
Abstract
Abstract
Background:
One of the most significant contributors to morbidity and death in patients with burns is infection, which accounts for 30%–75% of post-burn fatalities. Because of concerns for the development of antibiotic resistance in burn-related pathogens, the aims of this study were to identify antibiotic resistance trends for the four most common burn-related pathogens over a six-year period.
Patients and Methods:
The study used prospectively collected and de-identified aggregate data for all burn patients admitted to the burn unit between 2009 and 2014. The database query included patient demographics along with all data regarding cultures from any source (wound, sputum, urine, stool, blood), which included isolated pathogens and antibiotic resistance profiles. Profiles were then constructed using mean inhibitory concentration standards to determine whether each pathogen was susceptible (S), intermediate (I), or resistant (R) to each antibiotic. The aggregated data were then used to construct a heat map for the four most common pathogens and their resistance profiles over the six-year study period.
Results:
There were 368 patients with burns (248 with positive cultures, 120 with negative cultures) in this study. The positive culture group was significantly older (38 vs. 25 y, p < 0.001) and had longer hospitalizations (17 vs. 11 d, p < 0.01) compared with the negative group. Analysis of antibiotic resistance heat maps constructed for the four most commonly isolated pathogens (methicillin-sensitive Staphylococcus aureus, Enterococcus faecalis, methicillin-resistant S. aureus, Pseudomonas aeruginosa) indicated a lack of notable resistance patterns for any of the individual pathogens.
Conclusions:
Taken together, these results indicate that there are no discernible patterns of antibiotic resistance across time (six years) for the four most common burn-related pathogens. We conclude that antibiotic choice in burn patients based on previous in-hospital trends may be a flawed strategy. Emerging genomic technology to deliver point-of-care pathogen-specific antibiotic sensitivities via polymerase chain reaction may be needed to more appropriately guide antibiotic choice.
E
According to the American Burn Association's 2015 National Burn Repository, seven of the 10 most common burn-related complications are infectious in etiology. Consequently, infections comprise 77% of all post-burn complications, and they occur in 14%–28% of all burn patients.1,3 Studies investigating the impact of infections on post-burn mortality rates have estimated that infections account for 30%–75% of all fatalities in burn patients.4–14 These findings are compounded by the fact that 93% of hospitalized burn non-survivors had infectious complications with an 8.5- and 11-fold mortality risk increase in patients with burn wounds infected by multi-drug–resistant bacteria and fungi, respectively.3,15
While some clinicians argue that the current post-burn morbidity and deaths arising from infections cannot be reduced further because of the complex nature of burn injuries as well as other uncontrollable environmental factors, many providers believe that additional improvements in medical and surgical interventions may contribute substantially to reductions in burn-related infections. The aforementioned practices of early wound excision and grafting as well as utilization of topical antimicrobials has drastically reduced post-burn complications arising from infectious etiologies. Those interventions, however, were introduced more than three decades ago, and there has been notable stagnancy in burn care interventions addressing infections since that time. For that reason, further work is needed to understand and characterize the epidemiology of post-burn infections and the responsible pathogens to facilitate optimization of medical and surgical interventions that may further reduce complication rates.
The study hypothesis was that the four most common burn-related pathogens exhibit predictable antibiotic resistance trends that can be used to tailor antimicrobial stewardship practices. As a result, the aim of the present study was to identify the four most common pathogens cultured from patients with burns to construct antibiotic resistance profiles for each pathogen over a six-year period as a mechanism to inform more appropriate decision making with respect to antimicrobial choice.
Patients and Methods
Study population
We conducted an observational cohort study of consecutive patient admissions between January 2009 until December 2014 to the burn unit at the University of Chicago School of Medicine. The study was approved by the University of Chicago Institutional Review Board. Patient demographics, culture information, and antibiotic resistance data were used to determine resistance profiles. Data from this study were provided by the Clinical Research Data Warehouse, maintained by the Center for Research Informatics (CRI) at the University of Chicago. All patients who were admitted to the burn unit at the University of Chicago with positive cultures from any source were included in the culture analysis regardless of age, acuity, and total body surface area. There were no exclusion criteria. The demographics of the positive culture group were compared with those of the negative culture group—those who had cultures that ultimately returned no growth from any source.
Antimicrobial Stewardship Program (ASP)
The University of Chicago ASP is a hospital-wide effort to combat development of antimicrobial resistance (AMR). The ASP leadership comprises five infectious disease physicians with fellowships or research interests in AMR, two advanced practice nurses dedicated to data collection and analysis, and one doctor of pharmacy specializing in antimicrobial pharmacology. This multi-disciplinary committee evaluates all culture results for resistant pathogens to determine the most appropriate antibiotic therapy from the available options. They also perform antibiotic “time-outs” to re-evaluate the efficacy of chosen therapies at specific time intervals (i.e., 48 h after induction), which ensure appropriate coverage. They also maintain the hospital antibiogram and tailor empiric therapies relative to our hospital's overall resistance profiles for each pathogen.
Enteral and parenteral antibiotic agents are not started prophylactically in our burn patients because numerous randomized controlled trials have shown that prophylactic antibiotic agents are not effective at reducing incidence of or mortality rates associated with burn infections, and, in some cases, that practice contributes to increasing AMR pathogens in burn units.16,17 If there are clinical signs of local or systemic infection, broad-spectrum coverage is started after cultures are drawn and therapy is narrowed after culture speciation and sensitivities. The University of Chicago follows standard risk-modification practices aimed at reducing burn-related infections including early burn wound excisional debridement, topical antimicrobial agents (e.g., Silvadene, Sulfamylon) and/or temporary dressings (e.g., Xeroform, Mepilex, Biobrane, cadaveric skin grafts), and permanent coverage (e.g., autografted partial thickness mesh, partial thickness sheet, or full thickness sheet).
Pathogen ranking system
To identify the four most commonly cultured pathogens, a system was developed to calculate the frequency for each pathogen. A specific pathogen species (e.g. Staphylococcus aureus) was only counted once per hospital admission for the purposes of ranking determination. With this methodology, a patient who was in the burn unit for one month with multiple cultures identifying the same strain of S. aureus could only contribute one “count” toward the ranking system for S. aureus. This system was devised to eliminate any ranking bias that would otherwise afford unwarranted weight to pathogens cultured from patients with longer burn unit admissions.
Antibiotic resistance profiles
The culture results were collected from the CRI database and included the names of each isolated pathogen species as well as their tested antibiotic resistances. By applying the Clinical and Laboratory Standards Institute (CLSI) mean inhibitory concentration (MIC) standards, 18 antibiotic resistance strata for each pathogen were categorically defined as susceptible (S), intermediary (I), or resistant (R) to each of the 15 tested antibiotic agents. The tested antibiotic agents included cefepime, tobramycin, ceftazidime, levofloxacin, piperacillin-tazobactam, clindamycin, gentamicin, cefazolin, trimethoprim-sulfamethoxazole, rifampin, methicillin, ciprofloxacin, ampicillin, vancomycin, and erythromycin.
Each pathogen's respective antibiotic resistance ratio was determined by dividing the number of R counts for each antibiotic by the total number of culture susceptibility counts (S+I+R) for that specific antibiotic agent (equation below). The “resistance ratio” was converted to a color scale (vide infra) to create heat maps representing the percent resistance of the four common pathogens to each antibiotic over the six-year period. Increasing resistance [f(x): 0 → 1] correlated with an increasingly darker color (beige → maroon) as demonstrated in the color legends to the right of each respective resistance profile.
Resistance heat maps: Mathematical determination of color scale
Data analysis
All database query results were aggregated and subsequently analyzed in Microsoft Excel.
Results
Patient demographics
The patient demographics of the overall cohort are listed in Table 1. The study included 368 patients, 248 with positive cultures (i.e., wound, urine, feces, blood, sputum) and 120 without positive cultures. The average age for each group was statistically different (p < 0.01) at 38 years ±26 (standard deviation [SD]) and 25 years ±26 (SD), respectively. In addition, there were significantly more patients above 18 years of age in the positive culture (71%) versus the negative culture group (48%, p < 0.01). There was a significant difference between the positive and negative groups with respect to female gender (36%; 53%, p < 0.01) but not ethnicity: African American (63%; 64%), Caucasian (25%; 26%), and Other/unknown (12%; 10%). With respect to hospital length of stay, the positive culture group (17 d, 11–28 interquartile range [IQR]) had significantly longer hospitalizations compared with those with negative cultures (11 d, 7–14 IQR, p < 0.01).
SD = standard deviation; IQR = interquantile range.
p < 0.01
Culture data
A total of 974 cultures were analyzed for this study. From these cultures, 31 unique pathogen species were identified. After determining the number of unique encounters for each species, the top four most commonly encountered pathogens (Table 2) were determined to be methicillin-sensitive Staphylococcus aureus (MSSA: 64 encounters, 140 cultures), Enterococcus faecalis (41 encounters, 71 cultures), methicillin-resistant S. aureus (MRSA: 36 encounters, 124 cultures), and Pseudomonas aeruginosa (35 encounters, 113 cultures).
MSSA = methicillin-sensitive Staphylococcus aureus; MRSA = methicillin-resistant S. aureus.
Resistance profiles
The first graph (Fig. 1) displays the overall percentage of patients with R strains for each of the four pathogens with respect to culture year. In particular, each pathogen's yearly overall resistance was determined by the addition of all of the resistant values, regardless of antibiotic class, divided by the total number of available readings for that specific pathogen. The resulting graph showed no significant increasing or decreasing trend for any of the four pathogens that was sustained over the six years. MSSA (blue) and E. faecalis (red) showed minimal variation across the six-year study period whereas MRSA (green) exhibited an initial resistance increase from 2010 to 2011 that gradually diminished toward the 2009 value by 2014. The P. aeruginosa (purple) overall profile showed relatively lower levels of resistance (<15%) with intermittent periods of greater resistance in 2010 and 2012 and a subsequent return toward the initial resistance level by 2014.
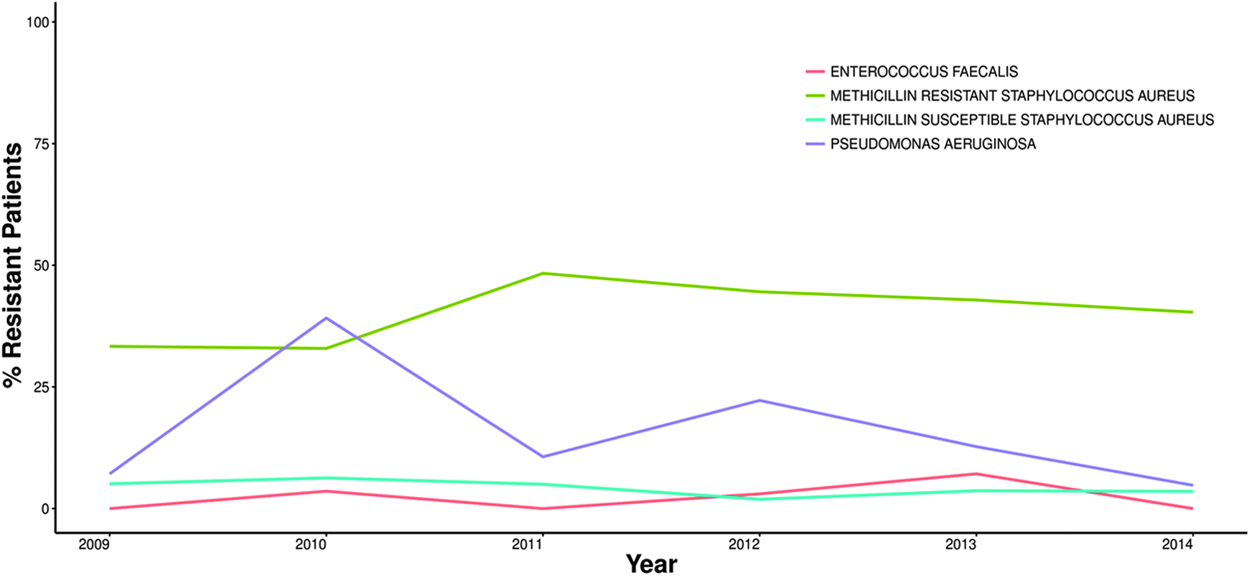
Overall antibiotic resistance trend by pathogen. The percentage of resistance patients includes any patient whose cultured pathogen(s) was resistant to one or more of the tested antibiotic agents. The color legend delineates each pathogen. Analysis reveals no discernible pattern of increasing or decreasing resistances over the six-year study period. Color image is available online at www.liebertpub.com/sur
After this initial analysis, a yearly resistance profile was created for each pathogen with respect to the 15 specific antibiotics. For MSSA, variable degrees of resistance were exhibited over the six years to clindamycin, ciprofloxacin, and erythromycin with no discernible increasing or decreasing trends (Fig. 2). With respect to clindamycin, the initial (2009) and final resistance (2014) were approximately 25% with periods of increased susceptibility in between those years. Ciprofloxacin resistance was present in 2010 (25% resistant), 2011 (30% resistant), and 2013 (20% resistant), although there was complete susceptibility during the remaining years. Resistance to erythromycin was initially 35% in 2009, increased to 50% in 2010, decreased to 10% during 2011 and 2012, and finally plateaued around 25% in 2014. Throughout the entire study period, MSSA was uniformly and completely susceptible to the remaining 12 antibiotic agents.

In the antibiotic resistance heat map for methicillin-sensitive Staphylococcus aureus, the color scale represents the ratio of resistance strains to all culture results for each antibiotic category. There were variable degrees of resistance over the six years to clindamycin, ciprofloxacin, and erythromycin with no discernible increasing or decreasing trends. Color image is available online at www.liebertpub.com/sur
For E. faecalis, it was broadly susceptible to all studied antibiotic agents throughout the study period except for ciprofloxacin and ampicillin (Fig. 3). Approximately 20% of cultured E. faecalis were resistant to ampicillin in 2010 with complete susceptibility during other years. In 2012, E. faecalis was 100% resistant to ciprofloxacin, 45% resistant in 2013, and completely susceptible in 2014 as well as all years before 2012. Throughout the entire study period, E. faecalis was uniformly and completely susceptible to the remaining 13 antibiotic agents.

In the antibiotic resistance heat map for Enterococcus faecalis, the color scale represents the ratio of resistance strains to all culture results for each antibiotic category. Throughout the study period, E. faecalis was broadly susceptible to all studied antibiotics except for ciprofloxacin and ampicillin, which displayed intermittent periods of resistance. Color image is available online at www.liebertpub.com/sur
Throughout the study period, MRSA displayed stochastic resistance to clindamycin, trimethoprim-sulfamethoxazole, ciprofloxacin, and erythromycin (Fig. 4). For clindamycin resistance, approximately 75% of cultured pathogens were resistant in 2011, but resistance gradually decreased to only 15% by 2014. The only year with observed resistance to trimethoprim-sulfamethoxazole was in 2013 (10%) with return to complete susceptibility in 2014. Ciprofloxacin started with complete susceptibility and increased to 80% resistance by 2012 with a subsequent drop to 55% by 2014. For erythromycin, complete resistance was present in 2009 and 2012 with variable but high resistance throughout the remainder of the study with a final resistance of 85%. Throughout the entire study period, MRSA was uniformly and completely susceptible to the remaining 10 antibiotics.

In the antibiotic resistance heat map for methicillin-resistant Staphylococcus aureus (MRSA), the color scale represents the ratio of resistance strains to all culture results for each antibiotic category. Throughout the six-year study period, MRSA displayed complete resistance to cefazolin and methicillin but stochastic resistance to clindamycin, trimethoprim-sulfamethoxazole, ciprofloxacin, and erythromycin. Color image is available online at www.liebertpub.com/sur
The P. aeruginosa resistance profile was notable for broad antibiotic resistance in 2010 and 2012 (Fig. 5). Cefepime resistance was initially highest in 2009 at 50% and gradually diminished to 0% resistance or complete susceptibility by 2014. Resistance to tobramycin was present in 2010 and 2014, but there was complete susceptibility during the other years. Ceftazidime resistance reached a peak in 2012 at 50%, but it then eventually returned to complete susceptibility. Levofloxacin resistance was highest in 2010 at 65%, intermittently fluctuated, and finally settled at 5%. Similar trends were present for gentamicin and ciprofloxacin with maximum resistance during 2010 at 30% and 45% with an eventual decrease to 2.5% and 5% by 2014, respectively. Resistance to piperacillin-tazobactam was greatest in 2010 with a subsequently stochastic trend and eventual return to complete susceptibility by 2014. Throughout the entire six-year period, P. aeruginosa was both uniformly and completely susceptible to the remaining eight antibiotic agents.
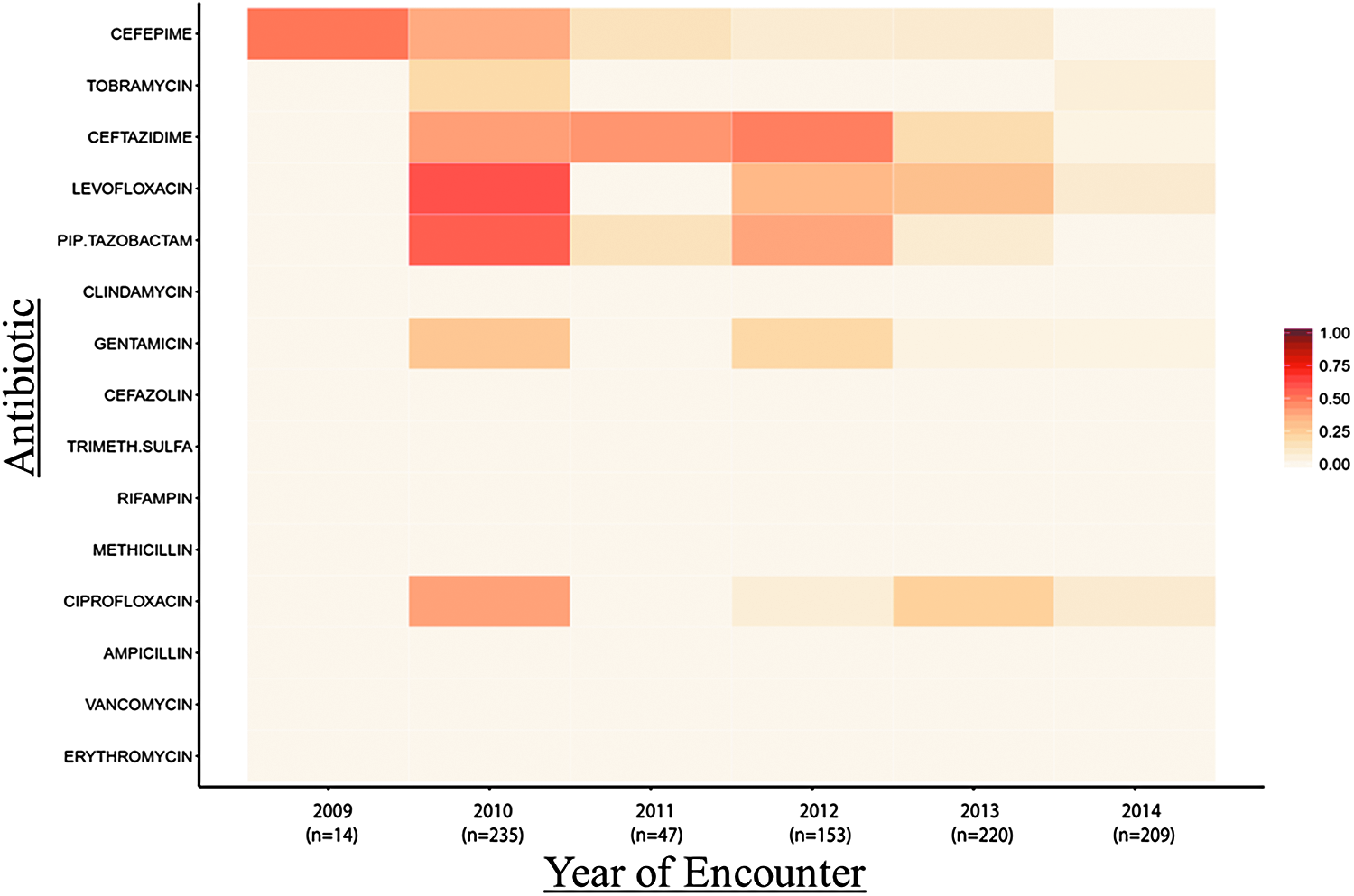
In the antibiotic resistance heat map for Pseudomonas aeruginosa, the color scale represents the ratio of resistance strains to all culture results for each antibiotic category. There were variable periods of resistance to cefepime, tobramycin, ceftazidime, levofloxacin, piperacillin-tazobactam, gentamicin, and ciprofloxacin. Color image is available online at www.liebertpub.com/sur
Discussion
One of the leading causes of morbidity and death in burn patients—even in countries with state-of-the-art burn care—is infection. Infections account for 77% of all post-burn complications, and some degree of infection-related sequelae develop in 14%–28% of all burn patients during their hospitalizations.1,3 The significant impact of infections in the burn population has been further substantiated by studies determining that infections may account for 30%–75% of all fatalities in patients with burns.4–14
Patients who have burn injury are frequently immunocompromised as a result of the pathophysiologic response to their injuries and the effects of numerous interventions such as early wound excision with coverage as well as use of topical antimicrobial agents. Despite the ability of these therapies to significantly reduce the observed rates of burn infections by as much as a factor of six in some retrospective studies, current interventions are not preventative uniformly, and the pervasive morbidity and death burden from infectious complications after burn injury still remains exceptionally high for this vulnerable patient population.19–21
During the six-year study period, the four most commonly identified pathogens were MSSA (19.6% of patients), E. faecalis (12.5%), MRSA (11.0%), and P. aeruginosa (10.7%). Numerous previous studies examining bacteriologic incidence in burn patients have similarly identified all of the aforementioned bacteria as frequent isolates.4,7,14,22–29 The heterogeneity with respect to relative frequencies and resistance profiles across studies supports the concept of injury location, community, and region-dependent influences on the overall patient microbiome and its pathogenicity. As a result, it is particularly valuable for each burn center or region to perform similar studies to identify the unique variations with respect to microbiome composition as well as their variable resistance profiles.4,14,23,29,30
It is equally important, however, that investigators consider focusing on single pathogens and their resistance profiles to the entire microbiome community and its resistome or collective antimicrobial resistance genes. For example, understanding that the entire microbial community that colonizes a specific patient possesses significant potential to influence horizontal gene transfer through mobile-genetic elements needs to be considered. As a result of this process, a pathogen's antibiotic resistance can be acquired either from the commensal flora through plasmid-mediated processes or intrinsically through deoxyribonucleic acid mutagenesis.31–34 Broadening our scope of analysis to the microbial community and its resistome as a whole will improve our ability to identify patients at greatest risk for the development of multi-drug–resistant organisms and the subsequent clinical sequelae. As technology to sequence bacterial genes develops into point-of-care diagnostic tools, both investigators and practicing clinicians will be able to choose antibiotic agents with less empiricism and more molecular precision.
When looking at the broad resistance of the four pathogens (Fig. 1), there were no sustained increasing or decreasing trends with respect to the overall percentage of isolated pathogens with resistant phenotypes. The observed stochasticity in overall resistance patterns is possibly the sequela of yearly and community-dependent variations in pathogens, such that a given patient's time of admission as well as neighborhood of origin alter the microbial composition as well as the resistance profiles. As a result, it is hard to clarify the role of changing antimicrobial stewardship policies on the overall pathogen resistance profiles from year-to-year.
Another possible explanation for the seemingly random resistance patterns over the six years is that more complex methods of dynamic mathematical modeling, such as chaos theory, are required to address the high complexity of variable responses by clinicians to individualized patient scenarios. 35 For example, while there was no clearly discernible increasing or decreasing resistance trend for P. aeruginosa that was sustained throughout the study period, the day-to-day clinical decisions regarding interpretation of and response to culture results may vary significantly. In other words, it is possible that the providers initially treated the broadly susceptible P. aeruginosa with common antibiotics until resistance developed and required a switch to different therapies.
To address any meaningful conclusions from the antibiotic-specific resistance profiles for each pathogen, the four bacteria will be addressed in turn. For MSSA (Fig. 2), variable degrees of resistance were exhibited to clindamycin, ciprofloxacin, and erythromycin with no discernible increasing or decreasing trends. The preferred treatments for such infections—staphylococcal penicillins and cephalosporins—remained effective throughout the study period, and, therefore, the observed resistances had no appreciable impact on antimicrobial stewardship practices.
For E. faecalis (Fig. 3), it was susceptible to all but two of the studied antibiotics—ciprofloxacin and ampicillin. While some resistance to the commonly used ampicillin was present during 2010, susceptibility to aminoglycosides and cephalosporins allowed for continued satisfactory coverage without significant influence on antimicrobial stewardship policies.
As might be predicted, MRSA (Fig. 4) displayed complete and sustained resistance to cefazolin and methicillin with relatively high resistance to erythromycin. The stochastic resistance to clindamycin and trimethoprim-sulfamethoxazole—frequent first-line agents for enteral coverage—was not sustained and relatively low throughout the study. The continued susceptibility to vancomycin and cephalosporins likely resulted in the aforementioned resistances not having a significant impact on patient care.
With respect to the P. aeruginosa resistance profile, it was notable for relatively broad antibiotic resistance in 2010 and 2012 (Fig. 5) with interspersed periods of increased resistance to anti-pseudomonals, fluoroquinolones, and cephalosporins. Despite significant resistance to first-line agents—piperacillin-tazobactam, cephalosporins, fluoroquinolones, and aminoglycosides—in 2010 and 2012, there was no appreciable increase in overall mortality rates for culture positive burn patients during that time. Although there was no gross correlation between death and antimicrobial resistance, further studies with higher granularity data sets are required to fully assess this apparent contradiction to the classical observation that resistant strains of P. aeruginosa are the most commonly associated pathogens in infectious-related death in patients with burns.14,15,22,36
This disconnect between increased resistance and observed mortality rates alludes to the differential phenotypes of resistance and virulence. In nature, it has been proposed that there is an evolutionary trade-off between expression of resistance and virulence genes.37–39 The hypothesized explanation for this finding is that highly resistant organisms rarely need to compete with other microbes in the local environment, and, as a result, infrequently employ expression of virulence genes to augment acquisition of host or environmental resources. Numerous studies have shown a direct reduction in virulence capacities with respect to the expression of resistance genes.37,38,40–43 Despite these findings, the hospital environment exerts its own evolutionary pressures leading to a form of unnatural selection that may cause evolutionary divergence, and such processes have already been observed in numerous studies.44–48 Because of the currently conflicting evidence and pathogen-dependent variability, further studies are warranted to elucidate the complex interactions between resistance and virulence genes as well as the clinically relevant phenotypes.
The present study is limited because of its retrospective nature and utilization of CLSI MIC standards 18 to categorically stratify pathogens as S, I, or R. The reliance on categorical determinations of resistance underscores the recognition that MIC creep, or subtle but significant increases in antibiotic resistance over time, may be missed by our study design. Further analysis of those pathogens categorized as intermediate resistance may better address the concern of MIC creep and the potentially valuable trends in that portion of the microbial sub-population. Another limitation to be addressed in future studies is the single center design from which regional influences on pathogen epidemiology and resistance profiles may be missed or over-represented by our unique patient population.
It is important to mention that culture positivity and clinical infection are not synonymous entities, even though such an assumption is made by many medical practitioners. As a result, cultures were only performed on specimens from burn patients who manifested signs of local and/or systemic infection. This study methodology significantly reduced the incidence of cases in which positive cultures were obtained for those not infected clinically. This culturing practice was implemented alongside measures that ensured materials for cultures were acquired before antibiotic administration to minimize the converse situation in which those with negative cultures had clinically significant infection. Because of the aforementioned practices, the authors believe that the study design ensures that the two dissonant scenarios do not significantly impact our conclusions.
Conclusion
The stochastic resistance patterns for the four identified pathogens provide meaningful insight into the complexity behind developing antibiotic resistance. While other studies have shown progressive and sustained increases in resistance to standard first-line agents, resistance patterns were entirely stochastic in our patient population. The clinical significance of this temporo-spatial variance is that we cannot reliably predict resistance patterns with enough statistical certainty to appropriately alter current empiric antimicrobial therapies. The current method of antimicrobial coverage uses broad-spectrum empiric therapy until speciation and sensitivities are acquired from cultures that often require 48–96 hours for completion. Our study shows that for certain pathogens (i.e., Pseudomonas) there were specific years with high resistance to the classic empiric coverage (i.e., piperacillin-tazobactam), which would subsequently render patients insufficiently covered until culture results provided susceptibilities.
In addition, clinicians must remain cognizant of the fact that antimicrobial resistance (AMR) trends may not translate across geographic regions, cities, or even different units within a single hospital because there are so many unpredictable factors that can influence a specific patient's microbiome and resistome. Addressing this issue requires faster methods of pathogen and resistance identification to circumvent the need for extended periods of empiric therapy that, in many cases, may be insufficient and contribute to increased morbidity and death.
Because of the observed AMR stochasticity, this study highlights the importance of pursuing research related to emerging point-of-care assays (e.g., polymerase chain reaction probes, procalcitonin, peptide nucleic acid fluorescence in situ hybridization, and Matrix Assisted Laser Desorption/Ionization – Time of Flight [MALDI-TOF] mass spectrometry). Incorporating these technologies into clinical practice will facilitate rapid identification of patient-specific antibiotic sensitivities within hours as opposed to the days required by standard culture methods, and it will enhance our capacity to precisely and promptly deliver effective antibiotic therapies.
Footnotes
Author Disclosure Statement
No competing financial interests exist.