
Abstract
Abstract
Background:
Antimicrobial prophylaxis is the single most effective intervention to reduce risk of surgical site infections (SSIs); however, prescribing practices should be aligned with accepted and recommended surgical antibiotic prophylaxis (SAP) regimens to be effective. As part of a comprehensive surveillance network, SAP data are collated and analyzed for compliance with recommendations. Results are reported to hospitals for quality improvement purposes. In this study, statewide results were analyzed to ascertain changes over time and whether improved compliance was associated with a reduction in risk for SSI.
Methods:
A standardized tool for monitoring SAP and SSIs was used in Victorian healthcare facilities. For the current study, data submitted for the period 2003–2015 were analyzed. Compliance with national recommendations (Australian Therapeutic Guidelines–Antibiotic) was used as the reference standard for antibiotic selection, timing, and duration
Results:
A total of 144,075 surgical procedures were surveyed during the study period. During this period, the proportion of patients receiving antibiotic agents according to national guidelines increased. Across all surgical groups, the odds ratio (OR) for appropriate SAP choice increased by 13%/year. Greatest improvement was seen for colorectal procedures (19%/year), with the smallest change observed for cholecystectomy and cardiac operations (9%/year). The OR for receiving an antibiotic agent at the recommended time increased by 12%/year and the odds of the antibiotic agent being discontinued within 24 hours by 27%/year. Non-compliance with a recommended SAP agent and timing was associated with an increased risk of SSI across all procedure groups (OR 1.33, 95% confidence interval 1.24–1.43).
Conclusion:
Sustained improvements in prescribing practices for SAP have been demonstrated through a comprehensive surveillance and reporting system. Non-compliance with SAP guidelines is associated with an increased risk for SSI. Quality improvement programs must focus on uptake and implementation of evidence-based guidelines.
T
Surgical antibiotic prophylaxis (SAP) has been demonstrated to be an effective intervention to reduce the incidence of surgical site infections (SSIs) after a broad range of surgical procedures [3–5]. For optimal effect, SAP must be appropriately administered in terms of antibiotic agent selection, timing of administration, and dosing [6,7]. Further, to reduce risks for antimicrobial resistance and other complications such as Clostridium difficile diarrhea, duration of prophylaxis should not be prolonged post-operatively.
Australia has national guidelines for administration of antibiotic agents (Therapeutic Guidelines–Antibiotic), which are based on international recommendations for evidence-based practice [8]. These are endorsed by clinicians, widely available, and are published online and as a hard copy publication. Many hospitals develop local protocols for SAP based on these guidelines [9].
VICNISS collates SAP data as part of routine SSI surveillance [10,11] to facilitate feedback to local quality improvement programs. The objectives of this study were to evaluate SAP data collated by the VICNISS coordinating center between 2003 and 2015 to determine: (1) whether current clinical practice reflects national guidelines regarding SAP, (2) time trends regarding uptake of national guidelines regarding SAP, and (3) whether improved compliance is associated with a reduction in risk for SSI.
Methods
SAP and SSI surveillance data routinely captured by participating centers for the period January 1, 2003 to December 31, 2015 were analyzed retrospectively for the current study.
Participating hospitals
All public hospitals with more than 100 acute beds in Victoria are required to participate in surgical site surveillance depending on types of surgical procedures performed [10]. All hospitals in which cardiac operations are performed (n = 6) and all those in which ≥50 hip or knee procedures are performed annually (n = 31) are required to conduct continuous surveillance [12,13]. Surveillance of other surgical procedures is voluntary. For colorectal operations, a total of 13 hospitals participated in surveillance (average of 8/year). For cholecystectomy, 15 hospitals participated in surveillance (average of 4.8/year). For hysterectomy, there were 11 participating hospitals (average of 4.3/year). Nine private hospitals participated in the VICNISS program during the study period, contributing data to the cardiac and orthopedic datasets since 2009.
Data are collected by trained infection control consultants and are obtained from the medical records of patients undergoing surgical procedures nominated for surveillance. Data are submitted to the coordinating center electronically. The VICNISS staff members provide regular education and support (webinars, seminars, online credentialing, e-mail and telephone contact for individual case-based queries) to hospital surveillance staff to ensure standardization of surveillance methods. All participating hospitals are contacted quarterly specifically regarding data validation; this includes checks of qualitative and quantitative attributes. Formal validation studies have been published [14].
Surgical procedures
The VICNISS surveillance utilizes surgical groups defined according to NHSN surveillance methods [15]. For the current study, surgical groups involving a common anatomic site or comparable procedure were combined where national recommendations for prophylaxis were aligned. For example, all cardiac surgical procedures (cardiac bypass and other cardiac operations) were analyzed as a single group, and hip and knee replacements were combined. Colon and rectal surgical procedures were also evaluated as a single group, and vaginal and abdominal hysterectomy procedures were evaluated as a common set.
Definitions
Compliance assessment—antibiotic agent selection
Designation of optimal was based on concordance with the current version of national antibiotic agent prescribing guidelines at the time of reporting (see Supplementary Appendix 1; see online supplementary material at ftp.liebertpub.com). Where antibiotic agent selection was not concordant with the guidelines but included agents active against the most likely pathogen(s) for SSIs for the procedure, it was assessed as “not concordant but adequate,” subsequently referred to as adequate. This category was also used where a broad-spectrum agent was given when guidelines recommended use of a narrow-spectrum agent. Antibiotic agent selection was deemed inadequate if the selection did not include agents active against the most likely pathogen(s) for that procedure or if no antibiotic agent was administered where recommended.
Designations of adequate and inadequate were made based on a consensus view of two infectious disease physicians within the VICNISS Coordinating Center and one infectious disease physician independent of the center. Patients receiving antibiotic agents during the pre-operative period were considered to have received prophylaxis if the agent (s) were concordant with national guidelines.
Compliance assessment—antibiotic agent timing
Timing of administration was assessed by comparing the timing of administration of the first dose of antibiotic agent with the recorded time of the surgical incision. The surveillance tool allows continuous or categorical data to be captured for timing depending on which is available (e.g., exact time of drug administration or nomination of drug delivery as “after incision”). Apart from vancomycin, timing was considered to be concordant if the antibiotic agent was administered within 60 minutes before incision (exact times) or “on induction” or “within one hour before incision”; otherwise, it was deemed non-concordant. Vancomycin was considered to be concordant if the infusion was started at least 30 minutes before the procedure. Where exact time was not able to be determined, “within one hour of procedure” was also considered concordant.
Compliance assessment—duration of antibiotic prophylaxis
Guidelines recommend completion of prophylaxis within 24 hours of incision for all surgical procedures included in this study. Duration was assessed as concordant if discontinued within 24 hours and non-concordant if continued beyond 24 hours.
Dosing was not assessed in this study because compliance consistently shows 95% or greater concordance with national guidelines.
Ethics review
No patient-identifying data are captured for the purposes of the surveillance, which is considered a quality assurance activity. All hospital-level data were de-identified for the current study. As a quality-assurance audit without direct impact on patient care, ethics review was not required.
Data analysis
Data were stored in a Microsoft SQL server database and analyzed using Stata version 12 (Statacorp, College Station, TX). Trends were analyzed using a mixed effects logistic regression model, clustered on the patient to adjust for individual patients contributing multiple procedures to the dataset with the hospital site included as a random effect to account for factors such as case mix. Association of risk for SSI with non-compliance for antibiotic prophylaxis was assessed using logistic regression clustered on the patient using SSI (all infections meeting the definition of a superficial, deep, or organ space infection) as the outcome variable.
Results
A total of 144,075 procedures were evaluated through the surveillance network, comprising cardiac (n = 30,261), orthopedic (n = 87,009), colorectal (n = 12,259), cholecystectomy (n = 6,403) and hysterectomy (n = 8,143) procedures.
Compliance with national prescribing guidelines
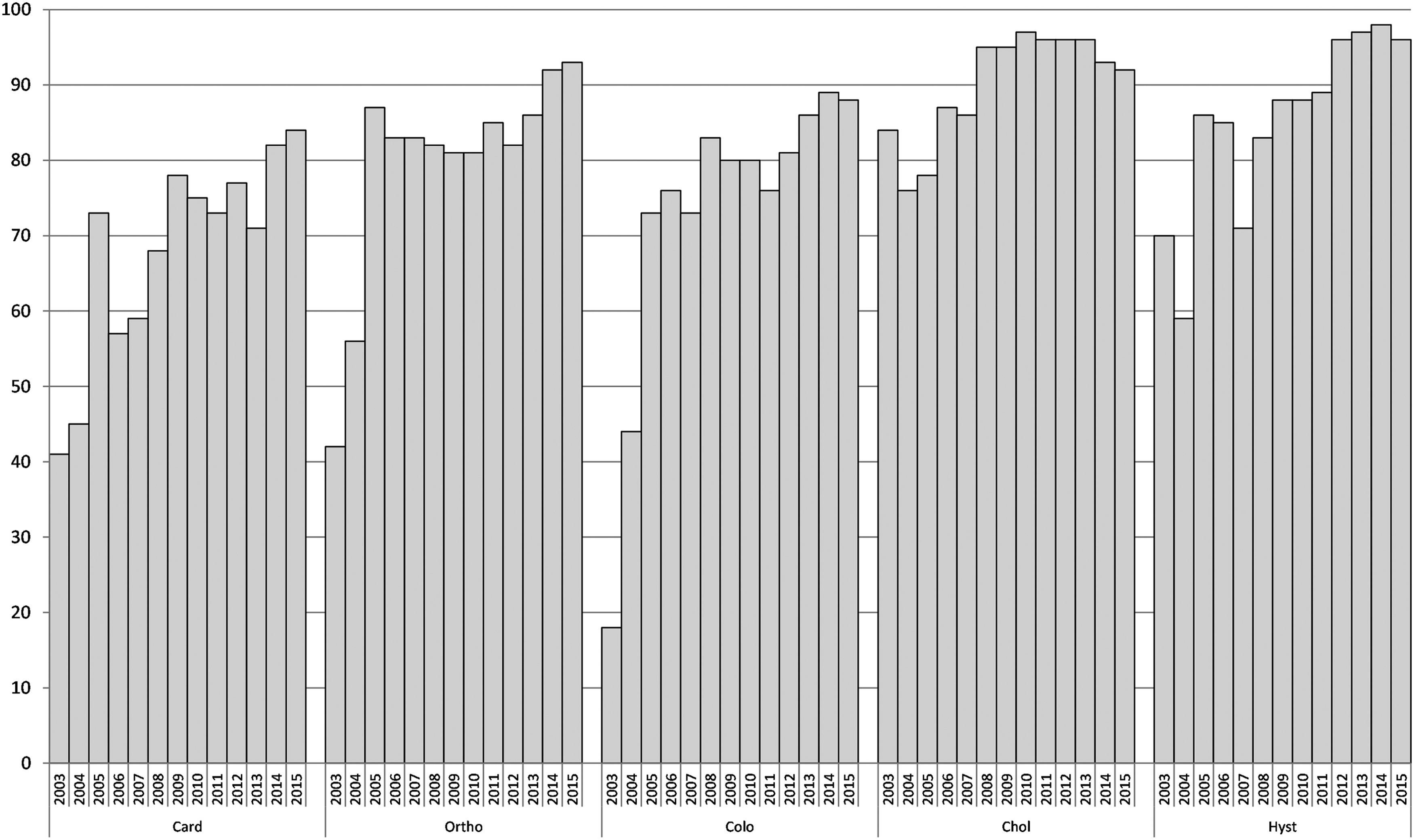
Increases in both optimal and adequate prescribing patterns were observed for all procedure groups throughout the studied time frame. Between 2003 and 2015, the overall percentage of procedures prescribed optimal choice of agent increased from 53% to 79% and those prescribed either optimal or adequate from 74% to 96%. Figure 1 shows annual compliance with guidelines according to procedure group.

Annual percentage of surgical procedures IN WHICH prophylactic antibiotic AGENT selection was optimal or adequate, by procedure group (2003–2015). Surgical procedures: Card = cardiac; Ortho = orthopedic; Colo = colorectal; Chol = cholecystectomy; Hyst = hysterectomy. Adequate  Optimal.
Optimal.
Timing of administration of the first dose of antibiotic agent was concordant with guidelines in 76% of procedures over the studied period. Figure 2 illustrates the annual percentage of procedures for which timing of prophylaxis was consistent with guidelines. While improvement was demonstrated in all groups, this was greatest for cardiac and cholecystectomy procedures (where compliance increased from 25% to 70%, and 15% to 74%, respectively). Figure 3 summarizes the percentage of procedures in which duration of prophylaxis was less than 24 hours. All procedure groups demonstrated increased compliance with guidelines over time, particularly cardiac and colorectal operations, where compliance increased twofold after commencement of the surveillance network.

Percentage of surgical procedures in which timing of administration of first dose was concordant with guidelines, by procedure group (2003–2015). Surgical procedures: Card = cardiac; Ortho = orthopedic; Colo = colorectal; Chol = cholecystectomy; Hyst = hysterectomy.
Percentage of surgical procedures in which post-operative duration of antibiotic prophylaxis was less than 24 hours, by procedure group (2003–2015). Surgical procedures: Card = cardiac; Ortho = orthopedic; Colo = colorectal; Chol = cholecystectomy; Hyst = hysterectomy.
For timing of the initial dose, there were statistically significant improvements in compliance for all surgical groups except hysterectomy (Table 1), and for duration, statistically significant improvements were demonstrated in all surgical groups.
OR = odds ratio; CI = confidence interval.
Data collection optional for these groups; therefore, data not continuously collected by all eligible hospitals.
Optimal choice defined as antibiotic agent corresponding exactly with national prescribing guideline [8].
Overall compliance for the three measures (allowing selection to be adequate or optimal) increased for all studied procedure groups. Across all three groups, compliance increased from 17.2% of 1122 procedures in 2003 to 73.5% of 10,256 procedures in 2015. Compliance with guidelines for antibiotic prophylaxis was lowest for cardiac and colorectal surgical procedures (58.7% and 59.8%, respectively).
Time trends in prescribing practices
Table 1 lists annual odds of receiving optimal and inadequate selection of antibiotic agent, by surgical procedure group. Improvements in optimal choice were reported for orthopedic surgical procedures (62% to 86%), colorectal operations (47% to 67%), and hysterectomies (41% to 71%). For all groups except cholecystectomy, a decrease in the odds of receiving inadequate prophylaxis was observed annually. The largest improvements were reported in cardiac operations and hysterectomies, where odds of receiving inadequate prophylaxis deceased significantly each year (22% and 25% decrease, respectively).
Association between compliance and SSI
Selection of optimal or adequate prophylactic antibiotic agent was associated with a significant reduction in risk for SSI when all procedures were combined (odds ratio [OR] 0.78) (Table 2). Analysis by procedure group revealed that appropriate antibiotic agent choice was protective for development of SSI after colorectal surgical procedures and cholecystectomy. Inappropriate timing of administration was associated with an increased risk of SSI when data for all procedures were combined (OR 1.2). When analyzed by procedure group, the strongest associations were for orthopedic and colorectal surgical procedures (OR 1.32 and 1.22, respectively).
OR = odds ratio; CI = confidence interval.
Data collection optional for these groups; therefore, not continuously collected by all eligible hospitals.
Analyzing the factors together, there was increased risk of infection when antibiotic agent choice was inadequate and timing was not compliant with guidelines (OR 1.33, 95% CI 1.24–1.43) for all procedures combined. Infection risk was higher for all procedure groups except for cardiac where no association was demonstrated. The trend was not statistically significant for hysterectomy and cholecystectomy procedures (Table 2).
Discussion
Our Australian surveillance network is one of the largest available internationally for examining the relationship between antibiotic prophylaxis and risk of SSI. Findings demonstrate substantial and sustained improved compliance with prescribing guidelines spanning a 13-year period, and include a broad range of surgical procedures. In addition, the efficacy of antibiotic prophylaxis was demonstrated, with optimal/adequate choice of prophylactic agent and appropriate timing of administration associated with reduced infection risk. These findings have direct implications for hospital quality improvement programs focused on standardization of prescribing practices and processes to enhance adequate timing of antibiotic agent administration.
During the study period, contemporaneous reports on compliance with antibiotic selection, timing of administration of initial dose, and duration of prophylaxis were available at least quarterly to participating facilities. Benchmarking of local (hospital) data with aggregate data is available to all participating hospitals through a secure online portal. Hospitals also have the option to collect data at the surgeon/anesthetist level. Since commencement of the program in 2003, improvements have been demonstrated in all three indicators as well as in overall compliance.
Importantly, compliance with recommended antibiotic agent was associated with a reduction in risk for SSI. When specific procedures were analyzed, the procedures that showed appreciable reduced risk for post-operative infection were cholecystectomy and colorectal surgical procedures. This association cannot be shown to be causal; however, the result is consistent with previous findings that administration of antibiotic prophylaxis is an important intervention for prevention of SSIs.
For most procedures surveyed (excluding colorectal operations), the most recent data demonstrate that selection of antibiotic agents is adequate or optimal at least 90% of the time. Large improvements were seen in the optimal category for orthopedic operations, which improved from 62% (2003) to 86% (2015). Prescribing practices also improved for cardiac surgical procedures, with compliance increasing from 47% to 67%. Compliance with guidelines was initially low for hysterectomies, then improved to around 65%, followed by a reduction to just over 20%. The explanation for this is that until 2014, a two-drug regimen including a β-lactam plus metronidazole was recommended in the national guideline for both vaginal and abdominal hysterectomies, and this was not fully supported locally by surgeons. In 2014, recommendations were revised to a single β-lactam agent for abdominal hysterectomies.
Analysis of time trends demonstrated annual increases in the odds of receiving optimal antibiotic choice for all categories of surgical procedures with each year since the commencement of the program, consistent with greater awareness and uptake of national guidelines. Our results compare favorably with the results published elsewhere in Australia [16] that showed overall adherence of 16.5% and 19.5% at two hospitals on randomly selected abdominal general surgical procedures performed during 2013–2014 [17]. The current study showed 44% adherence for equivalent procedures performed in Victoria. We have not specifically evaluated the reasons for improvements seen in our region, but believe that the feedback of surveillance findings and education of stakeholders to be pivotal [17,18], together with a national focus on antimicrobial stewardship programs [19]. A formal requirement for hospitals to have an antimicrobial stewardship program was incorporated into the hospital accreditation process in 2013, although there is evidence that antimicrobial stewardship (AMS) programs are less developed currently in the private sector, when compared with the public sector [20].
Limitations to the current study include, first, the extent to which “optimal” and “adequate” prescribing can be evaluated individually. We were interested particularly to examine changes in the optimal choice category, where antibiotic agent choice was aligned directly with the guidelines. No patient data were collected on factors such as the presence of antibiotic allergies, which may influence the choice of prophylactic antibiotic agent. The likely result is that the reported optimal category is underestimated. Second, there are limitations regarding the degree to which the timing of vancomycin administration can be analyzed. While national guidelines recommend slow infusion to be completed just before induction of anesthesia, monitoring of this time is impractical at many healthcare facilities in our region. As a pragmatic alternative, the start time of infusion is recorded as being at least 30 minutes before incision.
Despite demonstrated improvement in prescribing practices over time, compliance with all measures (agent, timing, and duration) remained low for some surgical categories. In particular, timing of administration was still suboptimal, particularly for vancomycin, and extended duration remains relatively high, particularly for cardiac surgical procedures. We have also identified second dosing of β-lactam agents as an area to target for future work. Identification of these gaps is an important step to guide future quality improvement programs in hospitals within our network.
Timing and second dosing may be areas that can be addressed with electronic prescribing and anesthetic equipment, which can store data and produce alerts when, for example, second doses of antibiotic agents are required. Introduction of equipment that supports data storage and transfer will also reduce the burden of data collection and transcription for collation of data such as those used in this study as well as routine surveillance data.
Conclusion
We have identified significant and sustained improvements in prescribing practices for SAP across a network of hospitals after the feedback of results as part of a routine surveillance program. Further improvement in prescribing practices may still be necessary, particularly with respect to timing of antibiotic agent administration for cardiac and colorectal surgical procedures. Specific quality improvement programs may be required to engage clinicians responsible for health service delivery within these groups.
Footnotes
Acknowledgments
The VICNISS Coordinating Centre is fully funded by the Victorian Department of Health and Human Services. The authors would like to thank all of the contributing hospitals and in particular the infection control practitioners. No external funding was used for the current study.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.