 0.5; 95% CI 0.05–5.34; p = 0.31). Users rated the ABR higher in satisfaction (9.5 ± 1.54 vs. 9.1 ± 1.39; p = 0.004), and fewer subjects reported hand dryness (2% vs. 6.5%; p = 0.02).
This study failed to report on the methods of hand culture, collection process, sampling fluid, diluent, plating, use of neutralizers, incubation period, and who interpreted the results. Also, few baseline staff characteristics are provided, with no demographic data pertaining to the patients within each group. Lastly, it is unclear if the independent observer or the personnel identifying SSIs were blinded to patient group assignments.
Nthumba et al. compared basic hand hygiene with soap and water or isopropyl alcohol 75% plus hydrogen peroxide 0.125% plus glycerol 1.45% (World Health Organization-recommended formulation II) in a longitudinal comparative cluster-randomized crossover trial in a rural Kenyan hospital [82]. Patients were allocated to one of the groups according to six operating theatres (plain soap or ABR). There were ten clusters during five two-month intervals with cross-over after each two-month period. Steam sterilization was employed, and skin preparation with PVP-I solution was applied to the surgical site prior to incision. Regardless of group, surgeons scrubbed with a non-medicated soap for the first procedure of the day and also if there was visible soiling. The ABR involved the application of 7–10 mL of product for three minutes, keeping the hands wet throughout. A trained nurse blinded to the surgical hand antisepsis protocol assessed for SSIs using modified CDC definitions within 30 days of surgery by direct observation on the surgical ward, at the outpatient clinic visit, or via telephone. The trial included 3,317 patients undergoing clean and clean-contaminated procedures. Patients undergoing contaminated or dirty procedures, those with incomplete case records, and those who underwent a second procedure within two weeks of the index procedure were excluded. In contrast to the study of Parienti et al., clustering and cross-over were incorporated in the power calculation and analysis.
Baseline characteristics were significantly different between groups for surgical specialty, American Society of Anesthesiologists classification, type of anesthesia, and operating theatre assignment (p < 0.05). The SSI rates were 8.0% and 8.3% for the soap and water and ABR groups, respectively (OR 1.03; 95% CI 0.80–1.33). Adjusting for the confounders listed above, as well as cluster effects, yielded no change (OR 1.06; CI 0.81–1.38). Lastly, attrition was similar in the two groups (5.1% and 6.0%, respectively). The authors were underwhelmed with the SSI rate (lower than expected) and therefore underpowered the study. However, the rates reported here are higher than those reported from developed countries in this review. Heavy reliance on phone calls to determine SSI outcomes was also disadvantageous.
Discussion
The state of surgical hand antisepsis testing has been evolving since the 1970s. The result of arbitrary mean log10 reduction thresholds being included in the original Monograph has led to much discussion over the last 20 years regarding whether these “pass/fail” markers correlate with a reduction in clinical infection [83]. The work included herein from decades past whereby inocula of different quantities were applied to human skin in order to demonstrate the threshold for clinical infection likely will never be replicated, as they would be unlikely to pass any Institutional Review Board. Multiple reviews of the literature have failed to identify any modern study that clearly links either an absolute value or log10 reduction factor to a reduction in SSIs. As stated at the NDAC March 2005 meeting, it would be unethical to perform a study comparing either placebo or soap and water with a surgical hand antisepsis agent at a facility where such products are readily available [83]. It also was suggested that studies designed to both measure the clinical surrogate (CFU/mL) by standardized methods and identify clinical infections could help answer the threshold question.
After much debate, it has been agreed that demonstration of a cumulative effect is not required for a surgical hand antiseptic, and it is the immediate and persistent effects that are most logical to maintain [26,83]. The new two-log10 requirement within one minute after a single application is simply the median value between the 1994 TFM's immediate threshold (one-log10) and its cumulative threshold (three-log10). This effect possibly lies outside the ability of several currently marketed products, and once the Final Rule is imposed, only products that remain compliant may continue to be marketed according to the Rule, whereas others may require formulary changes in order to meet this mark. It is known that not only active ingredient selection but also the concentration of the ingredient and product formula can alter product effectiveness [84–86].
As demonstrated here, the majority of the literature has measured surrogate endpoints and is based on 1994 TFM, ASTM, or European methods; but often, there are unexplained modifications to proposed regulatory standards, which make the pooling of largely heterogeneous data impossible. Other studies have used an intermediate corollary rather than clinical SSI, such as pre-operative and post-operative micro-organism growth on the hands. And finally, even fewer studies have been designed with SSI as an endpoint. To date, none of the SSI studies have shown any benefit of one product type over another. This is despite an abundance of literature showing the inferiority of PVP-I to both CHG and EA, with EA often markedly outranking CHG in non-clinical in vivo tests. What remains true, however, is the global impact of these infections [87].
Conclusion
There are few studies that have utilized SSI as the primary endpoint, probably because of the economic and logistic challenges of performing a well-powered randomized controlled trial. The majority of research continues to measure CFU as a potential surrogate for SSIs, and this method is supported by the FDA's Proposed Rule, released in 2015. The concept that reducing bacteria on the hands of surgical personnel will lead to an appropriate and correlative clinical response has been discussed for decades, yet the actual degree by which microbial reduction must be achieved to guard against SSIs remains unknown. Furthermore, methodological and ethical reasons may, in part, prevent such detection. In vivo testing comparing alcohol, alcohol + other ingredients, and CHG 4% hand antisepsis options utilizing both FDA and European methods, along with randomized controlled trials utilizing SSI as the primary endpoint, are still warranted. Although still in use, PPV-I is least preferred for surgical hand antisepsis. Caution should be used when choosing a surgical antisepsis agent; the decision should rest on whether products meet all efficacy standards and are both tolerable and acceptable to the end user. The inclusion of skin tolerance and cost-analysis information in future work will help in this feat. As value care continues to evolve, surgical care bundles utilizing the most effective and affordable surgical hand antisepsis protocols may help reduce the variability of care quality worldwide.
Footnotes
Author Disclosure Statement
The opinions expressed are those of the authors and do not necessarily reflect those of the U.S. Department of Veterans Affairs.
Dr. Brad S. Oriel has no competing financial interests. Dr. Kamal M.F. Itani has received research funds to his institution from Merck, Sanofi, and Dr. Reddy's Laboratories. He was a research consultant for Irrimax.