
Abstract
Abstract
Background:
Surgical site infection remains a significant concern in treating patients with open fractures. In prevention of such, current guidelines support the immediate administration of antibiotic agents. The duration of antibiotic treatment is still controversial. A maximum of 72 hours, even in the absence of definitive soft tissue coverage, is recommended in a number of recent guidelines and consensus reports. The aim of this meta-analysis was to review and analyze all published literature evidence with regard to antibiotic duration in open fracture treatment.
Methods:
We conducted a comprehensive review of the available literature from the 1970s until the present, including five comparative (1284 open fractures) and 27 observational (5408 open fractures) studies. A subgroup analysis was further performed, based on the Gustilo type of open injury and the anatomic location of the fracture. In addition, we investigated the effect of antibiotic regimes shorter than 72 hours on infection rates.
Results:
In the comparative studies, the summarized estimate of infection rate favored less than a 72-hour duration of antibiotic treatment, because prolongation of antibiotic treatment more than 72 hours did not seem to offer any protective effect against septic complications of open fractures (odds ratio: 0.85, 95% confidence interval [CI]: 0.60–1.21). The same trend was also documented in the observational studies, where the overall pooled estimate of infection rate was 10% (95% CI: 6.8%–14%) when antibiotic treatment did not exceed 72 hours and 9.2% (95% CI: 6.6%–12.2%) for more than 72 hours of antibiotic treatment (p = 0.53). In Gustilo I and II open fractures, the calculated pooled estimate of infection rate did not differ significantly when antibiotic treatment exceeded 72 hours (6%, 95% CI: 3.3%–9%) compared with shorter (up to 72 h) antibiotic protocols (4%, 95% CI: 1.8%–7%) (p = 0.52). In Gustilo III open fractures also, the calculated pooled estimate of infection rate (21.3%, 95% CI: 13%–31%) when duration of antibiotic treatment was more than 72 hours did not differ significantly compared with a shorter (less than 72 h) antibiotic treatment (17.7%, 95% CI: 12.5%–23.5%) (p = 0.39). A further subgroup analysis indicated that even shorter antibiotic regimes (24–48 h) were also equivalent to prolonged regimes of more than 72 hours in terms of infection rates.
Conclusions:
The results of the present systematic review and meta-analysis could not substantiate any benefit against septic complications of a prolonged duration of antibiotic treatment of open fractures, irrespective of their severity.
I
In elective orthopedic practice, single-dose antibiotic agents are sufficient to prevent peri-operative infections, as has been shown in joint arthroplasties [7].
The guidelines published by the British Orthopaedic Association [8], which strictly speaking refer to the management of tibial open fractures, advocate the use of broad-spectrum antibiotic agents in the emergency department (or even earlier—i.e., on site or in the ambulance [5,9,10] and at the time of wound debridement to decontaminate the wound [Step 1: decontamination]) and recommend the administration of teicoplanin (or gentamicin) at induction at the time of skeletal stabilization and definitive soft tissue cover to reduce the risk of hospital-acquired infections (Step 2: prevention of nosocomial infection). Co-amixoclav should be administered concomitantly until definitive wound cover has been established or for a maximum of 72 hours. These measures in combination with timely debridement, irrigation, and early definitive soft tissue cover by an orthoplastic team are expected to minimize the risk of post-injury infection [11].
The aim of the present meta-analysis was to validate the consensus opinion that short-term antibiotic protocols (duration of intravenous antibiotic treatment up to 72 h or less) are as efficient as longer-term regimes in reducing infection rates of all long bone fractures.
Methods
Literature search and data extraction
We conducted a systematic and comprehensive review of the existing literature adhering to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines [12]. Before commencing the comprehensive literature search, a written study protocol was established including clearly defined eligibility criteria and specifying the criteria for further subgroup and sensitivity analyses. Clinical studies dealing with open long bone fractures with a clear documentation of the duration of the utilized antibiotic protocol and reporting on infection rates in association with the duration of the respective antibiotic protocol were regarded eligible for inclusion in the systematic review. Exclusion criteria included pediatric open fractures, open spinal injuries, open fractures of hand, foot, and maxillofacial region, experimental studies, animal studies, case reports, and studies containing fewer than 20 subjects.
A comprehensive electronic search of MedLine via the PubMed search machine was performed using the following search terms and Boolean operators: “open fracture” AND “antibiotics.” The search was further extended to the Ovid MEDLINE, CINAHL, Cochrane Library, Embase, Google Scholar, and Scopus databases. No language restrictions were set. Further, other relevant publications (such as reviews and meta-analyses) were obtained, and their bibliographies were searched manually for potentially eligible papers. Any disagreement between the two reviewers was resolved by discussion. From each eligible article, information on author's name, year of publication, type of study, demographic and baseline characteristics of participants, follow-up details, outcome data, and complications were extracted and documented on an Excel sheet. No limitation was set a priori with respect to the type of eligible studies, although our priority was to include high quality comparative studies.
Quality assessment
The methodologic quality of all primary studies was evaluated with the Coleman Methodology score (CMS) [13]. The total score can range from 0 to 100, and higher scores are indicative generally of absence of various biases and confounding factors. The final score was categorized as excellent (85–100 points), good (70–84 points), fair (50–69 points), and poor (<50 points). The criteria of the CMS were modified slightly to suit the purpose of the present systematic review (Table 1). Each primary study was assigned a score independently by the two reviewers. The final score of each individual study constituted the average value of the scores given by the two reviewers. The agreement between the two assessors was tested with intra-class correlation coefficient (ICC).
RCT = randomized controlled trial.
Statistical analysis
For comparative studies, pooling of data was performed with the Mantel-Haenszel (M-H) statistical method and an either fixed or random effects model, depending on the degree of the statistical heterogeneity present (in the presence of significant statistical heterogeneity, a random effects model was used). Binary outcomes were summarized as odds ratios (ORs) with 95% confidence intervals (95% CI). The results of each primary study and the combined estimate of effect size were presented graphically as forest plots. Statistical heterogeneity was measured with the use of both Cochran's X2 (Q-test) and I2 statistics [14,15]. Significance was set at 0.1 for the Q test (because it is characterized by low sensitivity for detecting heterogeneity). An I2 value >50% was thought to represent significant heterogeneity. The RevMan (5.2) software (Review Manager, The Nordic Cochrane Centre, Copenhagen, Denmark) was used to present the study findings, produce pooled estimates of effect size, and test the presence of statistical heterogeneity.
For observational studies without a comparator cohort, all outcomes of interest were expressed as proportions (p), (infection rates). Pooling of proportions was performed with the MedCalc software (version 14.8.1) using a random effects model. Statistical heterogeneity was also tested with Cochran's Q test and Higgins I2 test. Non-parametric comparisons of the median values of outcomes of interest between two groups were performed with the Mann Whitney U test.
Subgroup analysis
The type of open fracture (according to the Gustilo classification) and the anatomic site of the open fractures were the a priori set criteria for subgroup analysis. After reviewing the primary studies, we realized that there were even shorter antibiotic prophylactic regimes of up to 24 or 48 hours that were used by some authors. Consequently, we also compared those regimes with the longer antibiotic prophylaxis of more than 72 hours in terms of infection rate.
Sensitivity analysis
The criteria of sensitivity analysis were also pre-specified and included studies of dubious eligibility, poor methodologic quality, or outlying results. We intended to repeat the analysis after excluding studies fitting the above categories. We would regard the results of our review with greater certainty if the process of sensitivity analysis did not affect them.
Results
Search process
The initial electronic search generated 847 results. Another 53 records were identified through published guidelines and consensus documents. After duplicates were removed, 794 abstracts and abstract titles were screened for suitability. For full article review, 57 publications were retrieved and analyzed. After applying eligibility criteria, 32 studies were left for final analysis (see PRISMA flowchart, Fig. 1). Five of them were comparative studies [16–20], while the remaining 26 were observational non-comparative studies [5,19,21–44]. In one comparative study [18], we analyzed separately two different treatment groups, based on the type of the used antibiotic prophylaxis. Subsequently, there were six pairs of treatment groups available for pooled analysis out of five comparative studies.
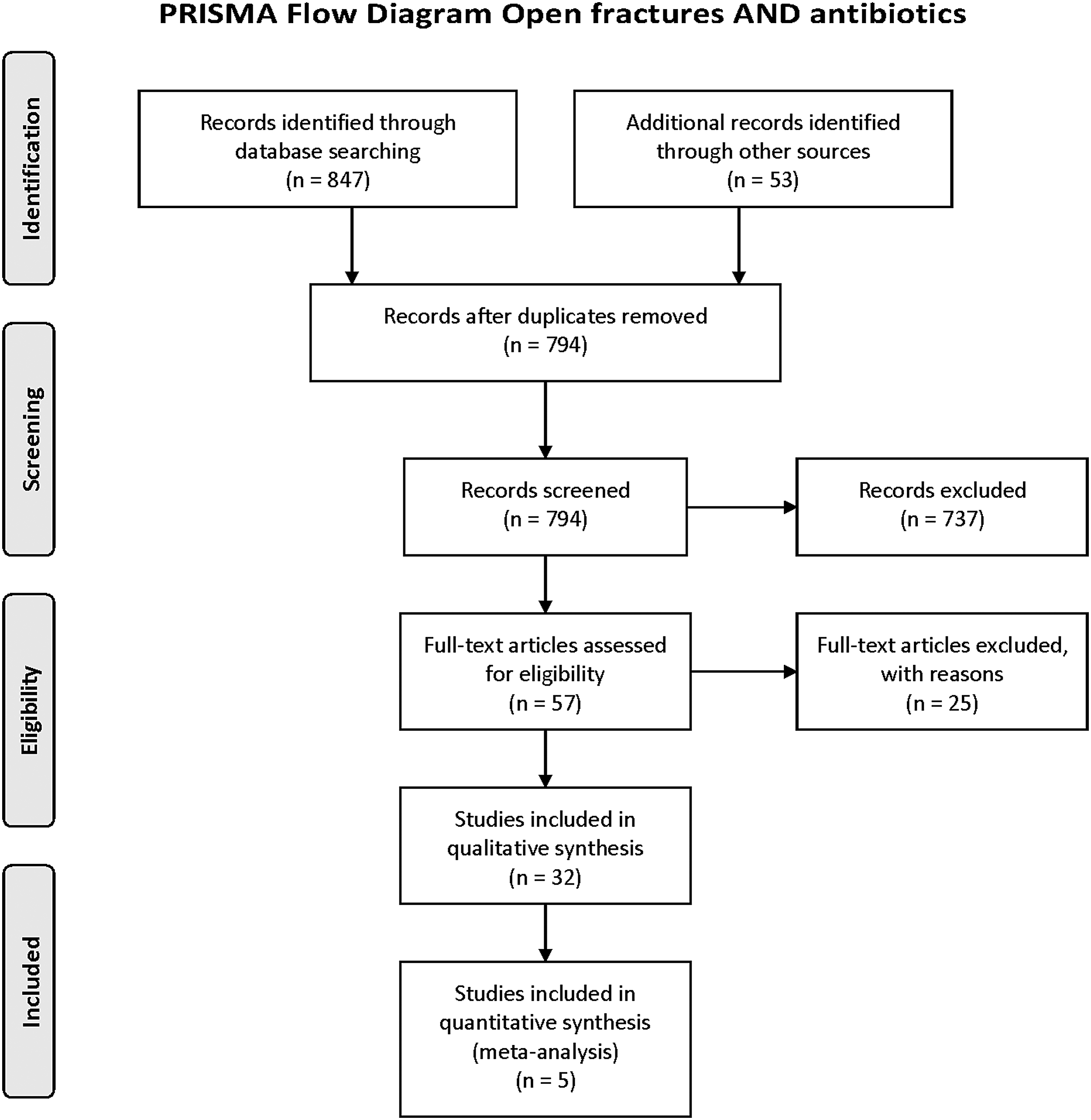
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flowchart.
Data were extracted regarding study design, patient numbers, patient demographics, antibiotic and surgical protocol, infection and complication rates. If different antibiotic duration regimens were used within a study, we split the patient populations and analyzed them separately. Both superficial and deep infections were extracted as one category. Table 2 shows a summary of all studies included, their CMS score, the various antibiotic regimes followed, the duration of administration, the study population, and the level of evidence.
pts = patients; CMS = Coleman Methodology Score; ORIF = open reduction internal fixation; Ex-fx = external fixation; IMN = intra-medullary nailing; SSG = split skin graft; BOA = British Orthopaedic Association; IV = intravenous; TBW = tension band wiring; ER = emergency room.
Number of patients/fractures relevant to our study question (not necessarily reflecting the whole study population in the publication).
Publication bias
We generated a funnel plot of infection rate for all primary comparative studies (used in the meta-analysis) to assess the likelihood of publication bias. The distribution of data points within the funnel plot was almost symmetric, implying that presence of publication bias was unlikely (Fig. 2).
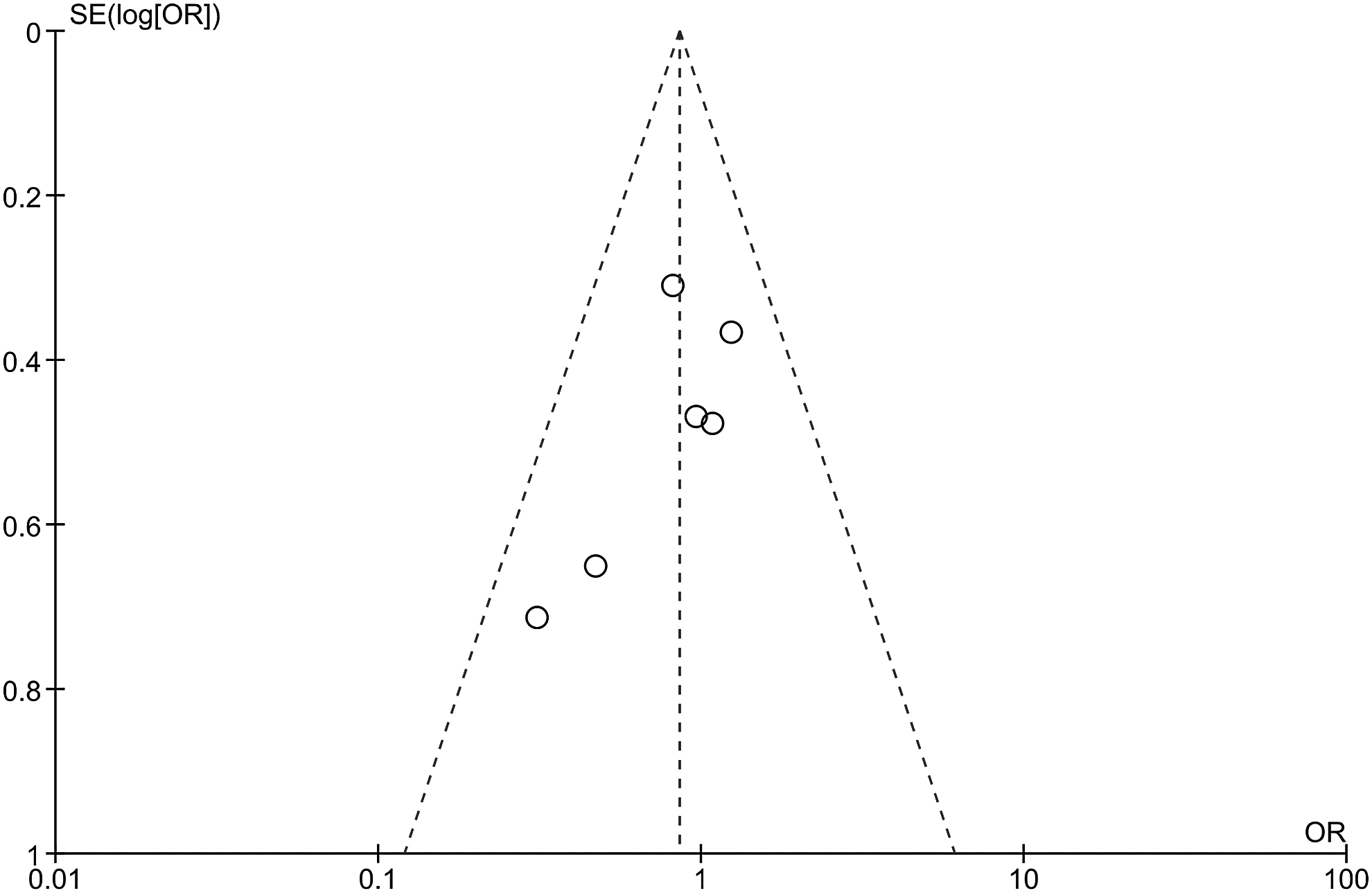
Funnel plot of the results reported to the comparative studies that were analyzed in this meta-analysis. Abs = antibiotic agents; CI = confidence interval.
Quality assessment
The CMS ranged from 27 to 88 across all primary studies (mean: 56, standard deviation: 14, median: 53). Comparative studies scored a higher score compared with non-comparative ones (Table 3). The ICC was 0.92 (95% CI: 0.81–0.99), implying a nearly perfect agreement between the two assessors.
CMS = Coleman Methodology Score; SD = standard deviation.
Infection rates
1. Comparative studies
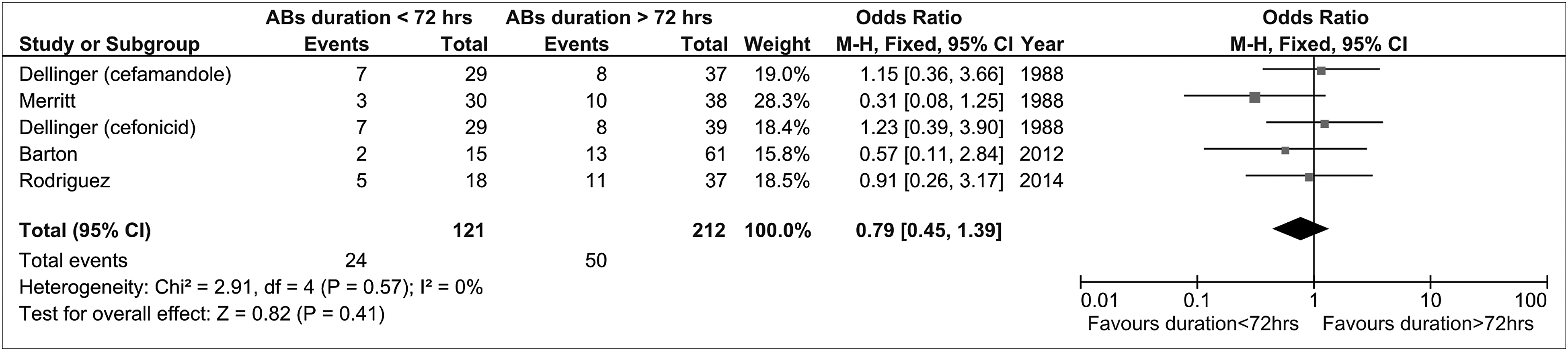
Five studies (six treatment groups) [16–20] provided relevant data. The pooled estimate of effect size for infection rate did not document any statistically significant difference between the two groups, although it seemed to favor a protocol of less than 72 hours duration of antibiotic agents (OR: 0.85, 95% CI: 0.60–1.21) in the absence of statistical heterogeneity (Q = 4.23, df: 5, p = 0.37, I2 = 0) (Fig. 3).
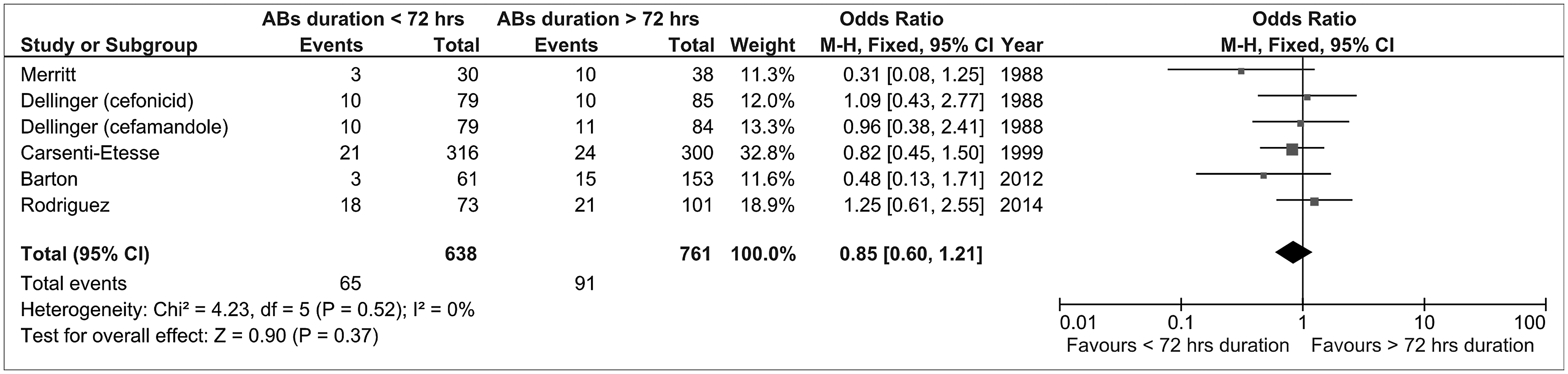
Foster plot of the results reported to the comparative studies that were analyzed in this meta-analysis. Abs = antibiotic agents; CI = confidence interval.
2. Observational studies (no comparator group)
These studies were grouped accordingly, based on the duration of antibiotic treatment of their participants either more or less than 72 hours. The group of “duration of abx >72 hrs” consisted of 15 patient populations derived from 13 studies [22,24,25,31,34,36–42,44] (Table 4). The infection rate ranged from 0%–20% (median: 6.4%) across component studies. The pooled estimate of infection rate was calculated (weighted mean of infection rate: 9.2%, 95% CI: 6.6%–12.2%), but it should be interpreted with caution, because of the presence of significant statistical heterogeneity across the primary studies (Q = 68, df: 14, p < 0.001, I2 = 80).
CI = confidence interval; df = degrees of freedom.
p = 0.53 (Mann-Whitney U test).
Random effects model.
The group of “duration of abx <72 hrs” included 14 patient populations from 13 studies [5,21,23,26–30,32,33,35,43,44]. The infection rate ranged from 2%–22% (median: 10%). The pooled analysis was deemed with significant statistical heterogeneity (Q = 96.6, df: 13, p < 0.001, I2 = 86.5) and, again, the respective results should be interpreted cautiously (weighted mean of infection rate: 10%, 95% CI: 6.8%–14%). The documented difference between the above groups was not statistically significant (p = 0.53, Mann Whitney U test) (Table 4).
Subgroup analysis
Subgroup analysis was performed in terms of Gustilo type, anatomic site of the open fractures, and shorter (<48 h) antibiotic regimes.
1. Comparative studies
These studies provided data for subgroup analysis based on the Gustilo type of open fractures. For this purpose, we stratified studies reporting on Gustilo type I + II open fractures and on Gustilo III open fractures (with no limitations per anatomic site). The results of subgroup analysis of the comparative studies are presented in Figures 4 and 5. The results did not support any advantage of duration of antibiotic treatment over 72 hours when open fractures were stratified per Gustilo type.
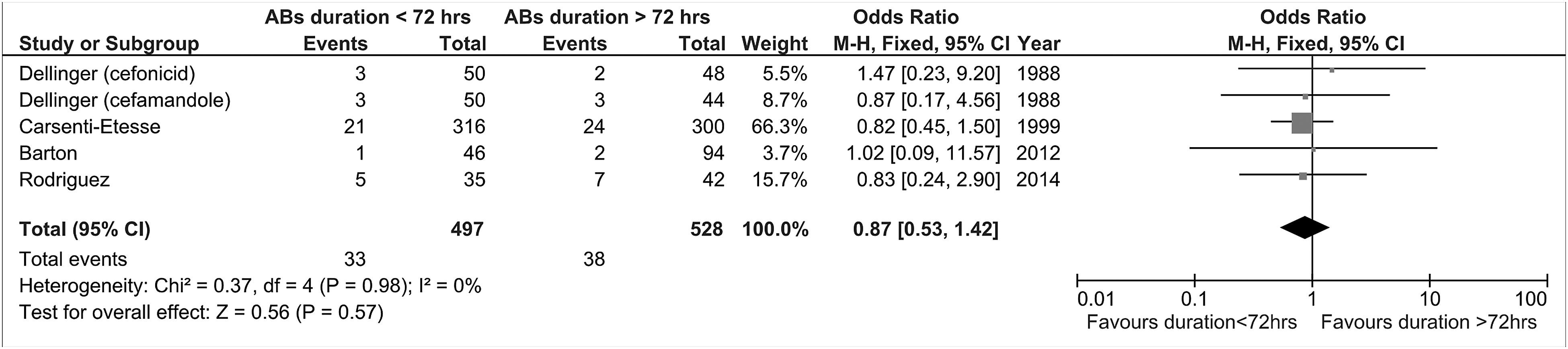
Foster plot per Gustilo classification groups of the results reported in comparative studies that were analyzed in this meta-analysis. Abs = antibiotic agents; CI = confidence interval.
Foster plot of the results reported for tibial open fractures in comparative studies that were analyzed in this meta-analysis. Abs = antibiotic agents; CI = confidence interval.
2. Observational studies
We were able to stratify them according to both the anatomic site and Gustilo type of open fracture. Concerning the anatomic site, only articles reporting on open tibial fractures were available for subgroup analysis (Table 5). The results did not favor antibiotic agent administration in excess of 72 hours (p = 0.4, Mann Whitney U test). About the Gustilo type of open fractures: An appropriate subgroup analysis was feasible, and the respective results are depicted in Tables 6 and 7. The results did not support duration of antibiotic treatment in excess of 72 hours for both Gustilo I + II (p = 0.52, Mann Whitney U test) and Gustilo III subgroups (p = 0.39, Mann Whitney U test).
CI = confidence interval; df = degrees of freedom.
p = 0.4, Wilcoxon-Rank Sum Test.
Random effects model.
df = degrees of freedom; CI = confidence interval.
p = 0.52 (Mann-Whitney U test).
Random effects model.
df = degrees of freedom; CI = confidence interval.
p = 0.39 (Mann-Whitney U test),
Random effects model
3. Shorter antibiotic prophylactic regimes
(i) Comparative studies. We directly compared regimes of “antibiotic duration less than 24 hours” with the longer regime (antibiotic duration more than 72 hours) for all open fractures (Table 8). We further stratified the results of the relevant studies based on the Gustilo type of open fractures (Fig. 6). The results did not show any clear benefit of prolonging antibiotic prophylaxis of open fractures even beyond the first 24 hours. (ii) Non-comparative studies. In this category of included studies, we were able to compare the regimes of “less than 48 hours antibiotic administration” with “more than 72 hours antibiotic administration.” The respective results are depicted in Table 9. Again, no statistically significant difference could be established between the compared groups in terms of infection rate.
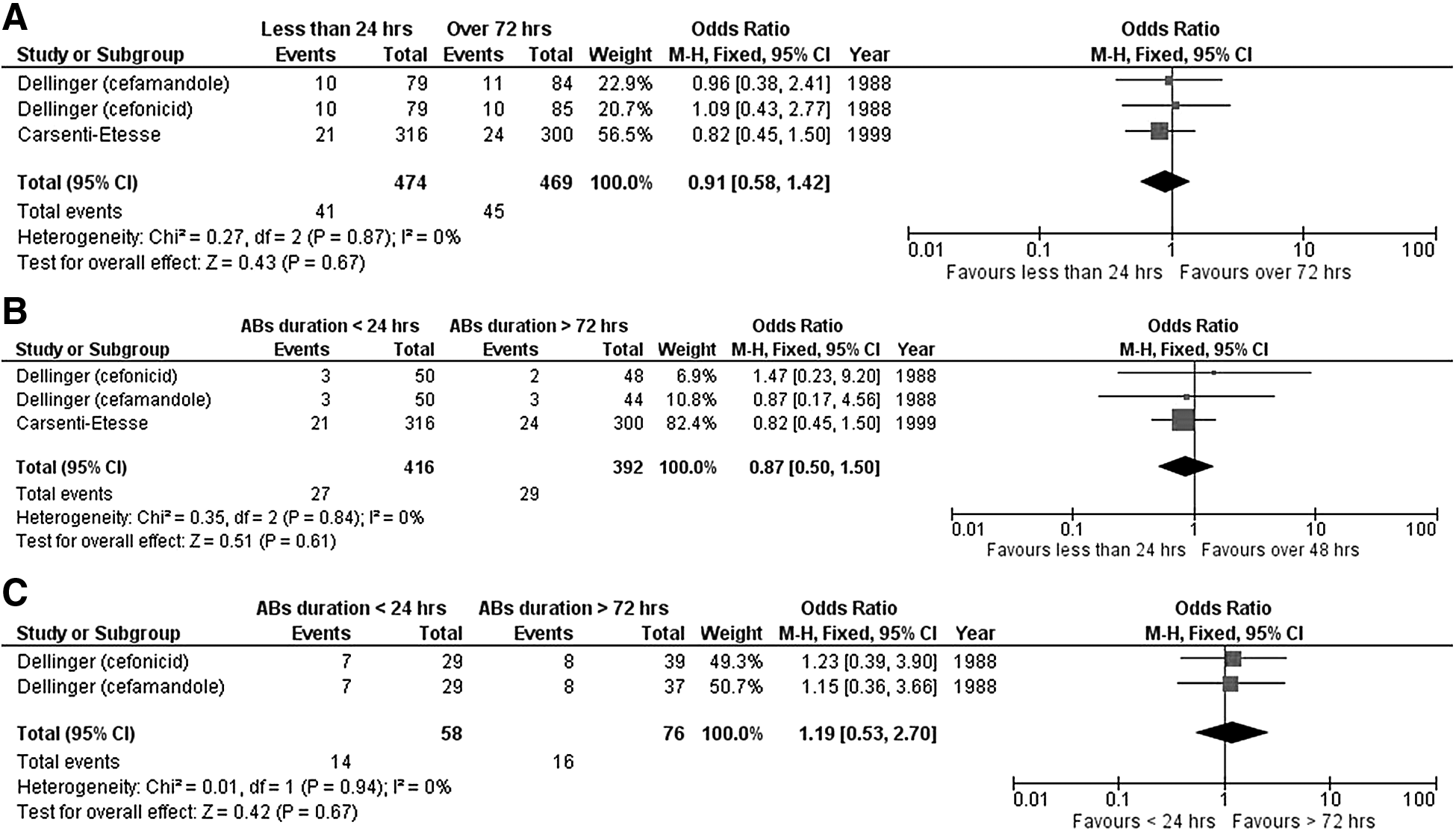
Forest plot comparing antibiotic agent administration of fewer than 24 hours against more than 72 hours for all open fractures (
CI = confidence interval.
CI = confidence interval; df = degrees of freedom.
random effects model.
Mann-Whitney U test.
For sensitivity analysis, we excluded studies that had received fewer than 40 points according to the CMS because these were regarded as methodologically weaker [27,38,41,43]. Repeat pooling analysis did not produce materially different results compared with the original ones. We have also repeated the pooling analysis after first excluding studies with outlying results [33,37]. Again, this procedure did not produce substantially different results compared with the original ones.
Discussion
This is the first meta-analysis focusing specifically on the duration of antibiotic administration in all long bone open fractures. The results from pooled analysis of both comparative and observational studies do not substantiate that prolonged (more than 72 h) antibiotic schemes in open fractures offer any benefit against septic complications.
Open fractures posed a high death occurrence and morbidity to patients before the arrival of modern antibiotic agents. Injured soldiers in wars either faced immediate amputation of the affected limb or weeklong bed rest with painful dressing changes. Both interventions were regularly complicated by severe infections, which most commonly led to the demise of the patient. The discovery of antibiotic agents and their use in open fractures reduced the infection rate significantly. The first study documenting their efficiency was published by Patzakis et al. in 1974 [45], which showed that cephalosporins reduced the infection rate by two thirds compared with placebo treatment. Ever since, various arbitrary antibiotic regimes have been used and their efficiency published in relatively small cohort studies. The time of administration, the combination of various agents, the duration of administration and their local or systemic application has been discussed widely in the literature [1].
Interestingly, almost 40 years after the publication by Patzakis et al., the duration of antibiotic treatment remains controversial. The choice of agent depends mainly on the community and hospital environment, but there is some agreement that a broad-spectrum antibiotic should be used in the emergency department whereas more specific agents are necessary in primary and subsequent surgical procedures to avoid nosocomial multi-resistant superinfection. The British Orthopaedic Association (BOA) guidelines published in 2009 [46] are based on a review article by Jaeger et al. [47], which takes previous meta-analyses and consensus publications into account. Since 2006, no further comprehensive meta-analysis has been undertaken, and this is the first meta-analysis and review focusing specifically on the duration of antibiotic administration.
We would like to suggest the elimination of the term “antibiotic prophylaxis” because it is being used in elective orthopedic practice. The nature and mechanism of an open fracture leads to a contamination of the wound site per definition, and the early administration of antibiotic agents in the emergency department has reduced the infection rate significantly [35,48,49]. This decontamination step does not need to be protracted over 72 hours, because the wound should have been debrided and irrigated [50,51], either primarily closed or covered or temporarily sealed within the first 24 hours 31,52]. Any prolongation of the initial antibiotic beyond 72 hours potentially increases the risk of nosocomial infection [53]. Vasenius et al. [44] found that resistance to the initial antibiotic was found in eight of 11 infected patients (clindamycin group) and 16 of 22 (cloxacillin group).
Many factors influence the outcome of open fracture treatment. Some paradigms are now outdated because more robust studies show that the old “six hour rule” does not apply [48]; similarly, wound swabs in the emergency department and at first surgical debridement are very poor predictors of the organism causing the subsequent infection [34]. Primary closure after thorough debridement, multi-disciplinary orthoplastic approach, and early coverage with soft tissue grafts [31] or negative pressure dressings have been shown to improve overall outcome [54].
Very little is still known about the appropriate management of heavily contaminated open fractures. There is a lack of studies specifically addressing farmyard and open water injuries. The choice of antibiotic agents is guided by local resistance profiles and varies highly among all studies.
Vasenius et al. [44] have shown that Grade III open fractures have gram-negative pathogens in 43% of cases. The BOA/British Association of Plastic, Reconstructive and Aesthetic Surgeons (BAPRAS) guidelines recommend co-amoxiclav because it has a higher bacterial kill rate than cefuroxime and offers gram-positive, gram-negative, and anaerobic cover [8]. Teicoplanin offers excellent bone penetration, covers gram-positive bacteria including methicillin-resistant Staphylococcus aureus. It has a long half-life, low toxicity, and bolus administration is possible [55].
This meta-analysis and review is limited by the lack of high-quality studies specifically looking at the duration of antibiotic administration. The only level 1a study (as per Oxford Centre of Evidence-based Medicine ranking system [56]) included in our analysis was Carsenti-Etasse et al [17]. In addition, only recent publications (5) are clearly stating their definition of infection (Centers for Disease Control and Prevention criteria) [57,58]. Geographical variations and different microbiologic environments have led to a wide spectrum of differing antibiotic regimes making direct comparison of specific antibiotic agents impossible. Treatment standards have only emerged slowly over the decades, and guidelines keep changing, which again makes analysis difficult. The inter-observer reliability of adequately grading and classifying open fractures remains another minefield. The centralization of open fracture treatment to major trauma centers in the United Kingdom will potentially increase the reliability of data.
Conclusions
Therefore, we support the recommendations by BOA/BAPRAS for open tibial fractures and recommend that they should be extended to all open long bone fractures. Because even shorter than 72 hours regimes did not lead to worse infection-related outcomes, the prolonged antibiotic administration (more than 72 h) should be abandoned. We suggest a randomized trial focusing on different duration of antibiotic treatment for the most severe variants of open fractures or those with gross contamination (fresh water open fractures, farmyard trauma, open pelvic fractures, open intra-articular fractures with exposed joints, high risk hosts (i.e., those with diabetes mellitus, immunosuppressed).
Footnotes
Author Disclosure Statement
No competing financial interests exist.