
Abstract
Abstract
Background:
Recent data suggest that treatment of acute, uncomplicated appendicitis (AUA) with antibiotics is as effective as surgery. A 2015 study indicated that more than 50% of patients would choose antibiotic therapy. Medical students represent a unique population of potential patients with greater medical knowledge than the general public and possibly less bias than practicing physicians. Therefore, we aimed to evaluate what the MEDICAL STUDENT'S treatment choice for AUA would be and what factors influence these decisions.
Methods:
We conducted a survey of current medical students at a single institution. Survey data included demographics, interest in surgery or a procedure-related specialty, knowledge of and experience with surgery and antibiotics, and concerns about treatments. A summary of the literature regarding the efficacy and safety of antibiotics and surgery was presented. Each participant was asked which treatment he or she would choose if affected by AUA.
Results:
A series of 255 medical students completed the survey (mean age 24.8 ± 2.4 y; 51.5% female). The largest number of respondents (41.2%) were second-year students, and more than half (54.2%) reported an interest in a procedure-related specialty. Nearly all (93%) reported prior antibiotic use (19% reporting adverse effects), and 50% had prior surgery (20% reporting adverse events). When asked to identify concerns about each treatment choice, “surgical complications” was selected most frequently (82%) for surgery, and “adverse events and side effects” was selected most frequently for antibiotics (57%). When asked how they would treat their own AUA, 66.3% selected surgery, 24.3% selected antibiotics, and 9.4% were unsure. Race, gender, specialty of interest, year of training, and history of adverse effects related to antibiotics or surgery were not significantly related to treatment choice (all p > 0.1).
Conclusion:
When informed of the benefits and risks of surgery and antibiotics to treat AUA, medical students in our study were more likely to choose surgery.
A
Multiple randomized trials have compared medical and surgical management. However, drawing definitive conclusions from these studies is difficult, as each study had a different definition of “non-inferiority” when comparing antibiotics with appendectomy; and the results and conclusions of each study differ greatly [9]. Therefore, the risks and benefits of either option must be weighed by both patient and physician. A 2015 survey conducted at another institution found that when a random sample of patients, visitors, and employees in a hospital were asked which treatment they would prefer for AUA, the majority selected antibiotics over appendectomy [10]. However, only 51% of participants correctly identified what and where the appendix was, 43% correctly defined appendicitis, and none of the participants was informed of the benefits and risks of each treatment option. Although patients seem to be interested in substituting antibiotics for surgery, they must be well-informed about each option in order to provide informed consent [11].
Medical students represent a unique population of potential patients with greater medical knowledge than the general public. It also is possible that they have less bias choosing a treatment for appendicitis than practicing physicians, as they are early in their training and have had less exposure to historical medical dogma. Therefore, we aimed to evaluate their treatment choice for AUA and the factors potentially influencing their decision. We hypothesized that medical students would be more likely to select surgery over antibiotics, and that those students interested in a procedure-oriented specialty would be more likely to choose surgical intervention than those interested in a non-procedure-oriented specialty. This hypothesis was based on the fact that medical students are taught the pathophysiology and traditional surgical treatment of appendicitis, and that students interested in a surgical specialty may have more exposure to, and bias toward, a surgical approach to management.
Patients and Methods
After receiving Institutional Review Board approval, a recruitment e-mail and survey were approved by the Case Western Reserve School of Medicine administration to send to all medical students class e-mail list-servers (Table 1). The survey was sent to all currently enrolled medical students, including MD/PhD students and other students not currently enrolled in the standard four-year curriculum. The survey was sent on November 14, 2016, and remained open for one week. Within this period, students were reminded once via e-mail and once in person to complete the survey.
Survey responses were anonymous, and all questions in the survey were optional. Subjects' information included demographics, level of training, and future career interest. Responses were divided into procedure-oriented (surgery or surgical subspecialty, obstetrics and gynecology, anesthesiology, or internal medicine with a procedural-oriented subspecialty) and not procedure-oriented (family medicine, pathology, radiology, neurology, pediatrics, physical medicine and rehabilitation, psychiatry, or internal medicine with a non-procedure-oriented subspecialty). Subjects were asked to report prior antibiotic use and surgical history, as well as any adverse events related to either experience. Baseline knowledge of appendicitis and its management was assessed, and subjects indicated whether they or a family member had ever had appendicitis and how it was managed. We provided students with a list of potential risks associated with surgery or antibiotics and asked them to select the three most worrisome risks for each treatment.
Students were directed to a summary statement that explained the evolution of appendicitis management and presented recent data regarding the risks and benefits of both appendectomy and antibiotic treatment (Table 1). Finally, students were given a hypothetical scenario of AUA and asked how they would elect to be managed themselves considering the data provided.
For statistical analysis, continuous variables were compared using two-sided Student t-tests and reported as a mean (± standard deviation) or median (interquartile range). Nominal variables were compared using the χ2 test or the Fisher exact test where appropriate. Statistical significance was defined as a p value <0.05. All analyses were completed using Stata/SE 14.2 (StataCorp, College Station, TX).
Results
There were 255 responses to the 739 surveys sent (34.5%). The largest number of responses came from second-year students (41.2%), and the majority of respondents were Caucasian, with a race make-up reflective of the student body (Table 2). Although interest in both procedural and non-procedural specialties was well represented, students were more likely to be interested in a procedural specialty by a margin of about 8%. Nearly all students indicated that they knew the meaning of appendicitis; only 2% admitted to being “not sure.”
With regard to student medical history, about half reported prior surgery requiring general anesthesia, and almost all students had used antibiotics (Table 3). Nineteen percent of antibiotic users reported adverse events related to the medication, and 20% of those with a surgical history reported adverse events related to the procedure. Examples of adverse events associated with antibiotics were gastrointestinal upset, nausea and vomiting, Clostridium difficile infection, allergic reaction, and yeast infection. Examples of adverse events related to surgery were post-operative infection, cardiac arrest, poor reactions to anesthesia and pain medications, and severe post-operative pain.
Most students selected at least one concern for each treatment option, but more students indicated “no concerns” about antibiotics than about surgery (Table 3). The distribution of students' selections for concerns related to each treatment choice is demonstrated in Figures 1 and 2. The most commonly selected concern for surgery was “surgical complications” and for antibiotics was “side effects.”

Specific concerns about having surgery.
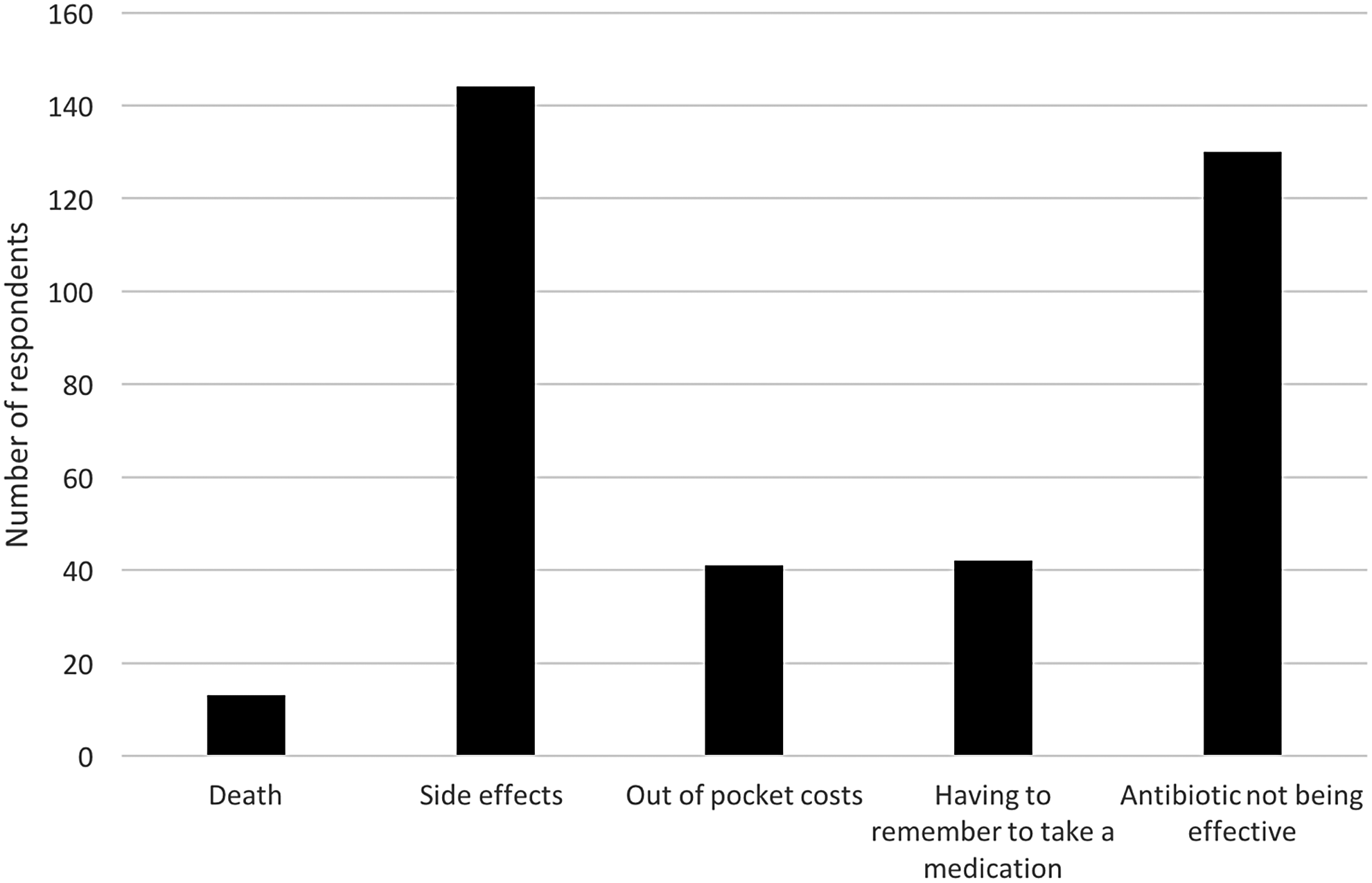
Specific concerns about taking antibiotics.
After considering the hypothetical AUA scenario and literature on treatment to students, 66.3% opted to have surgery, 24.3% selected antibiotics, and 9.4% were undecided. Neither race (p = 0.4), gender (p = 0.3), nor year of training (p = 1.0) had a statistically significant relation to treatment preference. Adverse effects or events related to past antibiotic use (p = 0.2) or past surgery (p = 0.1) likewise did not predict the treatment selected. Finally, there was no significant association between specialty interest and treatment preference (Table 4).
Discussion
This study demonstrates that when presented with data regarding AUA, most medical students would prefer to undergo surgery rather than have medical management. There was no significant association between gender, race, year of training, relevant medical and surgical history, or specialty of interest and treatment preference.
One other study has surveyed potential patients to assess opinions on medical versus surgical management of appendicitis. The aforementioned study surveyed random individuals in a hospital and found that the majority of respondents would opt for antibiotics rather than appendectomy [10]. However 49% of the respondents did not know what and where the appendix was, and the majority of the participants could not define appendicitis accurately. When presented with the choice of treatment, survey-takers were told that “existing studies comparing antibiotics with surgery suggest that appendicitis can be treated safely with antibiotic therapy alone.” Thus, it is unlikely that the decisions of the participants were informed.
In contrast, most of our respondents were familiar with the anatomy of the appendix and the pathophysiology of appendicitis. Additionally, our survey document informed respondents of the risks and benefits of each treatment by providing more specific data from the current literature (see Table 1). These two factors likely account for the difference between our results and those of the previous study and highlight the idea that with greater medical literacy, patients might make a different choice. Moving even further along the spectrum of medical education, physicians are biased in favor of treatment utilizing their specialty-specific modality [12–14]. In each of the cited studies, surgeons were more willing than both other physicians and patients to proceed with surgery in clinical scenarios (pulmonary nodules, soft-tissue sarcoma, ulcerative colitis) where either medical or expectant management are the options. In our study, the specialty of interest did not correlate with treatment preference. This suggests that our subjects, although more likely to opt for surgery than the general population, may not be as biased as graduate physicians.
The findings of this study have important implications for both physician and patient education. Because medical students receive extensive education regarding different treatment modalities and have greater insight into the benefits and risks of each, they represent a unique informed consent situation. The majority of respondents in this study opted for appendectomy. This is in contrast to the published study of random visitors in a hospital. which found a majority preference for antibiotics. In scenarios where multiple treatment options are appropriate and equivalent, it is less important which treatment the patient chooses and more important that the patient is adequately equipped to make that choice [15,16]. Considering the results of this study in the context of others that have assessed a given population's preference for medical versus surgical management of different diseases, there appears to be a spectrum of choice. On one end of this spectrum is the general population, which typically opts to avoid surgery when possible. On the opposite end is surgeons, who typically opt to proceed with surgery when feasible. Medical students lie somewhere between these two ends, but closer to the point where surgeons lie, with a majority opting for surgery yet 35% either unsure or preferring medical management in this study. Future directions based on this study might include repeating this survey with individuals more advanced in their medical training (residents, practicing surgeons) to identify potential areas of provider bias, conducting a larger study of the general population to see how the results would differ if they were to be informed in a manner similar to the one used in this study, and developing better models of informed consent for real patients faced with the decision of how to treat AUA.
We acknowledge there are limitations to this study. The views of medical students may not be generalizable to the typical patient presenting with acute appendicitis. Also, although we received 255 responses, about two thirds of the student body did not take the survey. Nevertheless, this response rate is similar to that observed in other survey studies polling physicians and residents [17,18]. We attempted to make the survey brief in order to maximize the response rate, realizing that polling a group of medical students during the school year would be particularly difficult. There was a noticeable lack of responses from third- and fourth-year students, which we believe may make our results more generalizable to a typical patient population, as first- and second-year students have had less clinical exposure. However, our results are likely less generalizable to upper-level medical students. Survey respondents may have known the researchers involved in this study, but the survey included no identifying information, so there would be minimal influence of this knowledge on the students to respond a certain way. The manner in which the summary data regarding each treatment arm were presented may have influenced answers, because some of the investigators involved in this project are surgeons, and many medical students are part of the surgery interest group. However, we aimed to frame this information in a neutral manner by providing similar data points for each choice. It should be noted also that although we attempted to summarize the literature and emerging controversy on this topic to inform students to a sufficient extent, presenting a more thorough literature review and including the deeper nuances of the issue might have changed students' answers. Additionally, survey responses to a hypothetical scenario may not correlate with real-life medical decisions.
Despite these limitations, this study surveys one population that simultaneously represents both potential patients and future physicians and provides new data on how the management of AUA may evolve by incorporating patient preference. Whereas several studies have compared the relative efficacy of antibiotics and appendectomy, few studies have surveyed patients about their preferences on this topic; and no studies that we are aware of have surveyed medical students in particular. Our results demonstrate how increasing medical knowledge may impact preference, and that even at this level, there still were 35% of potential patients who either were interested in antibiotics or unsure how they would proceed. These data may be taken into consideration by physicians when discussing the treatment options for appendicitis with their patients, as there clearly is patient interest in non-operative management.
Conclusion
This survey study at a U.S. medical school found that two of three students preferred appendectomy to treat AUA. Further study is warranted to assess which factors, if any, influence why certain individuals or demographics select one treatment over the other. It also is unknown how often physicians are offering their patients antibiotics, but perhaps these data will encourage more physicians to approach this topic with their patients.
Footnotes
Author Disclosure Statement
None of the authors of this manuscript has any disclosures to make.
All authors made substantial contributions to conception and design, and/or acquisition of data, and/or analysis and interpretation of data; participated in drafting the article or revising it critically for important intellectual content; and gave final approval of the version to be submitted and the revised version to be published.