
Abstract
Abstract
Background:
This study assessed Staphylococcus aureus infection risk in patients with type 2 diabetes mellitus (T2DM) undergoing an orthopedic knee, hip, or spine surgery.
Patients and Methods:
All patients with a diagnosis of T2DM in the period from 2010 to 2012 were identified from a German claims database. First inpatient knee, hip, or spine surgery was used as index date. Cumulative incidence of S. aureus infections was calculated for several time intervals. Risk factors were identified based on a multi-variable Cox regression analysis. A case control analysis was conducted to assess mortality, healthcare resource utilization, and healthcare costs of S. aureus.
Results:
In total, 9,401 patients with T2DM underwent a knee, hip, or spine surgery. Mean age was 72.58 years, 63.32% were female, and 1.08% experienced an S. aureus infection in the 365-day follow-up period. The difference in all-cause direct treatment costs per patient–year between infected and non-infected patients was 24,437.50$. Mortality rates were 25.52% (S. aureus group) versus 5.22% (non-S. aureus group), based on a 365-day follow-up.
Conclusions:
Staphylococcus aureus is associated with a substantial healthcare burden and high mortality. Effective infection control measures should be considered to reduce post-surgical S. aureus infection risk in patients with T2DM.
S
Previous studies of S. aureus infections provide incomplete data. Some were conducted in single centers or had relatively short follow-up periods [6,7]; some reported SSI rates only, rather than the general spectrum of S. aureus [8,9]. Most of the studies did not analyze S. aureus infection rates in specific patient subgroups, for example, those with particular sociodemographic characteristics or underlying diseases such as type 2 diabetes mellitus (T2DM). This is important because of the high prevalence of T2DM [10,11], and the above-average post-operative infection risks of this patient group [9,12,13].
The present study sought to assess the S. aureus infection risk of German patients with T2DM undergoing an endoprosthetic knee or hip surgery or a spine surgery. Risk factors associated with a high S. aureus infection risk were also examined, along with mortality, healthcare resource utilization (HCRU), and the cost burden associated with S. aureus.
Patients and Methods
Study design and data source
A retrospective, non-interventional cohort analysis was conducted based on anonymized claims data provided by a German statutory health insurance fund (AOK PLUS; 2.7 million insured people in the German federal states of Saxony and Thuringia at time of study period). The analyses included only continuously insured patients with a diagnosis of T2DM (at least one inpatient or outpatient T2DM International Classification of Diseases and Related Health Problems [ICD-10]) diagnosis (ICD-10 code: E11*) during 2010 to 2012. Because of the anonymization of the data, approval by an ethics committee was not required.
Population selection
The index date was defined as the date of first observed inpatient surgery between July 1, 2010 and December 31, 2011. Any endoprosthetic hip and knee replacement surgery and any spine surgery (German operational procedure codes 5-820*; 5-821*; 5-822*; 5-823*; 5-83*) performed within the first two days after a hospital admission was included in the study (the asterisk denotes that all ICD-10 sub-codes with the same first digits as defined were included in the analysis). The baseline period was the six months before index date.
Exclusion criteria were: younger than 18 years of age at index date; any surgery performed at the same part of the body (knee/hip/spine) as the index surgery in the 180 days before index date; and any S. aureus infection documented in the 90 days before index date.
Staphylococcus aureus infection identification
Staphylococcus aureus infections were identified by inpatient and outpatient ICD-10 diagnoses, up to 365 days after index surgery. Any ICD-10 code that expresses specifically an S. aureus infection was considered; ICD-10 codes that express un-specified staphylococci were only included if an S. aureus code had also been documented. It was assumed S. aureus infection had occurred if any of the following ICD-10 codes were documented: A41.0 (sepsis caused by S. aureus); U80.0 (S. aureus with resistance to antibiotic agents); B95.6 (S. aureus as cause of a disease that is classified elsewhere). Distinction between MRSA and MSSA infections was not possible in this study because of the nature of the dataset and how infections are documented in German healthcare institutions. For the outpatient diagnoses, only the quarter of the year was available and therefore date of diagnosis was assumed to be middle of the applicable quarter.
Outcome measures
The percentage of patients with T2DM affected by S. aureus infection after index surgery was calculated for the following time periods: during the index hospitalization and 30, 90, 180, and 365 days after index surgery. Follow-up ended at date of patient death, date of any follow-up surgery not done on the same part of the body (knee/hip/spine) as the index surgery, or date of a first identified S. aureus infection. Time without S. aureus infection was depicted in Kaplan-Meier curves, censoring for death and follow-up surgeries as defined earlier. In an additional analysis, overall S. aureus infection rates were reported without any censoring for follow-up surgeries (censoring for death only).
Factors associated potentially with risk of experiencing an S. aureus infection after an orthopedic surgery were identified by means of a multi-variable Cox regression analysis, using time until first observed S. aureus infection (censoring for death and follow-up surgeries) as dependent parameter. The following were included as independent parameters: age at index date; gender; index surgery type; length of index hospitalization in days; Charlson Comorbidity Index (CCI) without age factor (based on the 6 mo before index date; Supplementary Table S1 [see online supplementary material at http://www.liebertpub.com/sur]); and number of antibiotic prescriptions in the six months before index date.
To assess outcomes associated potentially with S. aureus infections, we conducted a case control analysis, comparing patients with T2DM who experienced at least one S. aureus infection with those who did not experience any S. aureus infection but could have experienced infections caused by other pathogens during the follow-up period of 365 days after index surgery (only censoring for death of patients). All patients with an observed S. aureus infection were assigned to the S. aureus group in this analysis, even if the first S. aureus infection was observed after follow-up surgeries. Outcomes assessed were: number of general practitioner and specialist visits per patient–year; number and length of follow-up hospitalizations; prescribed defined daily dose (DDD) of antibiotic agents (as defined by the World Health Organization) [14]; and all-cause mortality. Mortality after index date was assessed by a multi-variable Cox regression analysis adjusting for age, gender, CCI, and antibiotic prescriptions in the six months before index date, surgery type, and any observed S. aureus infection as independent parameters.
Finally, all-cause direct healthcare costs per patient–year in the 365-day follow-up period were compared between patients with type 2 diabetes mellitus who experienced an S. aureus infection and those who did not. To calculate direct healthcare costs, we referred to diagnosis-related groups (DRGs) for hospitalizations and to official retail prices for medication prescriptions. For outpatient treatment, costs were approximated by documented treatment points per visit (one documented treatment point equals 0.035048€ for the years 2010 to 2012), indicating the complexity of a general practitioner/specialist visit in the German claims data system [15].
Statistical analysis
Sample characteristics were reported by descriptive statistics. As per parameter level and distribution, Pearson χ2 test, Mann-Whitney U test, t-test, and Kruskal-Wallis test were used to assess differences between patient groups. For all applied multi-variable regression models, a backward elimination methodology was applied. All factors not reaching a significance level of p < 0.10 were excluded stepwise. Factors reaching p ≤ 0.05 were interpreted as statistically significant. All reported p values were two-sided and 95% confidence intervals (CI) were calculated for hazard ratios (HRs). Descriptive evaluations were carried out with Microsoft SQL Server 2008 and Microsoft Excel 2010 (Microsoft Corporation, Redmond, WA). All other statistical analyses were carried out using Stata version 14.1 software (Stata Statistical Software: Release 14. StataCorp, College Station, TX).
Results
Observed patients
In total, 9,401 patients with T2DM undergoing an orthopedic surgery and meeting all other defined inclusion and exclusion criteria were identified. Of these patients, 3,784, 4,111, and 1,506 underwent a knee, hip, or spine surgery, respectively. Patients had a mean age of 72.58 years (standard deviation [SD]: 9.88 years); 63.32% were female (Table 1). Mean CCI (without age factor), based on the six-month baseline period, was 3.45 (SD: 2.25). Average length of the index hospitalization stay was 13.88 (SD: 7.91) days.
Listed are the characteristics of the observed samples used for the analysis.
CCI = Charlson Comorbidity Index; SD = standard deviation; T2DM = type 2 diabetes mellitus.
Incidence of S. aureus infections
Figure 1 depicts the S. aureus infection rates after index date. Overall, 1.08% of observed patients experienced an S. aureus infection in the 365-day follow-up period. The percentages of patients experiencing an S. aureus infection during the hospital stay and 30, 90, and 180 days after index surgery date were 0.22%, 0.31%, 0.68% and 0.83%, respectively. The number of new S. aureus infections per 1,000 patient–years decreased from 73.45 during the index hospitalization to 12.83 during the entire 365-day follow-up period (Fig. 1A). This analysis censored the follow-up period in case of death of a patient, a first observed S. aureus infection, or any follow-up surgery not performed in the same part of the body as the index surgery. If no censoring for follow-up surgeries was performed, the percentage of infected patients during the whole 365-day follow-up increased to 2.54% (Fig. 1B).
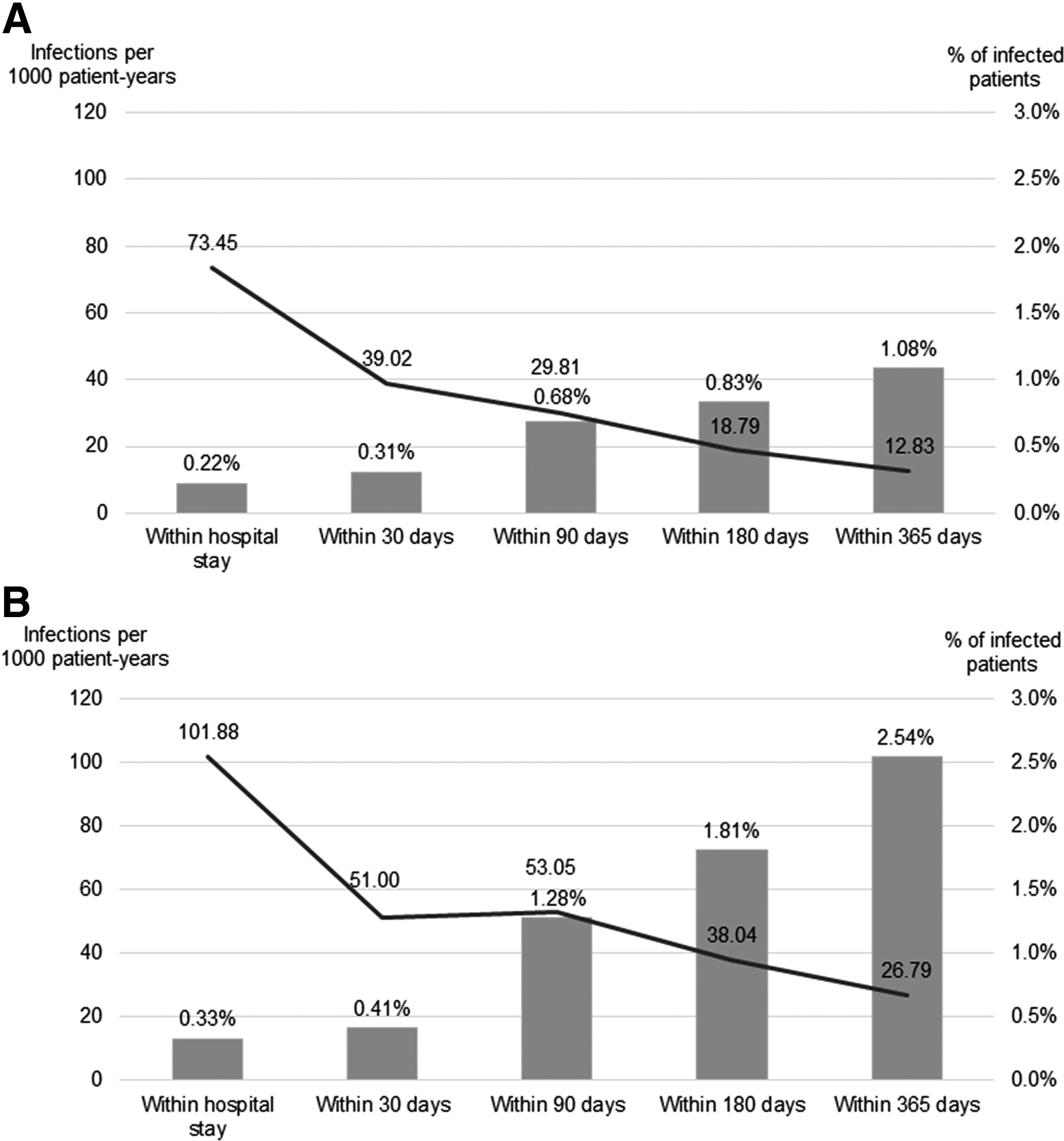
Staphylococcus aureus infection rates. The graphs show percentage of observed patients with type 2 diabetes mellitus (T2DM) affected by S. aureus infection during the hospital stay as well as after 30, 90, 180 and 365 days' (cumulative numbers). Only the first observed infection diagnosis was taken into account. Incident infection rates per 1000 patient-years for the respective time periods are also presented. (
Factors associated with S. aureus infection risk
Table 2 summarizes results of the multi-variable Cox regression analysis using time to first S. aureus infection as a dependent parameter; this analysis included censoring for follow-up surgeries not carried out in the same part of the body as the index surgery. Older age (HR = 1.05 for an additional year of age), higher CCI (HR = 1.21 for CCI score), and length of index hospitalization (HR = 1.03 for hospitalization length in days) were associated with higher infection risk; knee surgeries (HR = 0.51; hip surgeries as reference) were associated with lower infection risk. Number of antibiotic prescriptions in the six-month baseline period and patients' gender were found to be non-significant independent parameters, and were excluded from the final model. Figure 2 presents Kaplan–Meier curves for the patient sub-groups as defined by type of index surgery and CCI.

Kaplan-Meier curves for the percentage of patients with type 2 diabetes mellitus (T2DM) free of Staphylococcus aureus infection after an orthopedic surgery. The graphs show percentage of patients with T2DM still free of S. aureus infection after an orthopedic surgery. Cumulative survival after 365 days: hip, 0.982 (confidence inerval [CI]: 0.978–0.986); knee, 0.994 (CI: 0.990–0.996); spine: 0.987 (CI: 0.980–0.992). Differences between the groups were analyzed using log rank tests. (
Patients included: 9,401; events (S. aureus infections): 102 (censored for follow-up surgeries); log likelihood: −875.71; LR χ2 = 92.18; (Prob > χ2) < 0.001.
Based on 6-mo baseline period before index.
Age was excluded from CCI.
CCI = Charlson Comorbidity Index; CI = confidence interval.
Outcomes associated with S. aureus infections
Table 3 shows all-cause mortality, HCRU, and all-cause direct healthcare costs for patients who experienced an S. aureus infection compared with those who did not (based on a 365-d follow-up since index surgery). Kaplan–Meier curves in Figure 3 depict the time until death for both patient groups.

Kaplan-Meier curves for the percentage of surviving patients with T2DM after an orthopedic surgery. The graph shows the percentage of patients still alive after their surgery, differentiating between patients who experienced a Staphylococcus aureus infection in the 365-day follow-up period (cumulative survival after 365 days = 0.745, confidence interval [CI]: 0.685–0.795) versus those who did not experience an S. aureus infection (cumulative survival after 365 d = 0.945; CI: 0.943–0.952). Differences between the groups were analyzed using log rank tests (survival difference between patients with and patients without S. aureus infection <0.001).
Index hospitalization excluded.
DDD = defined daily dose; GP = general practitioner; HCRU = healthcare resource utilization; T2DM = type 2 diabetes mellitus.
Healthcare resource use and all-cause treatment costs per patient–year were higher for patients who experienced an S. aureus infection. The number of hospitalization days per patient–year in the 365-day follow-up period of S. aureus-infected patients (hospitalization related to index surgery always excluded) was 50.40 days; patients without S. aureus infection spent only 7.90 days in hospital (p < 0.001). Differences in HCRU were translated into a difference in all-cause direct treatment costs of 24,437.50$ per patient-year between the patient groups (30,066.70$ in the S. aureus group versus 5,629.77$ in the group without S. aureus infection; p < 0.001). Among patients affected by S. aureus, all-cause direct healthcare costs did not differ significantly (p = 0.430) between surgery types (knee: 30,074.40$; hip: 25,656.70$; spine: 26,948.50$).
Substantial differences in mortality were observed between S. aureus and non-S. aureus patients. Ninety days after index date, 8.37% of the patients in the S. aureus group had died versus 2.74% in the non-S. aureus group (p < 0.001). Respective mortality numbers for the 365-day follow-up were 25.52% in the S. aureus versus 5.22% in the non-S. aureus group (p < 0.001). Results were confirmed in a multi-variable Cox regression analysis using time to death as dependent parameter (Table 4). Among other parameters such as age in years (HR = 1.11), CCI (HR = 1.21), number of baseline antibiotic prescriptions (HR = 1.21), female gender (HR = 0.71), and knee surgery (HR = 0.32; hip surgery as reference), an S. aureus infection was shown to be an independent predictor of early death in this patient sample (HR = 2.94).
Patients included: 9,401; events (deaths): 539; log likelihood: −4438.94; LR χ2 = 952.99; (Prob > χ2) < 0.001.
Based on 6-mo baseline period before index.
Age was excluded from CCI.
CCI = Charlson Comorbidity Index; HR = hazard ratio; CI = confidence interval.
Discussion
This study investigated the incidence of S. aureus infections after a hip or knee replacement surgery or a spine surgery in patients with T2DM in Germany. It also assessed risk factors for these infections, as well as clinical and health-economic outcomes associated with S. aureus. Patients with T2DM face an above-average risk for post-surgical infections [9,12,13]; they also constitute a substantial proportion of the elderly population in Germany, with a prevalence of more than 20% in those aged older than 75 years [11].
Orthopedic surgeries were assessed because they are most often performed electively [16], thus allowing physicians and patients time to consider the risks and benefits of the procedure and apply the most appropriate infection control measures to reduce risk of post-surgical infections.
Of the observed patients, 0.22% were affected by an S. aureus infection during their index hospital stay. This percentage increased to 0.68% (90-d follow-up) and even 1.08% (365-d follow-up). Staphylococcus aureus infection rates were higher in older and more comorbid patients and in those who underwent hip surgery.
These results are in line with numbers reported in earlier studies. A recent German study reported an SSI rate, based on hospital records only, of 0.98% for orthopedic surgeries. In this study, 31% of SSIs were caused by S. aureus [5]. In the United States, an S. aureus infection rate of 0.2% of all patients (after 90 d: 0.9%) after orthopedic surgery was reported, with approximately one-third caused by MRSA [1]. Other studies reported similar S. aureus infection rates of 2.3% or less for a follow-up of 180 days after index surgery [3,4].
In the current study, without censoring for follow-up surgeries, the reported S. aureus infection rates were substantially higher (2.54% of affected patients versus 1.08% in the 365-d follow-up period). Censoring for follow-up surgeries was implemented to exclude any S. aureus infections possibly not related to the index surgery. However, this methodology might have led to an under-reporting of S. aureus infection rates because even follow-up surgeries not performed on the same body part might have been caused by previous undocumented S. aureus infections.
Risk factors associated with identified S. aureus infections were consistent mainly with a U.S. population study that analyzed risk factors for MRSA infections. Patients with more comorbidities and those who experienced earlier infections, leading to above-average antibiotic use, generally faced a higher S. aureus infection risk [17]. Regarding the impact of gender on S. aureus infection risk, published findings are conflicting: some report higher infection rates for male patients [4,17]; some report it for MSSA but not MRSA infections [1,5]. The present study cannot confirm that women face an under-average S. aureus infection risk, because gender was not found to be a significant independent predictor.
The analysis of all-cause direct healthcare costs for the 365-day follow-up period since index surgery demonstrated that patients with T2DM affected by S. aureus infection had 18,492.54€ higher costs per patient–year compared with those without S. aureus infection. This result was mainly driven by inpatient hospitalization costs and is in line with U.S. analyses, which have reported a high healthcare resource burden and high costs associated with S. aureus infections [18,19].
Staphylococcus aureus infections in patients with T2DM after an orthopedic surgery also led to substantially higher mortality, compared to patients with T2DM without S. aureus. The results for 90-day post-surgery mortality (2.74% in the non-S. aureus and 8.37% in the S. aureus group) are comparable to previous studies reporting death rates of 1.5%–3% for non-infected patients, 6.7%–13.1% for patients with MSSA, and 16.7%–20.7% for those with MRSA infections during 90-day follow-up after any surgery [1,18,19]. Another recent publication has reported similar death rates of 6.6% for patients without S. aureus and 16.8% for those with S. aureus in the 180 days after an orthopedic surgery [4]. For the 365-day follow-up in the current study, respective mortality in the S. aureus group was 25.52% versus 5.22% in the non-S. aureus group. In the multi-variable analysis, S. aureus infection was associated with a three-fold increase of early death.
In summary, S. aureus infections in patients with T2DM are associated with a serious healthcare burden and substantial mortality risk. Whereas orthopedic procedures can improve patients' quality of life, appropriate risk management through infection control measures should be considered. In addition, S. aureus infection risk should be included in the patient-specific benefit–risk assessment for an orthopedic surgery; this would prevent over-estimation of the benefits of surgery and under-estimation of the risks.
Limitations
This study has some limitations. First, S. aureus infections were identified via outpatient and inpatient diagnoses without laboratory data to confirm infection. Additionally, there is no specific code for SSIs caused by S. aureus in the German system; the study may therefore be affected by an under-reporting of S. aureus infections.
Second, it was assumed that every S. aureus infection seen in the dataset was associated with the observed index orthopedic surgery. Whereas this can be surmised with some certainty for infections observed during the index hospital treatment and 30-day follow-up period, S. aureus infections during the longer follow-up periods may have been caused by other factors, e.g., a stay in a nursing home or another hospital stay. To minimize this risk, infection rates and time to first infection were reported based on methodology that censored for follow-up surgeries not performed on the same part of the body as the index surgery; surgeries carried out on the same part of the body were not censored because these might have been revisional surgeries resulting from the S. aureus infections themselves.
Third, because of the conservative definition used for S. aureus infections, there may have been additional under-reporting of infection rates, HCRU, and costs. Even if patients experienced more than one S. aureus infection, only the first observed infection was included in the analyses. Additionally, follow-up surgeries on other regions of the body, potentially caused by S. aureus SSI after hip, knee, or spine surgeries, were not included in the analyses because the follow-up period ended at the date of this surgery.
Another study limitation is that patients who experienced a previous surgery in the 180-day baseline period were excluded only if that surgery was performed on the same part of the body as the index surgery; this was done to ensure the index surgery was not a revisional surgery performed because of prior surgery infection. However, other previous surgeries, which could have caused an S. aureus infection leading to the observed index surgery, were not excluded. That analyses of factors associated with infection risk and mortality of patients could only include parameters available in the claims dataset can also be cited as a study limitation. More detailed information on patient, surgery, or hospital characteristics was not available.
In addition, the health insurance fund covers patients in two regions of Germany only, and this may have caused regional bias. Nevertheless, health reimbursement rules are identical across Germany, still it is possible differences exist in S. aureus screening/management in the included regions' hospitals compared with the rest of Germany; the authors are not aware of any differences, however.
As a result of the nature of the dataset, it was impossible to identify MRSA infections as a sub-group of S. aureus infections. Based on previous publications, it can be assumed that approximately one-third of patients infected with S. aureus were affected by MRSA; these patients face an even higher healthcare burden than those with MSSA infections [1]. Moreover, we were not able to describe additional risk factors that are shown to be associated with S. aureus infection, such as increased glucose level after surgery, baseline body mass index, duration of surgery, and timing of peri-operative antibiotic therapy as well as the status of S. aureus colonization.
Conclusions
In German patients with T2DM, S. aureus infection risk after an orthopedic hip, knee, or spine surgery is high. Older patients with a high comorbidity burden face an above-average infection risk. Staphylococcus aureus infections are a healthcare burden because of high associated costs and high mortality. Effective infection control measures should be considered to target this population, with the aim of reducing the risk of S. aureus infection after an orthopedic surgery.
Footnotes
Acknowledgments
This study was supported by Pfizer. The editorial support was provided by Engage Scientific and was funded by Pfizer Inc.
Because of the non-interventional, retrospective nature of this study and because our analysis involved an anonymized dataset, neither ethical review nor informed consent of the patients was required. However, the study protocol was reviewed by a scientific steering committee to which all the authors belonged.
Author Disclosure Statement
H. Yu and K. Heinrich are employees of Pfizer. T. Wilke has received honoraria from several pharmaceutical/consultancy companies (Novo Nordisk, AbbVie, Merck, GSK, BMS, LEO Pharma, AstraZeneca, Bayer, Boehringer Ingelheim, Pharmerit). S. Mueller and F. Gottschalk participated in this study as staff members of Ingress-Health; Ingress-Health work in this study was sponsored by Pfizer. U. Maywald and A. Fuchs have no potential conflict of interest, except those potentially related to their employer, AOK PLUS.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.