
Abstract
Abstract
Background:
According to existing guidelines, orthopedic specimens collected in joint and bone infections (JBI) in our institution are cultured on several media sets and incubated for two, seven, and 14 days. The optimal timing for de-escalation of the first-line antibiotic combination according to the culture results needs to be defined.
Methods:
Single-center, retrospective analysis of all adult patients with a first documented episode of JBI between May 2012 and April 2013.
Results:
Ninety patients were included, 51 males (57%), median age 58 y (range 18–87 y), with prosthesis infection in 62 cases (69%). Rapidly growing pathogens (Staphylococcus aureus [n = 36] and Enterobacteriaceae [n = 12]) usually were diagnosed within two days, whereas coagulase-negative staphylococci (n = 25) and Propionibacterium acnes (n = 13) generally were identified after seven days (p < 10−5). Positive culture results at day 2 fit with definitive microbiological diagnosis in 95% of cases, and prolonged incubation led to the identification of additional micro-organisms in only four of 76 patients (5%) with day-2-positive cultures. Conversely, for those with negative two-day culture (n = 14), the seven-day culture allowed identification of less virulent pathogens in eight cases (57%).
Conclusions:
Our results suggest that, in JBI, de-escalation of the empirical antibiotic regimen can be based on micro-organisms identified on the two-day culture set. The impact of such a strategy on clinical outcomes, antibiotic consumption, and costs needs to be assessed in larger studies.
R
Patients and Methods
All procedures were conducted in accordance with the ethical standards of the National Research Committee and the 1964 Helsinki Declaration and its amendments.
For this type of observational retrospective study, formal informed consent is not required.
Setting
This retrospective single-center study was set up at the Academic Cochin Hospital (Assistance Publique-Hôpitaux de Paris, Paris, France), a 1,500-bed tertiary-care hospital. The Department of Orthopedic Surgery is a general orthopedic and trauma setting and a referral center for the management of malignant bone tumors. On average, 900–1,000 orthopedic prostheses are implanted each year. All cases of suspected or documented JBI are discussed weekly in a multidisciplinary meeting (surgeons, microbiologists, infectious disease clinicians, and anesthesiologists). Decisions regarding antibiotic regimen are taken collectively on the basis of peri-operative findings and microbiological and clinical data and in accordance with local and national guidelines. After discharge, patients are followed by surgeons, and data regarding medical management are collected routinely on a standardized electronic form.
Patients
All medical records reviewed in the multidisciplinary meeting between May 2012 and April 2013 were screened. Patients aged 18 years and older with a first documented episode of JBI were included. Prosthetic infections were defined by the following criteria [1,2,13]: (1) culture of the same micro-organism in ≥2 peri-operative specimens (or one single culture for virulent pathogens; i.e., S. aureus); and (2) purulence of synovial fluid or acute inflammation on histopathologic examination of peri-prosthetic tissue or the presence of a sinus tract communicating with a prosthesis. Similar criteria were used in the absence of indwelling material. Patients with fungal and mycobacterial infections were excluded. Medical files were searched for data on medical history (co-morbidities, malignant tumor, etc.), antibiotic regimen, and outcome at the end of follow-up. Outcomes were reported as (1) alive with no clinical or laboratory signs of infection; (2) death; (3) relapse with the baseline pathogen; or (4) re-infection with another pathogen.
Microbiologic methods
In the context of high suspicion of infection, it is recommended that surgeons collect five per-operative biopsy specimens and inoculate them on five culture media: (1) one blood agar and one heated blood agar (BioMérieux, Marcy L'Étoile, France), which are incubated for two days at 35°C anaerobically and with 5% CO2; (2) another set of agar and heated blood agar media, which are incubated for seven days, and (3) one Schaedler enrichment broth supplemented with 0.2% agar (BioMérieux), which is incubated for as long as 14 days. Bacterial isolates are identified using matrix-assisted laser desorption/ionization time of flight (MALDI TOF) (MALDI BioTyper, Bruker Daltoniks, Leipzig, Germany), and antibiotic susceptibility testing is performed by the disc diffusion method or in Vitek2 (BioMérieux) in accordance with the EUCAST 2012 and 2013 guidelines. The definitive microbiologic diagnosis is settled with culture results at the end of the 14-day incubation period. The timing (up to two days, seven days, or 14 d) and medium of first positive culture were collected for each micro-organism isolated. Infection was considered to be multi-microbial if at least two bacterial species were isolated from one or several specimens.
Statistical analysis
Results are expressed as n (%) for categorical variables and median (minimum, maximum) for continuous variables. We used the Wilcoxon test for continuous variables and the Fisher exact test for categorical variables. A two-sided p value <0.05 was considered statistically significant. Statistical analysis was performed using the R software version 3.1.2 (R Development Core Team, R Foundation for Statistical Computing, Vienna, Austria).
Results
Study population
Over the study period, 104 consecutive patients were screened. Among them, 90 had a confirmed first episode of infection and were included in the analysis (Table 1). The reasons for non-inclusion were diagnostic criteria not fulfilled (n = 7) or more than one previous episode of infection (n = 7). The patients were mainly males (n = 51; 57%) of median age 58 y (range 18–87 y). Nine (10%) had diabetes mellitus. Sites of infection were the knee (n = 28; 31%), hip (n = 27; 30%), foot (n = 13; 14%), upper limb (n = 12; 13%), and spine (n = 10; 11%). In 62 cases (69%), the infection involved an indwelling orthopedic device (joint prosthesis or internal fixation device). The median time between the index and revision surgery was <1 mo in 17 cases (30%), 1 to 12 mos in 15 cases (27%), and >12 mos in 24 cases (43%). Patients with bone tumors (n = 14, 16%) were mainly females (n = 10) of median age 43 years (range 18–85 y).
Amoxicillin, cloxacillin, amoxicillin–clavulanatic acid, or piperacillin–tazobactam.
Microbiologic findings
Over the study period, 406 clinical specimens were collected from 90 patients, corresponding to a median of four specimens per patient (mean 4.5; range: 1–13), and 121 bacterial isolates were obtained (Table 2). The most frequently isolated species were Staphylococcus aureus in 36 patients (40%) and coagulase-negative staphylococci (CNS) in 25 (28%). Culture yielded more than one micro-organism in 21 patients (23%), the most frequent combination being CNS/Propionibacterium acnes, which was recovered from five patients. Although non-significantly, CNS seemed to be isolated more frequently in infections of orthopedic devices than in patients without such devices (34% and 14% for the two types, respectively; p = 0.07). In the 14 patients with malignant bone tumors, the most frequent pathogen was CNS (n = 5). The infection was polymicrobial in four cases and involved anaerobic pathogens in two cases. Isolation of P. acnes occurred significantly more frequently in patients with upper limb or spine infections (p = 10−4).
Results are presented as number of isolates (%) for each culture set.
Time to culture positivity
The definitive microbiologic diagnosis was obtained within two days in 72 patients (80%), seven days for 11 patients (12%), and 14 days for the remaining seven patients (8%; Fig. 1). The proportion of patients with negative cultures after two days was significantly higher (p = 10−4) in patients with upper limb (n = 6; 50%) or spine (n = 4; 40%) infections than in those with infections in other locations: Knee (n = 1; 4%), hip (n = 3; 11%) and foot (n = 2; 15%). The time to culture positivity was not linked to the presence of an implanted device (p = 0.64) but differed according to the nature of the microorganism (p < 10−5). As reported in Table 2, most pathogens were diagnosed within two days of culture: 97% of S. aureus isolates (n = 35), 100% of Enterobacteriaceae (n = 12), 91% of Streptococcus spp. (n = 10), 90% of Enterococcus spp. (n = 9) and 100% of Pseudomonas aeruginosa (n = 8). On the other hand, the large majority of P. acnes strains were first identified after seven days (n = 9; 69%) or 14 days (n = 3; 23%) of incubation. The timing for CNS was similar (8% and 16%, respectively).
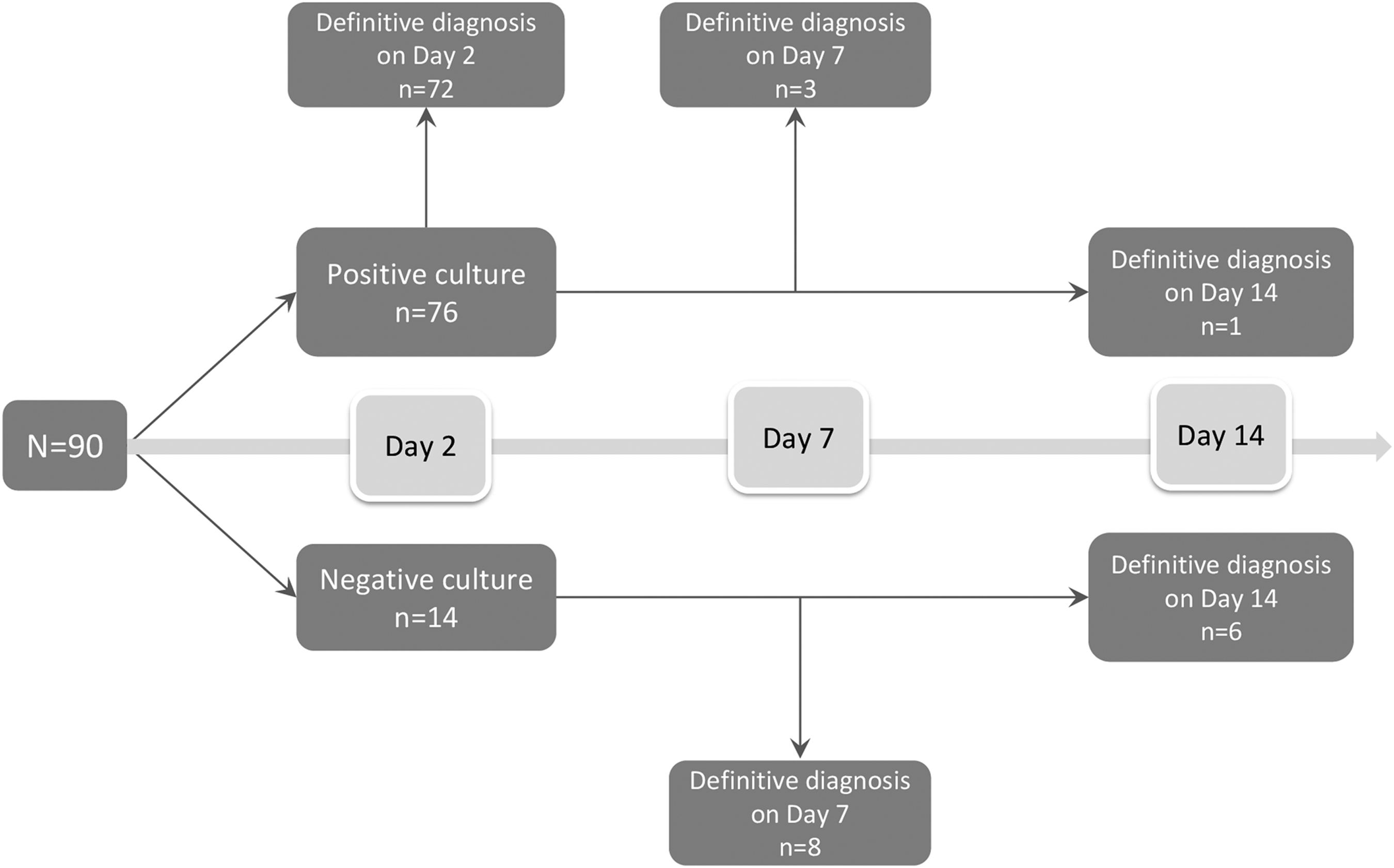
Sequence of positivity of samples cultures.
Antibiotic regimen in relation to culture positivity
As shown in Table 1, the antibiotics most frequently used for treatment were fluoroquinolones (levofloxacin or pefloxacin in 55 patients; 61%) and penicillins or penicillins/β-lactam inhibitor (amoxicillin, cloxacillin, amoxicillin-clavulanic acid or piperacillin-tazobactam, n = 49; 54%), which frequently were associated (n = 23; 26%). First-line antibiotic therapy was switched after a median of six days (range 1–63 days): within four days in 20 patients (26%), between five and eight days in 32 (42%), and beyond day 9 in 24 (32%). The median time to first antibiotic switch did not differ according to the time to culture positivity (5.5 days for patients with definitive microbiologic diagnosis at two days vs. 6.5 days for the others; p = 0.83). Bacteriological documentation on day 7 led to a switch of the antibiotic therapy in six patients, either to narrow the antibiotic spectrum for P. acnes (n = 3) or to broaden the spectrum for methicillin-resistant CNS (n = 3). Twenty-eight patients were switched to the oral route after 15 days of intravenous administration (median; range 4–38), for an additional median duration of 28 days (range 7–162 days). Clindamycin-fluoroquinolone was the most frequent combination (n = 11).
Outcomes at the End of Follow-Up
Seven patients were lost to follow-up immediately after surgery. Of the 83 remaining patients, the duration of follow-up was ≤1 mo in 14, 1–12 mos in 35, and ≥12 mos in 34. At the end of follow-up, 69 patients were alive with no relapse of infection, one had died, seven had suffered a relapse with the baseline micro-organism (S. aureus in five), six had experienced reinfection with another pathogen (S. epidermidis, Streptococcus dysgalactiae, Escherichia coli, Ps. aeruginosa, unidentified in two cases). Signs of relapse were reported before the end of antibiotic therapy in two patients and after discontinuation of antibiotics in five.
Discussion
In this cohort of 90 patients with microbiologically documented JBI, we aimed to assess the impact of culture timing on decisions about antibiotic therapy. Bacterial species usually considered pathogens (S. aureus, Enterobacteriaceae, Ps. aeruginosa, Streptococcus spp., and Enterococcus spp.) accounted for 64% of the micro-organisms isolated, and most were cultured within two days. Conversely, CNS and P. acnes (31% of the isolates) were obtained mainly from day 7 to day 14. Upper limb and spine infections were more frequently associated with negative results on day 2. The results of the seven-day culture led to a substantial modification of the antibiotic therapy in six patients (7%).
There is no consensus on the optimal incubation time for the diagnosis of JBI. In a general orthopedic and trauma setting with a high proportion of post-traumatic infections, Schwotzer et al. showed that 97% of orthopedic device-associated infections were diagnosed within seven days of incubation. However, P. acnes accounted for less than 5% of the bacteria in their cohort [6]. In populations with a higher incidence of low-virulence micro-organisms (14% of Propionibacterium species in [7]), prolonging incubation of the culture for two weeks allowed isolation of a significant proportion of micro-organisms that would otherwise have remained unidentified. In our analysis, CNS and P. acnes accounted for 20% and 10% of the total number of isolates, respectively. The use of prolonged culture sets led to a definitive bacteriologic diagnosis in 18 patients (20%), which confirms their usefulness in a setting with a relatively high incidence of slow-growing or fastidious organisms. We also found a relatively high number of polymicrobial samples that were less abundant [6] or absent [7] in other reports. This might reflect the high proportion of patients with bone tumors (16%) in our cohort. As hypothesized previously, polymicrobial infections in patients with bone tumors may be explained by a high risk of post-resection hematoma leading to colonization with anaerobic bacteria, by the use of pre-operative radiotherapy causing tissue hypo-oxygenation, and by location near the pelvis, which can lead to breaches in the digestive tract [14].
Several observations can be drawn from our results. First, in patients with positive cultures on day 2, prolonged incubation leads to the identification of additional micro-organisms in only a small proportion of patients (4/76; 5%). Second, negativity of the two-day culture in a context of clinical suspicion of JBI is no argument to discontinue antibiotics, particularly for patients with upper limb and spine infections, which are more frequently related to P. acnes. Third, the first-line antibiotic regimen was maintained for almost one week, regardless of the two-day culture results, suggesting that the seven-day culture was perceived as a milestone in the process of narrowing the antibiotic spectrum, thus potentially delaying de-escalation in some patients. These results suggest that in patients with positive cultures on the two-day culture set, early de-escalation of the antibiotic regimen is a reasonable option. Nevertheless, in case of culture negativity at day 2 and if the suspicion of infection remains high, particularly in upper limb and spine infections, our local protocol now recommends maintaining an empirical antibiotic combination of clindamycin, a fluoroquinolone, or both that targets P. acnes and most of the CNS throughout the 14-d holding period. Antibiotics are discontinued in patients with negative cultures after 14 d of incubation.
As previously shown in other settings [10], there are many potential benefits of early de-escalation in orthopedic patients. Switching to the oral route and discontinuation of antibiotics that are available only in hospital pharmacies could allow earlier discharge of patients. Consumption of antimicrobial agents and related costs also could be reduced. For example in our orthopedic department, daptomycin accounted for 61% (167,000 €/270,000 €) of the total antimicrobial costs in 2016. Daptomycin has broad anti-gram-positive activity, good bone penetration, and high bactericidal activity in biofilms [15]. It is an effective and well-tolerated treatment option for osteomyelitis and therefore is widely used as first-line empiric treatment in our institution. Earlier discontinuation of this drug in the absence of gram-positive bacteria on the two-day culture set could lead to a significant reduction in antibiotic costs.
Our study has several limitations. It was single center, with a relatively small sample. Our local epidemiology may differ from that of other centers; in particular, the high proportion of bone tumors probably led to a higher rate of polymicrobial infections. Second, the study was retrospective. The follow-up times were highly variable: Seven patients were lost to follow-up right after surgery and 14 during the month after surgery, which weakens our conclusions on final outcomes. And finally, we included patients with different clinical presentations (acute, delayed, and late infections, presence of various orthopedic devices), who were pooled in the analysis. This study aimed at describing the microbiologic features associated with JBI over a one-year period in our institution to provide clinicians a practical guide for antibiotic adaptation. This heterogeneity reflects the diversity of clinical situations that are faced in a general orthopedic ward and illustrates the obstacles to defining a unique strategy.
Our results suggest that in patients with a JBI, early de-escalation of empiric antibiotic regimens could be based on micro-organisms identified on the two-day culture set. However, longer incubation remains of great interest in patients with negative cultures on day 2 in order to identify slow-growing organisms such as P. acnes and CNS. The impact of such a strategy on clinical outcomes, antibiotic consumption, costs, and antimicrobial resistance remains to be confirmed in larger prospective studies.
Footnotes
Author Disclosure Statement
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sector.
Each author certifies that he or she has no commercial associations (e.g., consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with this paper.