
Abstract
Abstract
Background:
Pressure irrigation of surgical incisions and traumatic wounds is commonly used to prevent infections. Commercial pressure irrigation devices have proliferated rapidly, but scientific validation of clinical benefit or appropriate use remains uncertain.
Methods:
The published experimental and clinical investigations of pressure irrigation have been reviewed since the introduction of the Waterpik device in 1967 to identify the evidence for use to prevent soft tissue infections associated with injury wounds or surgical incisions.
Results:
The published literature favors low pressure irrigation between 5–15 pounds/square inch (psi) for experimental removal of bacteria from contaminated tissues, with pressures higher being associated with soft tissue and bone injury. No experimental or clinical data have demonstrated improved benefit from pulsed over continuous lavage. Clinical studies have been very heterogeneous in patient populations and study design; meta-analysis was not feasible. High-risk abdominal operations may have lower surgical site infection rates with pressure irrigation. Pressure irrigation in fractures and joint replacement surgery has shown mixed results. The largest multi-center randomized trial showed no benefit of pulsed (8–10 psi) lavage over conventional continuous gravity irrigation of open fractures.
Conclusions:
Experimental studies have shown effective removal of bacteria and contamination, but with a potential risk of tissue injury or displacement of contamination deeper into the soft tissues. Rigorous clinical documentation has not validated the optimum flow or pressure characteristics of pressure lavage in clinical practice. There is need for randomized clinical trials to validate pressure lavage in the prevention of infections in soft tissue injuries or high-risk surgical incisions.
I
In the 1960s, Mattingly (engineer) and Moyer (dentist) launched the Aqua Tech Company, and in 1967 patented the Waterpik Oral Irrigator as a device that was designed for oral hygiene to remove food debris and perhaps remove bacteria that conventional mouth rinse would not remove [6]. The Waterpik delivered pulsed and pressurized water irrigation to the teeth and gums. It remains a recognized and effective device for preventive dental care.
Shortly after the introduction of the Waterpik, interest developed about the potential merits of pressure irrigation for use in the management of contaminated traumatic wounds and surgical incisions. The interest created by experimental studies resulted in the use of pressure irrigation for contaminated and infected wounds. It has been recommended as effective and safe in the prevention and management of soft tissue infections [7].
Over the last 40 years, many commercial pressure irrigation devices have been introduced into surgical practice with the express purpose of removing debris and bacteria from the contaminated wound or incision (Table 1). Many questions about pressure irrigation have not been answered, however, including whether it is of any value over conventional irrigation in the management of surgical incisions. This presentation will review the experimental and clinical evidence on the use of pressure irrigation in the prevention of soft tissue and surgical site infections.
The listing does not likely identify all manufacturers of devices that are available.
Theory of Pressure Irrigation
To understand the application of pressure irrigation, it is necessary to understand the pathobiology of surgical incisions and traumatic wounds. With the disruption of skin and the subcutaneous tissues from either injury or the surgical incision, numerous activators of the innate immune response are released at the site. The activators include tissue factor and other danger-associated molecules from cellular and tissue disruption [8]. These activator events initiate inflammation via coagulation cascade cleavage products, platelet granule contents, bradykinin synthesis from the constitutively present pre-kallikrein, mast cell vasoactive peptides, and complement activation products.
There are two major effector phases of inflammation that have relevance to this discussion of pressure lavage. First, the vasoactive phase results in microcirculatory vasodilation, local increased microvascular permeability, and edema formation with extravasation of plasma proteins. Extravasated fibrinogen is converted to fibrin, which is precipitated within the injured tissues, especially on the exposed surface of the wound tissues (Fig. 1A). This fibrin coat can be viewed as physiologic coverage of the wound tissues to avoid further contamination from environmental pathogens. Second, a generous number of opsonic proteins are released into the injured tissues from the vasoactive phase to launch the infiltration of the injured area with phagocytic cells. Thus, the injured or incised tissue has a fibrin matrix over the exposed surface.

This depiction of a surgical incision demonstrates the fibrin matrix that develops on the incision surface before closure. This is a product of the vascular phase of human inflammation that begins immediately after tissue injury.
For the surgical incision or traumatic wound, the open exposure to the environment permits continuation of the fibrin deposition process and makes the duration of the open wound a variable in the number of bacterial pathogens that will contaminate the fibrin surface. The fibrin coated wound surface and tissue interstices likely contain most of the bacterial contaminates from the injury or the incision. The density of the fibrin likely impedes the infiltration of leukocytes into this matrix for removal of bacterial contaminants (Fig. 1B) [9]. Conventional gravity irrigation regardless of the volume of irrigation solution used that is delivered from a surgical basin or other low-pressure device is generally not thought to remove this fibrin surface nor the imbedded bacteria, foreign body contaminants, or dead surface cells.
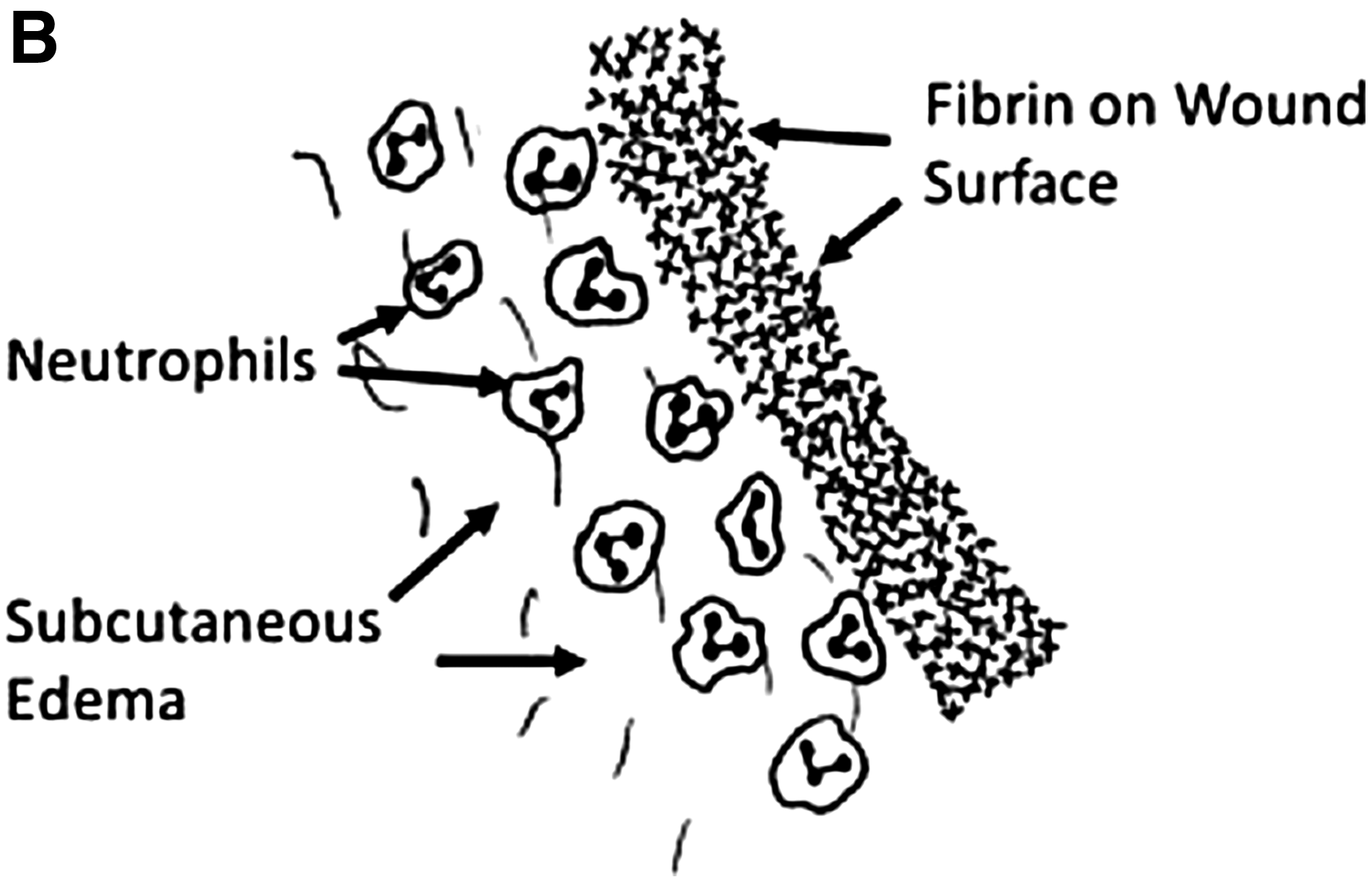
This depiction of the surgical incision demonstrates the penetration of neutrophils into the subcutaneous edema immediately beneath the fibrin matrix on the wound interface. As is illustrated, neutrophils poorly penetrate the mature fibrin matrix.
The theory of pressure lavage is that the force of the irrigation stream will strip the fibrin and its associated bacteria from the wounded surface. Pressure irrigation may overcome microbial adhesion mechanisms associated with bacteria that are bound to the surface of the host tissues of the wound surface. Removal of particulate matter and clot in traumatic wounds would be yet another benefit. The pressure stream that is perpendicular to the target surface for irrigation will potentially drive fibrin, contaminants, and foreign bodies deeper into the area of the wound tissue (Fig. 2A). This displacement of microbes and particulate matter in combination with pressure-associated tissue damage from the perpendicular force may enhance the risk for infection.

This depicts the consequences of a perpendicular delivery of pressure irrigation to the wound surface. Fractured fibrin matrix with accompanying bacteria may be driven deeper into the tissues.
An important consideration in pressure irrigation is that the “jet stream” of irrigation solution should be at an angle to the target surface so that sheer forces will functionally strip the fibrin and other debris off the wound surface (Fig. 2B). Thus, considerations of the force of the irrigation, that is usually expressed as pounds/square inch (psi), and the angle of delivery for the pressure stream become important variables in attempting to understand the differences in outcomes in the published literature. Still other variables for consideration are the volume of the irrigation solution and whether pressure irrigation is pulsed or continuous.
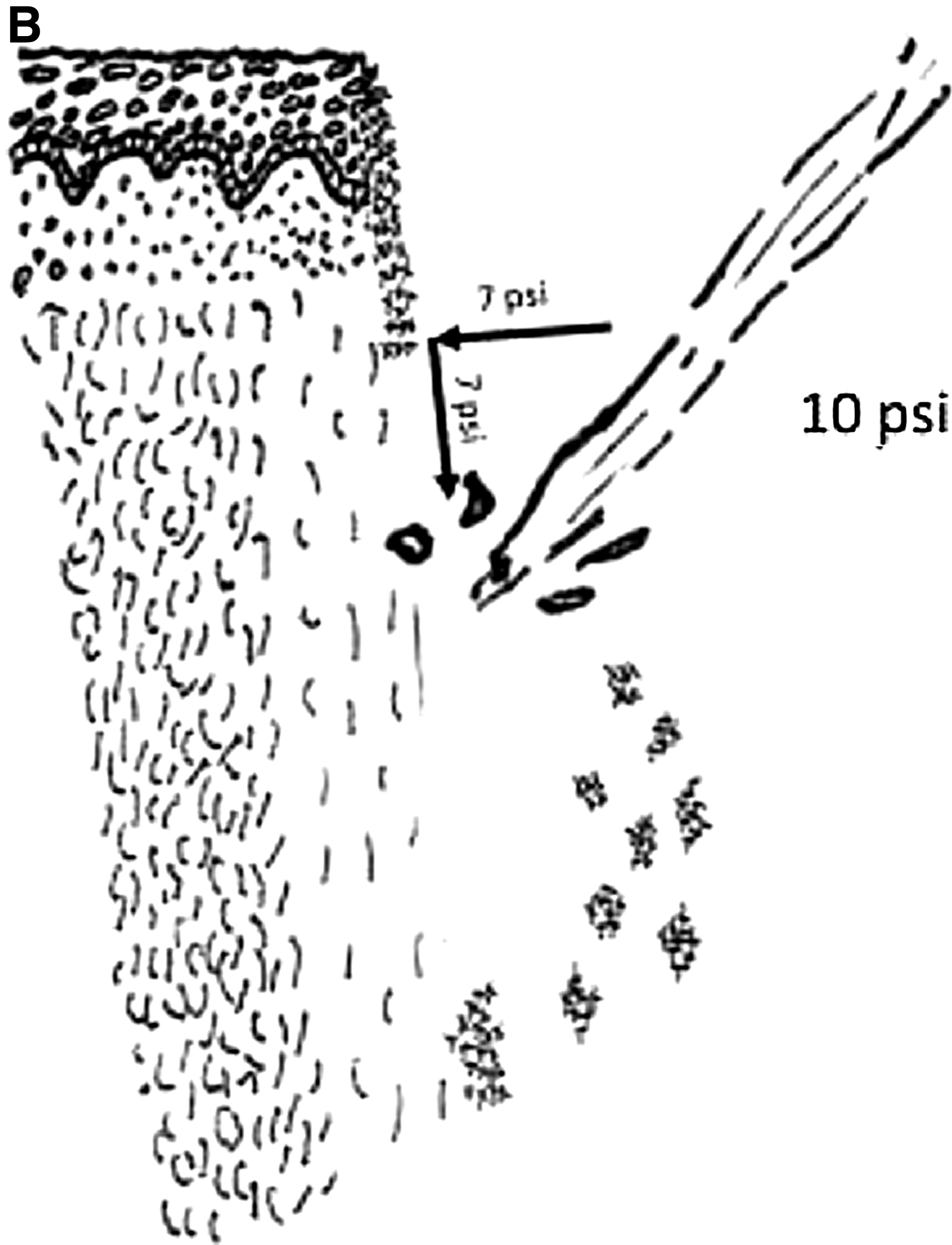
This depicts pressure irrigation delivered at a 45-degree angle. The 10 pounds per square inch (psi) force of the irrigation stream can be illustrated by vector physics to have a reduced perpendicular force (7 psi) to the wound but also to have a sheer force (7 psi) that will remove the bacteria-laden fibrin matrix.
Experimental Studies
Experimental studies have consistently demonstrated the promise of pressure irrigation in the prevention of infection. Madden et al. [10] in 1971 studied acute rabbit wounds contaminated with Staphylococcus aureus. Pulsatile versus continuous pressure irrigation was evaluated at 0.5, 10, and 25 psi. They used quantitative cultures to define the effectiveness of the irrigation method. Increasing pressure proved to be more effective in these acute experiments in removing bacteria. In this study, pulsatile irrigation was less effective than continuous irrigation. Also in 1971, Stewart et al. [11] studied pulsed versus continuous irrigation at 60 psi in contaminated experimental wounds and found the two methods to be similar in bacterial removal. Green et al. [12] performed similar experiments in contaminating experimental wounds with iron filings and found equal effectiveness of pulsed versus continuous irrigation at 60 psi in the removal of the particulate matter.
Gross et al. [13] in 1972 used a masseter muscle incision in rats but also crushed muscle tissue and introduced moist soil at the time of bacterial contamination to simulate a traumatic injury. They used Staphylococcus aureus, Klebsiella pneumoniae, Proteus mirabilis, and Pseudomonas aeruginosa each in separate experiments. They used bulb syringe irrigation and compared it with 70 psi pulsed irrigation. Wounds were irrigated 30 minutes after contamination and then closed. Animals were sacrificed at 4, 6, 8, 10, and 12 days after wound closure. Pulsed lavage was far more effective than bulb syringe irrigation in the removal of bacteria and particulate contamination. Continuous pressure irrigation was not studied. Similarly, Hamer et al. [14] found superior removal of bacteria with pulsed lavage (50 psi) compared with low pressure irrigation in bacterial contamination of experimental wounds in rats.
In perhaps the most widely quoted experimental study of pulsed irrigation, Rodeheaver et al. [15] studied incisions on the back of guinea pigs that were contaminated with colloidal clay and S. aureus to simulate dirty traumatic wounds. One hour after contamination, pulsed irrigation was performed with 100 mL of saline at 1, 5, 10, and 15 psi. They identified better particle removal and lower infection rates in animals with 10–15 psi. They extended the studies by using different chelating agents, flocculents, dispersants, and surfactants and found no benefit of adding any of these substances to the saline irrigation. They found no benefit by increasing irrigation volumes at each pressure level to more than 100 mL. Despite the clinical practice of using very large volumes of irrigation solution in contaminated wounds, there remains no experimental or clinical evidence that increased volumes of irrigation with pressure devices reduces contamination or subsequent infections.
Brown et al. [16] performed an extensive study of rat incisions contaminated with 109 Escherichia coli. The wounds were irrigated with saline at gravity pressure, bulb syringe pressures, and at 50 psi with an adapted Waterpik device. Wounds were cultured 30 minutes after contamination and closed. Animals were sacrificed and wounds were cultured at 3, 7, and 10 days later. Pulsatile high-pressure irrigation was most effective in reducing bacterial colon counts, but was not compared with continuous lavage at the same pressures. The experiment was repeated with ischemic muscle and sterile garden soil contamination in addition to the contamination with E. coli. This repeat series of experiments demonstrated the same benefit for pressure irrigation. The results of this study were confirmed in more recent experimental studies where high-pressure irrigation was most effective in the removal of bacteria from soft tissue injuries with exposed bone, especially when the wound irrigation was delayed by 6 hours [17].
In 1976, Wheeler et al. [18] conducted studies to evaluate whether pressure lavage displaced bacteria deeper into the tissue. In vivo experimental porcine wounds were contaminated with Serratia marsescens. They evaluated no irrigation, 8 psi with a piston syringe, and 70 psi with pulsed lavage. No displaced bacteria were observed in any groups, but lavage fluid was identified at 3 ± 1 mm into the tissue with the piston syringe, and lavage fluid was 14 ± 1 mm into the issue with the pulsed lavage. Wound infections were equivalent in both pressure irrigation groups but were also five times more frequent than in wounds with no irrigation. The authors concluded that bacteria were not displaced by pressure irrigation, but that tissue injury and inflammation from the process increased infection rates.
Hassinger et al. [19] performed experiments to evaluate potential deleterious effects of pressure irrigation. Using ex-vivo ovine muscle, the tissue was contaminated with fluorescent S. aureus. Three minutes after contamination, experimental muscle was lavaged with 200 mL at pressures of 3 psi and compared with higher pressures of 6–19 psi. Irrigation was delivered parallel and perpendicular to the muscle fibers in separate experiments. Fluorescent microscopy was used to measure depth and colony counts in controls and all irrigation groups. The results demonstrated better removal of bacteria by the low-pressure method, but high-pressure irrigation resulted in displaced bacteria to a depth of 2–7 mm into the tissue. No difference was identified based on the direction of the irrigation stream with respect to the muscle fiber orientation. These studies confirmed the observations that high-pressure irrigation caused soft tissue injury [20].
Experiments with bovine cancellous bone that was contaminated with rock dust demonstrated that pulsed lavage at 6–19 psi resulted in better removal of the foreign contamination than low lower pressure irrigation but also was associated with more bone damage [21]. The authors concluded than pulsed lavage would drive contaminants deeper into the tissues and create greater bone structural damage that might lead to poorer healing. Their observations of structural bone injury and potentially impaired healing confirmed earlier observations by earlier authors [22–25]. One experimental study identified histologic replacement of osteoblasts by adipocytes after high-pressure irrigation [26].
An examination of all experimental studies generally leads to the conclusion that higher pressure appears to be more effective in the removal of bacterial contamination and particulate foreign matter than lower pressures. High-pressure irrigation more than 15 psi, however, likewise causes both soft tissue and bone injury. The force of higher-pressure irrigation may enhance cement incorporation into bone and may be a positive feature for the placement of orthopedic prostheses [27–29]. The different pressure devices that have been used in the experimental studies have varied from homespun delivery systems to commercial pressure devices. Studies to evaluate the optimum removal of bacteria and foreign material versus the magnitude and potential damage of the pressure that has been applied leaves a void in knowing the best pressure for clinical application.
Clinical Studies
Pulse lavage systems are commonly used for open fractures, contaminated soft tissue injuries, and even for the management of contaminated or infected visceral spaces. Specifications of the appropriate pressure, fluid composition, or volume of irrigation solution to be employed remain largely undefined, however. Many commercial devices are sold for pulse lavage in clinical surgical procedures (Table 1), but accurate specifications of the actual pressure that is delivered by these systems are quite variable. The number of randomized trials is sparse and leaves uncertainty about the appropriateness of this technology.
Open fractures
Pressure irrigation of contaminated wounds has been applied most commonly in patients with open fractures. The consequences of infections, mal-union, and non-union after open fractures have led to the common use of pressure irrigation to remove microbial and particulate contamination that is responsible for these complications. Potential benefits of this preventive strategy have largely been driven by experimental studies, as noted above, and clinical evidence to support this practice has been limited.
Previous surveys have demonstrated that orthopedic surgeons preferred pressure irrigation of open fractures, although there appears to be ambivalence about what constitutes high-pressure versus low-pressure irrigation of the wound [30,31]. While the addition of soap to the irrigation has some clinical evidence that suggests benefit for open fracture irrigation [32], most surgeons chose only saline irrigation with pressure irrigation. The consensus in the cited surveys indicated a need for clinical evidence to guide whether pressure irrigation in open fractures is of value, what pressure should be used, and whether the addition of antimicrobial agents or soaps to the irrigation solution are of any merit. To address the absence of data, the Fluid Lavage of Open Wounds (FLOW) investigators were organized to test whether saline versus soap solution and whether high pressure versus low pressure versus gravity irrigation was best in the management of open fractures [33].
A preliminary report of 89 randomized patients with open fractures by the FLOW investigators compared irrigation with castile soap added to physiologic saline versus physiologic saline alone, and high pressure (25–30 psi) versus low pressure (6–10 psi) [34]. The follow-up was for one year after injury. Infections, all wound healing problems, non-union, and functional status of patients were the outcomes of interest. Results indicated no difference in outcomes when the castile soap versus saline irrigation groups were compared (p = 0.52). Low-pressure irrigation had apparently fewer primary adverse outcome events (19%) than did the high-pressure group (28%) in the one-year follow-up. This apparent difference did not achieve statistical significance (p = 0.17) but given the small study population. the results raised the expectation that a larger study sample would demonstrate benefit.
The FLOW Investigators have recently completed a multi-institutional, randomization of 2,447 evaluable patients to receive either saline irrigation or saline plus castile soap and saline [35]. A second randomization of these same patients to high pressure, low pressure, or gravity pressure irrigation was performed to complete a 2 × 3 factorial matrix where each patient was identified in one of six unique irrigation solution/pressure treatment groups. Adverse outcomes of interest were re-operations for infection or poor tissue/bone healing at the primary wound of the fracture site. Follow-up was for 12 months after the index operation. The addition of castile soap to the saline irrigation resulted in a significantly increased rate (p < 0.01) of re-operation (14.8%) compared with the saline only group (11.6%). There were no statistically significant differences among the three groups of high-pressure (13.2%), low-pressure (12.7%), or gravity-pressure (13.7%) irrigation. For open fracture management, the results of this large multi-center randomized trial demonstrated that saline irrigation alone was best and that increased-pressure irrigation offered no benefit in 12-month re-operation rates.
Hip fractures and arthroplasty
Hip fractures from falls and direct trauma are associated with significant complications of infection after arthroplasty [36]. This patient population tends to be elderly patients who are prone to complications, especially infections. The consequences of arthroplasty infection in this population are particularly severe. Pressure irrigation has been proposed as a method to reduce infections.
Hargrove et al. [37] performed a randomized clinical trial of pressure irrigation versus convention irrigation in 356 hip fracture patients undergoing hip hemiarthroplasty. Two liters of saline irrigation was used in each arm of the study without any antimicrobial agents added to the irrigation solution. Neither the specific pressure nor the specific irrigation device was identified. The use or type of preventive systemic antibiotic agents in the two treatment groups was not specified. The results of the study identified a 15.6% superficial and deep infection rate in the control group and a 5.5% rate in the patients undergoing pulse irrigation (p < 0.002). A criticism of this study has been that the overall infection rates among the patients in the study were very high.
Spine operations
Ahn et al. [38] studied 79 consecutive patients who underwent spine operations and had saline irrigation of the incision with a bulb syringe. The next 59 spine cases had saline pulsed irrigation (17 psi). All sites were cultured at the conclusion of the procedure. Bacteria were more commonly cultured in the bulb irrigation group (p = 0.05) from the posterior muscle layer than were cultured in the pulsed irrigation group. No differences in cultures were observed from the intervertebral disc space. No differences in clinical infections at the surgical site were identified.
Abdominal operations
Cervantes-Sánchez et al. [39] studied complicated appendicectomy incisions in patients with gangrene, abscess, or diffuse peritonitis. Patients were randomized to receive syringe pressure saline irrigation of the surgical site at closure versus patients with no irrigation for the control group. There were 29 (72.5%) infections among 40 patients in the control group versus 9 of 55 (16.3%) patients in the syringe pressure group.
Nikfarjam et al. [40] performed a retrospective study of patients undergoing a heterogeneous group of abdominal surgical procedures that were greater than four-hours duration. Pulse lavage (<15 psi) with saline was compared with conventional saline irrigation. The mean length of the operative procedures was eight hours. The 34 standard irrigation patients had 11 surgical site infections (32%), while four infections were seen in the 42 pulse lavage patients (10%). This statistically significant difference in surgical site infections (p < 0.019) was not associated with excess antibiotic administration beyond 24 hours after the operation (p < 0.839) nor was it associated with any differences in lengths of stay between the patients in the two groups (p < 0.255).
After this retrospective study, Nikfarjam et al. [41] performed a prospective randomized trial of pressure lavage (<15 psi) versus conventional saline irrigation in 128 patients undergoing hepatobiliary and pancreatic procedures. Surgical site infection rates were 19% (12/62) in the standard irrigation group but only 6% (4/66) in the pressure irrigation group. As was observed in the original retrospective trial, no difference was identified in the need for antibiotic administration beyond 24 hours, inpatient length-of-stay, or in re-admission rates after discharge from the hospital.
Soft tissue
Shetty et al. [42] studied the use of pressure lavage (10–15 psi) in a randomized clinical study of 30 cases of chronic extremity wounds that were compared with conventional irrigation with povidone-iodine dressings. Once randomized, each patient received the designed irrigation treatment daily. The area of the wound surface was measured daily and the end point was complete healing of the wound or acceptability of the wound for skin grafting. Patients receiving pulse lavage therapy reached the acceptable clinical end point at 6.3 ± 1.1 days while those in the conventional irrigation group required 13 ± 2.5 days (p < 0.001).
Discussion
Despite the widespread use of pressure irrigation both for the prevention and management of infection, there remains a paucity of quality evidence to support the practice. Experimental studies show benefit in the elimination of bacteria and foreign bodies in soft tissue wounds. There is also evidence, however, of tissue injury and the potential displacement of bacteria deep into the irrigated soft tissues that appears to correlate with the magnitude of the pressure that is used. Clinical trials are very limited in number, and in the one area where pressure irrigation is most commonly used (open fractures), there is a large multi-center randomized clinical trial showing no benefit to either high or low pressure irrigation when compared with gravity lavage.
Conclusion
The case for or against pressure irrigation is certainly complicated by uncertainty about continuous versus pulsed irrigation, the appropriate pressure to be used, the appropriate volume to be used, the angle of pressurized irrigation that is introduced into the wound, and whether pressure lavage can be enhanced by the addition of antimicrobial agents to the solution. As has been emphasized recently [43], one can only depend on expert opinion about the use of wound irrigation strategies. Despite the extensive commercialization of pressure irrigation devices, the best recommendation that can be made now is that the evidence is of low quality and that randomized clinical trials are needed.
Footnotes
Author Disclosure Statement
Dr. Fry is a speaker and consultant to the IrriMax Corporation and is the Medical Coordinator of an on-going clinical trial sponsored by IrriMax of a pressure device (IrriSept System) for the prevention of surgical site infections in emergency abdominal surgery (Clinical trials.gov Registration No. NCT02255487). The results of this trial will be published regardless of outcome. Dr. Fry is also a speaker for CareFusion, and a consultant to Prescient Surgical Co.