
Abstract
Abstract
Background:
To evaluate the efficacy and safety of direct hemoperfusion with polymyxin B-immobilized fiber (PMX-DHP) therapy in patients with sepsis.
Design:
A systematic review and meta-analysis of four major databases: Cochrane Central Register of Controlled Trials, MEDLINE, Scopus, and Science Citation Index Expanded.
Study Selection:
Randomized controlled trials comparing PMX-DHP with conventional therapy on the outcome of mortality in patients with severe sepsis/septic shock.
Data Extraction:
Two reviewers independently applied eligibility criteria, assessed quality, and extracted data. Primary outcomes were mortality and adverse events. We used the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach to rate quality of evidence and grade the strength of recommendation.
Results:
In seven trials enrolling 841 patients, assessment for risk of bias indicated variations in study quality from high (n = 4) to unclear (n = 3) resulting from a lack of adequate randomization, blinding, and incomplete outcomes. Polymyxin B-immobilized fiber therapy was associated with lower mortality (risk ratio, 0.65; 95% confidence interval [CI], 0.47–0.89; p = 0.007; I2 = 72%). Significant heterogeneity among trials was explained partly by study venue and baseline mortality rate. Meta-regression analysis revealed a significant negative slope between effect size of PMX-DHP therapy and baseline mortality rate in individual studies (p = 0.003), suggesting the probability of a beneficial effect with PMX-DHP increased with increasing baseline risk. Polymyxin B-immobilized fiber therapy did not increase the risk of hemoperfusion-related adverse events. The quality of the body of evidence was considered low for both mortality and adverse events.
Conclusions:
Polymyxin B-immobilized fiber therapy was associated with reduced mortality in sepsis/septic shock. Based on the low quality of evidence, therapeutic use of PMX-DHP for survival benefit may be recommended conditionally for patients with high risk of death. Additional large randomized controlled trials are needed to confirm or refute this evidence.
S
Endotoxin, an outer membrane component of gram-negative bacteria, is recognized as the most potent trigger of the inflammation cascade in sepsis. Indeed, a previous study demonstrated a dose-response relation between endotoxin concentrations and adverse outcomes including organ dysfunction and subsequent death in patients with severe sepsis/septic shock [3]. Direct hemoperfusion with polymyxin B-immobilized fiber (PMX-DHP), an extracorporeal hemoperfusion technique to remove circulating endotoxin, was first developed in 1994 and proposed as an adjuvant therapy for sepsis in Japan. Over the past several decades, several single-center randomized controlled trials (RCTs) and observational studies have reported its superiority to conventional therapy in Japan [4–6]. In addition, since PMX-DHP received its product certification for use in Europe in 1998, several clinical trials have been conducted in European countries. The results of an Italian multi-center RCT published in 2009 by Cruz et al. [7] demonstrated that PMX-DHP therapy improved hemodynamics and reduced mortality in a targeted population with severe sepsis and/or septic shock from intra-abdominal gram-negative infections. However, a recent multi-center RCT published in 2015 refuted the treatment effect of PMX-DHP not only on mortality but also on hemodynamics [8]. So far, PMX-DHP therapy is not listed in the Surviving Sepsis Campaign guidelines [2], and the efficacy and safety of PMX-DHP against sepsis/septic shock is still under debate.
We conducted a meta-analysis of RCTs to examine the effects of PMX-DHP on mortality and adverse events when used in the resuscitation of adult patients with severe sepsis/septic shock compared with conventional therapy. The body of evidence for each outcome and the strength of recommendation were evaluated using the Grading of Evidence, Assessment, Development, and Evaluation (GRADE) approach [9,10].
Patients and Methods
Protocol and registration
This systematic review was conducted according to the recommendations and checklist from the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. We developed a protocol prior to conducting the review but did not register it.
Search strategy
A comprehensive search of four major databases of biomedical publications was performed on February 1, 2015: Cochrane Central Register of Controlled Trials (through February 2015), MEDLINE (source: PubMed, 1966 to February 2015), Scopus (1960 to February 2015), and Science Citation Index Expanded (1900 to February 2015). We used the search terms “PMX-DHP,” “DHP-PMX,” “PMX-F,” “Polymyxin B,” “Toraymyxin,” “hemoperfusion,” “hemosorption,” “hemodiafiltration,” “hemofiltration,” “hemodialysis,” and “purification” in each database. Full-text articles were retrieved and examined carefully to avoid potential duplicates or overlapping data. For specific information regarding our search strategies and results, see Supplementary Table S1 (see online supplementary material at http://www.liebertpub.com/sur). Other methods of study identification included searching names of authors of relevant studies and contacting industry. We also searched the reference lists of the included studies. We did not search the gray literature such as unpublished reports, theses, conference proceedings, newspapers, fact sheets, websites, and policy documents. When faced with insufficient or incomplete data, we contacted the authors of the studies directly.
Study selection and inclusion criteria
Two authors (T.T. and Y.U.) performed the study selection process independently. We performed the first selection based on the titles and abstracts identified from the searches and selected potentially relevant articles. Reviews, letters, comments, editorials, corrected publications, duplicate publications, and abstracts only were excluded, and any disagreements were resolved through discussion and consensus. We included trials with the following characteristics:
1. Study type: RCTs. 2. Population: adult patients with sepsis as proposed by the authors of the individual studies. 3. Intervention: PMX-DHP. The timing of PMX-DHP introduction after sepsis onset and number of sessions did not matter. 4. Control: standard therapy without PMX-DHP. 5. Outcomes: 28- to 30-d all-cause mortality and adverse events related to blood purification. 6. Sample size of the trials included: more than 30 patients because a sample size of at least 30 patients was required to provide 80% power at a 5% two-sided alpha level based on mortality rates reported in previous studies.
Risk of bias in individual studies
Three independent reviewers (T.T, K.Y., and Y.U.) assessed the risk of bias in individual trials as the methodological quality of the articles; disagreements were resolved by discussion and consensus. We applied uniform criteria for evaluating the risk of bias associated with individual RCTs based on the criteria recommended by the Cochrane Collaboration. We defined the overall risk of bias for an individual trial as low if all of the above domains except for blinding were conducted adequately.
Data extraction and outcome assessment
Using a standardized data extraction sheet, two independent reviewers (T.T. and Y.U.) extracted the data, with disagreements resolved by discussion and consensus. We identified the primary author's name, year of publication, study venue, inclusion and exclusion criteria, patient population, protocol of PMX-DHP therapy, mean value of the Acute Physiology and Chronic Health Evaluation II (APACHE II) score, mortality rate in the control group (control event rate), and duration of follow-up.
The primary outcome measures were all-cause mortality at 28 to 30 d after study entry as patient-important outcomes. As secondary outcomes, we assessed clinically important adverse events related to blood purification: hemodynamic complications such as hypotension and tachycardia, blood count disorders such as anemia and thrombocytopenia, and hemorrhagic episodes as proposed by the authors of the individual trials. Additionally, the differences in serum concentrations of endotoxin before and after PMX-DHP therapy in the PMX-DHP group were assessed.
Rating of the quality of evidence
Two authors (K.Y., a methodologist with expertise in both research methods and systematic reviews, and M.A., a member of the GRADE working group) used the GRADE tool independently to rate the quality of the body of evidence and the strength of recommendation. We applied the GRADE approach to rate the quality of evidence of PMX-DHP therapy for patient-important outcomes. Although the quality of evidence represented a continuum, we assessed the quality of the body of evidence for each outcome as high, moderate, low, or very low using the GRADEpro Guideline Development Tool [11].
Statistical analysis
We presented the results of all analyses using the random-effect model because this model incorporates statistical heterogeneity: (1) all of the studies included in the analysis were not equivalent functionally; (2) the subjects or interventions in the studies differed in ways that would have affected the results and therefore we should not assume a common effect size; and (3) our goal was to compute an effect size generalizable to other populations. For dichotomous parameters such as mortality, values for the risk ratio (RR) are expressed as a point estimate with 95% confidence interval (CI) and p value. All risk ratios refer to the risk for the PMX-DHP group compared with the control group. Statistical heterogeneity was assessed by the Mantel-Haenszel χ2 test and the I2 statistic. Substantial heterogeneity was predefined as a p < 0.10 with the Mantel-Haenszel χ2 test or an I2 value of more than 50%.
Possible sources for heterogeneity were investigated by several sensitivity analyses and meta-regression analyses. Sensitivity analyses were performed based on the study venue (Japan versus other countries), overall risk of bias (overall low risk of bias versus the others), or the start day of the first PMX-DHP session (first day after the diagnosis of sepsis versus the others). Additionally, to analyze the relation between severity of illness and the relative treatment effect, the log odds ratio of mortality in the PMX-DHP group was plotted against the control event rate or mean APACHE II score for each trial. A linear meta-regression weighted to reflect the variance of the individual studies was used to model the data.
To assess publication bias, we created funnel plots for mortality in which the log risk ratios were plotted against their standard errors, and we tested the symmetry of the funnel plots using Egger linear regression test.
All statistical analyses including risk of bias within studies and/or across studies were carried out with Review Manager Version 5.3.1. (RevMan; The Cochrane Collaboration 2012, The Nordic Cochrane Centre, Copenhagen, Denmark) and Stata version 14.0 software (StataCorp LP, College Station, TX). The level of statistical significance was set at a p < 0.05.
Results
Literature search
The PRISMA flow chart of study selection in the systematic review is shown in Figure 1. The combined search strategy identified 2,816 citations, of which 35 were judged to be potentially eligible based on titles or abstracts, or both, and the full texts were obtained. After excluding 28 articles after full-text review (Supplementary Table S2), seven RCTs enrolling 841 patients were judged to be eligible and were included in the review [4–8,12,13].
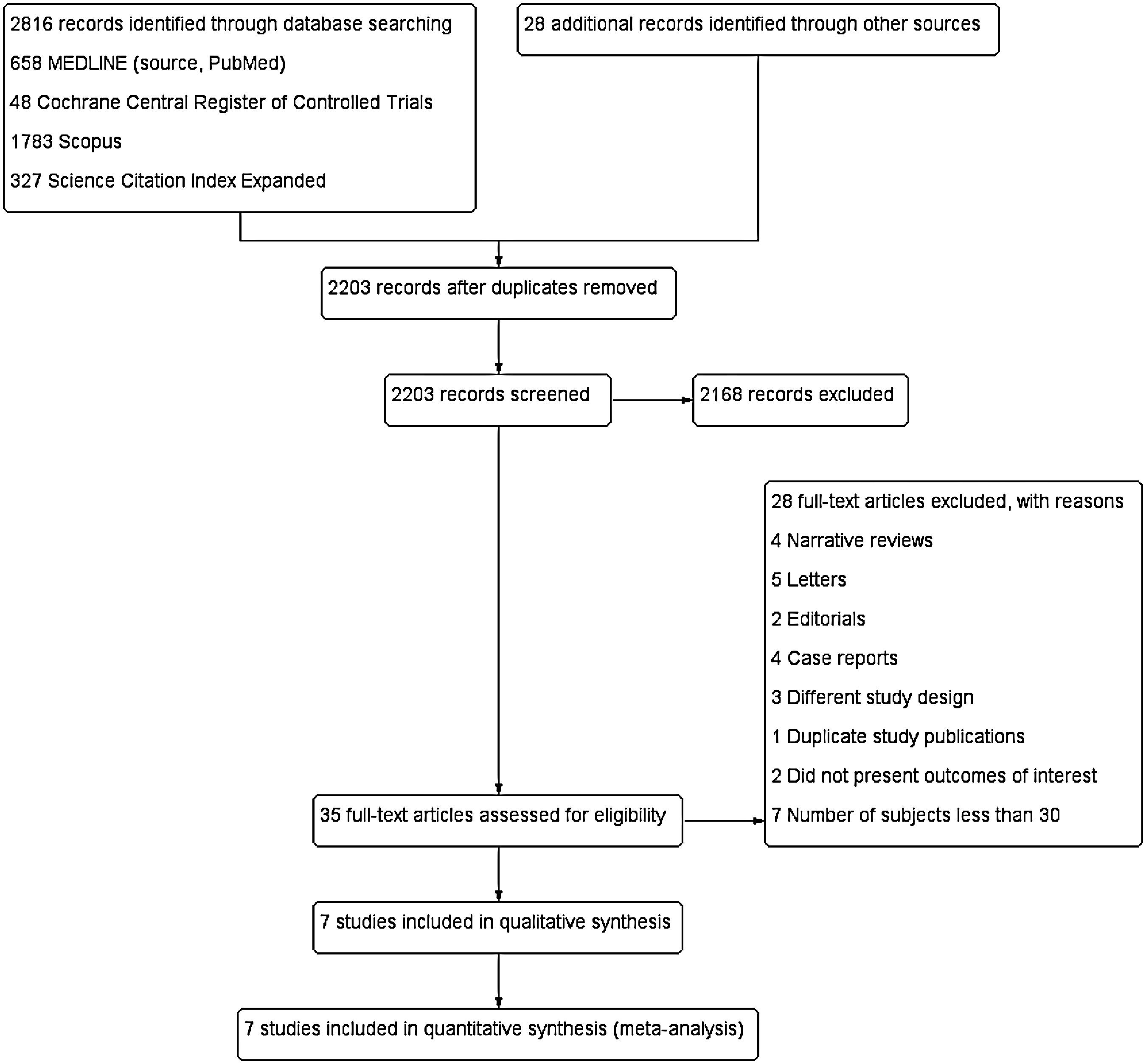
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) chart. Identification and selection of studies for inclusion.
Included trials
Study characteristics are summarized in Table 1. Included trials were published between 1999 and 2015. Four trials were carried out in Japan [4–6,12]. Most of the trials measured severity of illness by using the APACHE II score, and the mean score varied between 16.7 and 25 across the trials. There were some differences in PMX-DHP protocol, such as in the timing of PMX-DHP induction and the number of sessions in the trials. Direct hemoperfusion with polymyxin B-immobilized fiber in all included studies in this analysis was performed using Toraymyxin™ (Toray Industries, Tokyo, Japan).
Start of 1st PMX-DHP session indicates the day when PMX-DHP was first performed after diagnosis of sepsis.
PMX-DHP = direct hemoperfusion with polymyxin B-immobilized fiber; APACHE = Acute Physiology and Chronic Health Evaluation; AKI = acute kidney injury; NA = not available.
Risk of bias in included trials
The risk of bias evaluated in each included RCT is shown in the risk of bias summary in Figure 2. Randomization was performed in all seven trials, but only three trials specifically mentioned how the patients were randomized. For the blinding item, four trials were open-label RCTs and had high risk of bias, and the other three trials had unclear bias because of the lack of detail in describing the blinding of the patients and physicians. Other risk of bias domains was judged as trials with low risk of bias.
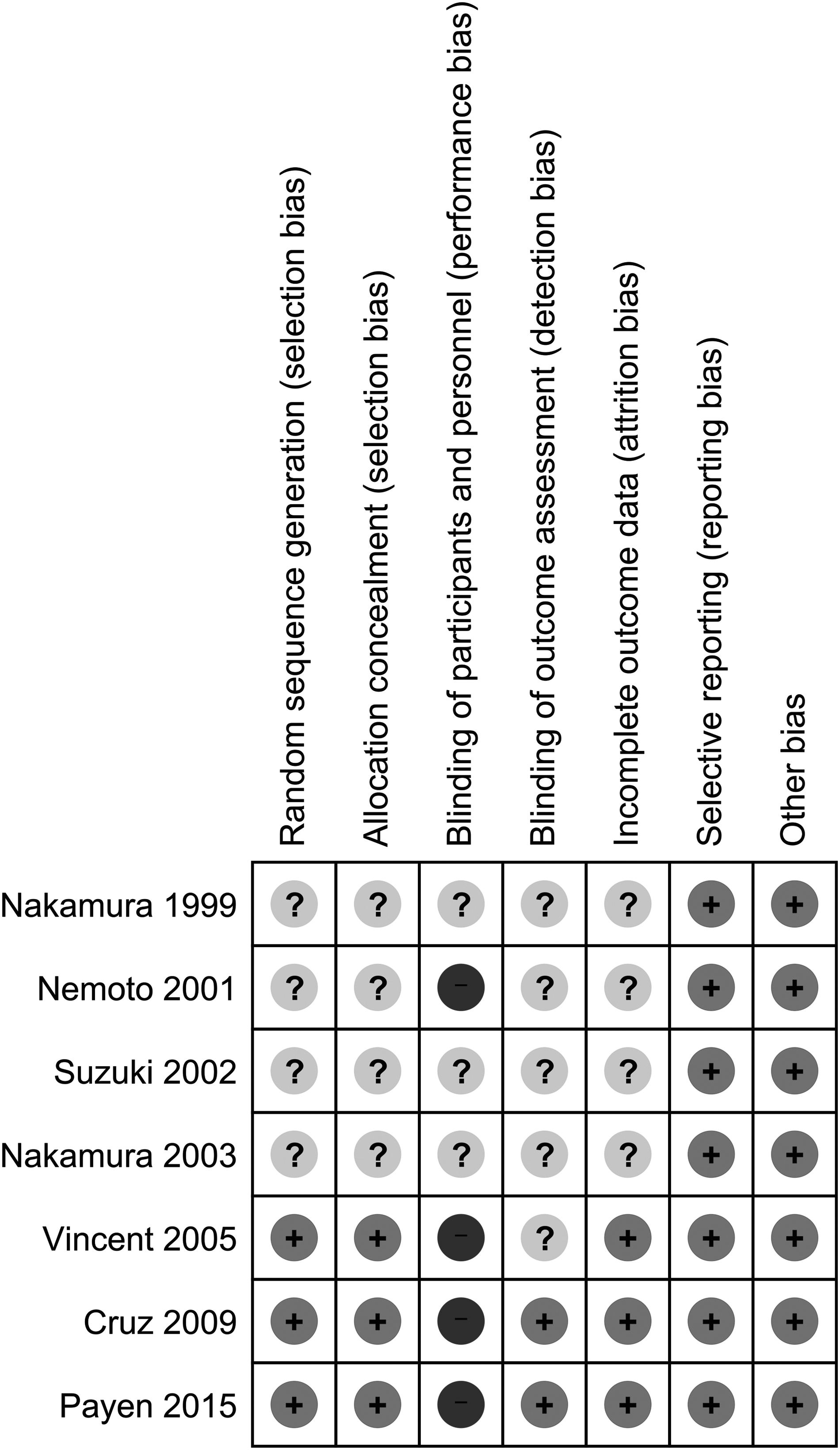
Risk of bias summary. Review of the authors' judgment of each risk of bias item for each included trial.
Effects on mortality
All seven RCTs reported all-cause mortality at 28–30 d. There was a reduction in mortality in the PMX-DHP group, and the pooled risk ratio was 0.65 (95% CI, 0.47–0.89; p = 0.007), as shown in Figure 3. Because there was substantial heterogeneity across the trials (I2 value = 72%, p = 0.002), we performed several additional analyses to identify trials contributing to this heterogeneity.
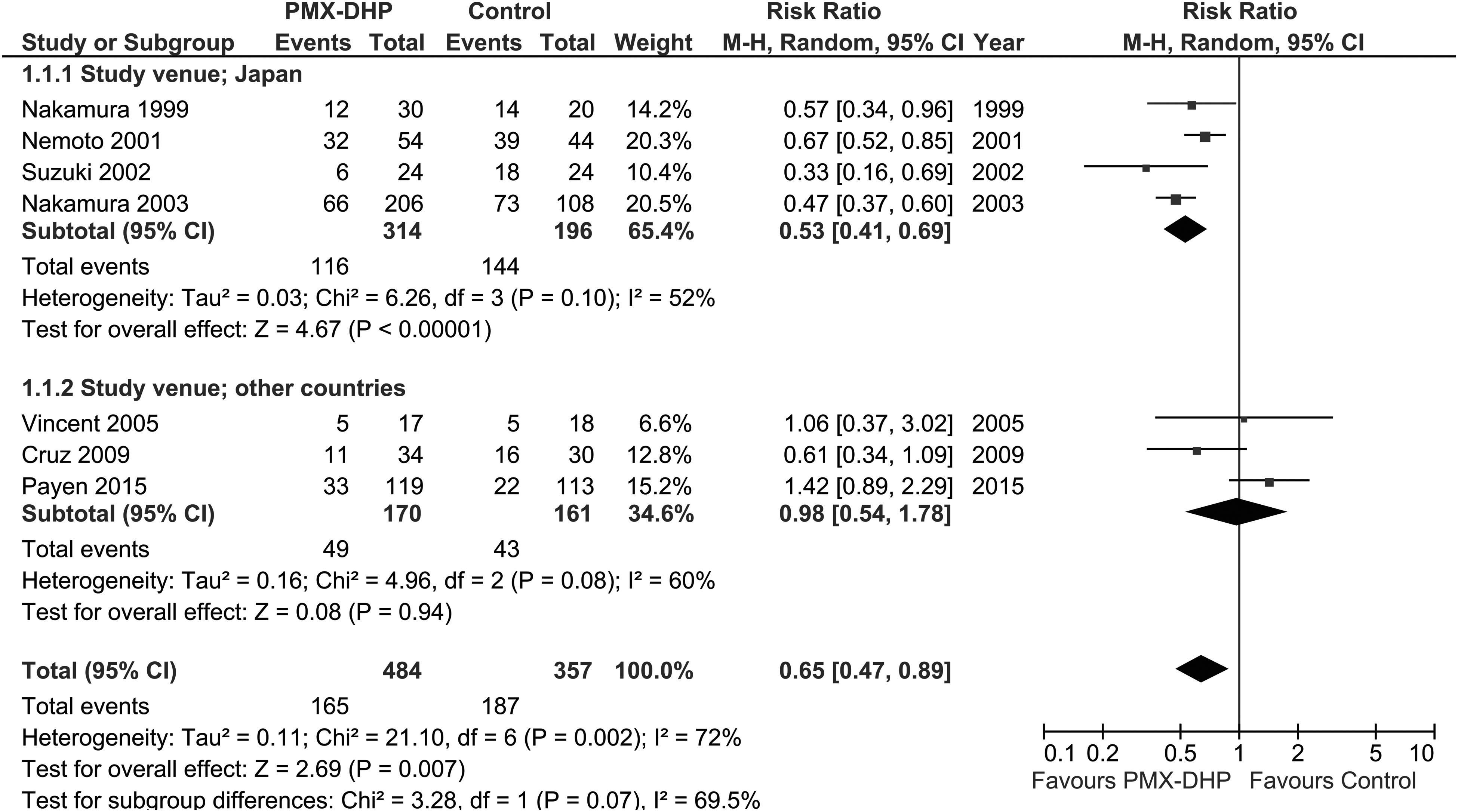
Forest plot of the comparison of PMX-DHP versus conventional therapy for all-cause mortality at 28–30 d. PMX-DHP = direct hemoperfusion with polymyxin B-immobilized fiber; M-H = Mantel-Haenszel; CI = confidence interval
First, we conducted a sensitivity analysis by dividing the trials according to the venues in which the studies were carried out. Consequently, the subgroup-specific pooled risk ratios were 0.53 (95% CI = 0.41–0.69) for the trials in Japan and 0.98 (95% CI, 0.54–1.78) for the trials in European countries, with less heterogeneity in both subgroup analyses. There was a difference in the effect size of PMX-DHP therapy between the subgroups of study venue (p = 0.07, I2 = 69.5%). We also conducted two additional sensitivity analyses according to the risk of bias and the day on which PMX-DHP was first performed. The subgroup-specific pooled risk ratios were 0.95 (95% CI, 0.41–2.20) for the two trials with low risk of bias and 0.55 (95% CI = 0.43–0.71) for the other five trials. The subgroup-specific pooled risk ratios were 0.73 (95% CI, 0.47–1.15) for the five trials in which PMX-DHP was conducted on the first day and 0.49 (95% CI = 0.39–0.61) for the other two trials. The result of influence analysis is shown in Supplementary Figure S1, which indicates that the effect size of PMX-DHP might be most influenced in the trial reported by Payen et al. [8]
Other possible sources for heterogeneity were investigated by meta-regression analyses. Figure 4A plots the log (odds ratio) of mortality in the PMX-DHP group against the mortality rate in the control group in individual trials. There was a significant negative relation (coefficient, −3.72; 95% CI, −5.46 to −1.98; p = 0.003), suggesting that the probability of a beneficial effect with PMX-DHP therapy increased with increasing risk of mortality in the control group. R2, which indicates the proportion of between-study variance, was 100%. Similarly, we also observed a negative relation between mortality reduction and APACHE II scores, although it did not reach statistical significance (Fig. 4B; coefficient, −0.199; 95% CI, −0.456 to 0.045; p = 0.097).

Meta-regression analysis. The weighted meta-regression line shows the relationship between the log risk ratio of mortality with PMX-DHP and the mortality rate with the control group (A) and the mean APACHE II score (B) in individual trials. The size of the symbols is inversely proportional to the variance of each trial. The negative slope of the regression line indicates a positive relationship between the probability of benefit of PMX-DHP therapy and increasing severity of illness. PMX-DHP = direct hemoperfusion with polymyxin B-immobilized fiber; APACHE II = Acute Physiology and Chronic Health Evaluation II.
We summarize the main findings including the quality of evidence as a GRADE evidence profile in Table 2. We detected no evidence of publication bias by assessing the funnel plot either visually (Supplementary Fig. S2) or statistically (p = 0.780 by Egger's linear regression test). For the other downgrade factors, we downgraded the quality of evidence by each one level for risk of bias and inconsistency. Hence, the overall quality of evidence across the studies of PMX-DHP therapy for all-cause mortality was rated as low.
Most of the studies are classified as unclear or high risk of bias (allocation, blinding; selection/detection, and other bias including study design).
Heterogeneity can be partly explained by the mortality rate in the control group. There is unexplained moderate heterogeneity (I2 of 52% and 60%) in both subgroups.
Egger's test indicated no publication bias.
The number of events is less than 300, and confidence intervals include possible harm with PMX-DHP.
PMX-DHP = direct hemoperfusion with polymyxin B-immobilized fiber; CI = confidence interval; RR = risk ratio; RCT = randomized controlled trial.
Effect on adverse events
Four RCTs enrolling 413 patients reported rates of hemoperfusion-related adverse events (Fig. 5, Supplementary Table S3). Adverse events reported by Vincent et al. [13] consisted of catheter-related infection and anemia, whereas those reported by Payen et al. [8] consisted of severe adverse events and hemorrhagic episodes. In two RCTs, no adverse events related to hemoperfusion treatment were reported [4,12]. Overall, there was no significant difference between groups in the risk of adverse events (RR, 1.04; 95% CI, 0.64–1.70; p = 0.87; I2 = 0%). In the other three RCTs, adverse events were demonstrated only in the PMX-DHP group (Supplementary Table S3). Cruz et al. [7] reported the occurrence of hemodynamic complications, including hypotension (one case, 1.5%) and tachycardia (two cases, 3%) in some patients.

Forest plot of the comparison of PMX-DHP versus conventional therapy for hemoperfusion-related adverse events. PMX-DHP = direct hemoperfusion with polymyxin B-immobilized fiber; M-H = Mantel-Haenszel; CI = confidence interval.
Regarding the quality of evidence of PMX-DHP for hemoperfusion-related adverse events, the 95% confidence interval around the risk ratio included appreciable benefit or harm, so we downgraded for serious imprecision. Taken together with the downgrade for serious risk of bias, we rated the quality of evidence of PMX-DHP therapy for adverse events as low.
Endotoxin concentrations
Five RCTs reported comparisons of serum endotoxin concentrations before and after PMX-DHP therapy (Supplementary Fig. S3). Among them, one trial described the median and range of endotoxin concentrations, and thus we estimated the mean and standard variance from the median and range using the method proposed by Hozo et al. [14]. The pooled standardized mean difference was 3.46 pg/mL (95% CI, 1.62–5.30; p < 0.001; I2 = 98.3%). This finding suggested that the concentrations of endotoxin were decreased substantially before PMX-DHP treatment, but this must be interpreted cautiously because of the high heterogeneity.
Discussion
In summary, this meta-analysis including seven RCTs demonstrated that PMX-DHP had a significant benefit (RR, 0.65; 95% CI, 0.47–0.89) on mortality in patients with sepsis/septic shock. The quality of evidence of PMX-DHP therapy for all-cause mortality was evaluated as low by the GRADE approach because of serious risk of bias and serious inconsistency. This rating of the quality of evidence means that further research is likely to have an important impact on our confidence in the estimate of effect and is likely to change that estimate.
Polymyxin B-immobilized fiber therapy is a method to remove endotoxins using an extracorporeal device with an adsorbent column containing polymyxin B that was developed as an adjunctive therapy for sepsis in Japan since the 1990s [15–19]. The main effect of polymyxin B is believed to be binding and neutralization of endotoxins, which plays an important role in the pathogenesis of sepsis and septic shock. Additionally, some cases were reported in which PMX-DHP therapy was believed to be effective in patients with septic shock induced by gram-positive bacteria without endotoxemia [20,21]. Thus, although the mechanism has not been fully elucidated, it is reasonable to speculate that binding, neutralization, and the reduction of other related components such as interleukin-6 [6,22,23], tumor necrosis factor-α [23,24], and neutrophil elastase [25] would be useful to improve outcome in such cases.
Between-trial heterogeneity was high in the present review (I2 = 72%), and both subgroup analyses and meta-regression analyses failed to identify completely the source of the heterogeneity. However, we indentified the source partially as being study venue (Japan versus European countries) and severity of illness (baseline mortality rate in the control group). In fact, four of the seven trials included in this review were carried out in Japan, for which mortality was generally high compared with that in the European countries. Additionally, the trials described in Japan were relatively dated. After the launch of the Surviving Sepsis Campaign, the mortality of sepsis/septic shock reportedly declined significantly [26]. Thus, these multiple factors might be involved with the heterogeneity observed across the trials.
Three previous meta-analyses have been published on the efficacy of PMX-DHP against sepsis. The first two reviews by Cruz et al. [27] and Qiu et al. [28], respectively, investigated the effect of PMX-DHP therapy on mortality, and the third review by Zhou et al. [29] investigated the efficacy of several types of blood purification techniques including PMX-DHP. One of the most important features that distinguished our analysis from these previous analyses was the articles eligible for review. We included two recent multi-center RCTs (the EUPHAS and ABDO-MIX trials) in our review and tried to update the previous evidence. Despite the divergence of eligible trials, the effect size of PMX-DHP therapy for mortality in our analysis (RR, 0.65; 95% CI, 0.47–0.89) was similar to those of the previous meta-analyses: Cruz et al. [27] (RR, 0.50; 95% CI, 0.37–0.68), Qiu et al. [28] (RR, 0.24; 95% CI, 0.16–0.38), and Zhou et al. [29] (RR, 0.57; 95% CI, 0.45-0.72).
The incidence of hemoperfusion-related adverse events in the PMX-DHP group in the present systematic review was not different from that in the control group (RR, 1.04; 95% CI, 0.64–1.70). However, because of insufficient data in the individual trials included in this analysis, well-designed RCTs are needed. The quality of evidence of PMX-DHP therapy for adverse events as evaluated by the GRADE approach was low as a result of serious risk of bias and serious imprecision. For the additional information that was not assessed by meta-analysis, few clinically important hemodynamic complications were reported among the included publications (1.5%–3%), suggesting that PMX-DHP therapy was generally well tolerated in clinical settings.
Consequently, from the viewpoint of the balance between benefit and harm, we suggest the use of PMX-DHP therapy as an option for sepsis management based on the assumed risk of death in patients with sepsis/septic shock. Currently, a large RCT called the EUPHRATES trial is underway in North America (clinicaltrials.gov ID NCT01046669). The trial will assess the efficacy of PMX-DHP in patients with septic shock and high levels of endotoxin activity defined by endotoxin activity assay. The results should shed light on this question.
A major strength of this analysis is our comprehensive search with no language limitations to identify RCTs. We performed a rigorous investigation of duplicate study populations by contacting the authors through interview or e-mail. In addition, this review is, to our knowledge, the first meta-analysis of PMX-DHP in patients with sepsis to use the GRADE approach, which offers a transparent system for rating the quality of evidence and for grading the strength of recommendations.
There are several limitations in our analysis. First, some of the included trials were of suboptimal quality: four of the seven trials were judged to have unclear risk of bias as to random sequence generation and allocation concealment. Also, all of the trials were open-blind trials. Second, most of the included trials were of small sample size and were conducted in a single center in Japan. Through our search strategy, we excluded seven other RCTs because of small sample size and other trials because of their low quality. However, the effect size of trials with and without these excluded trials showed little difference from that of the present analysis. Last, the insufficient number of included trials could lead to inaccurate evaluation of publication bias.
Conclusions
Putting these data into perspective, this systematic review found beneficial effects of PMX-DHP therapy on mortality (low quality of evidence) in patients with sepsis/septic shock. Additionally, an important finding of our analysis was that the beneficial effect of PMX-DHP therapy increased in accordance with the increasing severity of illness. Overall, however, because of the small numbers of included patients and the suboptimal risk of bias in most of the analyzed RCTs, further large rigorous RCTs are needed to confirm or refute these findings before the implications for practice are clear.
Footnotes
Acknowledgments
T.T. and Y.U. contributed equally to this article. T.T. and Y.U. performed data acquisition and analyses and drafted the manuscript. K.Y. conceived, designed, and coordinated the study, performed data acquisition and an analyses, and drafted the manuscript. A.M. had a major impact on the interpretation of data and critical appraisal of the manuscript. S.F. participated in data interpretation and helped to draft the manuscript. All authors read and approved the final manuscript.
We wish to express our gratitude to Drs. Nakamura and Suzuki, who provided valuable additional data.
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Author Disclosure Statement
The authors declare no sources of funding or conflicts of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.