
Abstract
Abstract
Background:
Surgical site infections (SSIs) are the leading cause of hospital-acquired infections and are associated with substantial healthcare costs, with increased morbidity and mortality. To investigate the effects of the antibiotic stewardship program on prevention and control of SSI during clean surgery, we investigated this situation in our institution.
Patients and Methods:
We performed a quasi-experimental study to compare the effect before and after the antibiotic stewardship program intervention. During the pre-intervention stage (January 1, 2010 through December 31, 2011), comprehensive surveillance was performed to determine the SSI baseline data. In the second stage (January 1, 2012 through December 31, 2016), an infectious diseases physician and an infection control practitioner identified the surgical patients daily and followed up on the duration of antimicrobial prophylaxis.
Results:
From January 1, 2010 to December 31, 2016, 41,426 patients underwent clean surgeries in a grade III, class A hospital. The rate of prophylactic antibiotic use in the 41,426 clean surgeries was reduced from 82.9% to 28.0% after the interventions. The rate of antibiotic agents administered within 120 minutes of the first incision increased from 20.8% to 85.1%. The rate at which prophylactic antimicrobial agents were discontinued in the first 24 hours after surgery increased from 22.1% to 60.4%. Appropriate antibiotic selection increased from 37.0% to 93.6%. Prophylactic antibiotic re-dosing increased from 3.8% to 64.8%. The SSI rate decreased from 0.7% to 0.5% (p < 0.05). The pathogen detection rate increased from 16.7% up to 41.8% after intervention. The intensity of antibiotic consumption reduced from 74.9 defined daily doses (DDDs) per 100 bed-days to 34.2 DDDs per 100 bed-days after the interventions.
Conclusion:
Long-term and continuous antibiotic stewardship programs have important effects on the prevention and control of SSI during clean surgery.
S
Recently, several countries have proposed guidelines [15,16] that state that appropriate antibiotic use is one of the most important methods for SSI prevention and control. In 2002, the Centers for Medicare & Medicaid Services (CMS) conducted the Surgical Infection Prevention Project (SIP) and proposed three measures [17] that promoted appropriate antibiotic use for SSI prevention and control; many medical organizations have controlled the incidence of SSI by using these measures [18]. The introduction of antimicrobial prophylaxis has resulted in the reduction of SSIs. Surgical antimicrobial prophylaxis (SAP) refers to a brief course of antibiotic prophylaxis given just before surgery. Guidelines for antibiotic prophylaxis have been designed worldwide to advocate the proper use of SAP. To decrease microbial drug resistance and improve clinical outcomes, the World Health Organization (WHO) has proposed the antibiotic stewardship program (ASP) [19] in an effort to try to reduce toxicity and combat antibiotic resistance, which can further ensure medical quality and decrease healthcare costs.
In China, the antibiotic use ratio in hospitalized patients is much higher than that in Europe and North America (up to 70%). Compared with internal medicine patients, the inappropriate antibiotic agent use in surgical patients is much higher [20]. Inappropriate prophylactic antibiotic use is present in up to 50% of patients, however, only 20% of patients need antibiotics. An over-dependence on antibiotic agents to prevent SSI may cause inappropriate antibiotic use that increases medical costs. Furthermore, long-term antibiotic misuse could lead to an increase in the isolation of drug-resistant bacteria, difficulty in treating infectious diseases, and the spread of multiple resistant bacteria within hospitals. Moreover, the continuous seven-year ASP intervention was implemented in a class III, grade A hospital to evaluate its effectiveness on prevention and control of SSIs during clean surgery.
Patients and Methods
Setting
Beijing Hospital, a class III, grade A hospital under the direct supervision of the National Health and Family Planning Commission, lies in the center of Beijing City. The hospital has more than 55,800 square meters of floor space, a building area of 227,788 square meters, 1,247 beds, and 38 medical and medical departments. The average annual number of discharged patients is 20,000, the average length of stay is 10 days, and the annual number of surgeries is 15,000. The number of clean surgeries from 2010 to 2016 was 5,691, 5,712, 5,292, 6,088, 6,325, 6,009, and 6,309, respectively.
Study subjects were patients undergoing clean surgeries from January 1, 2010 to December 31, 2016, in Beijing Hospital. Patients who underwent outpatient surgery and patients with infections, tumors, or who were immunocompromised during hospitalization were excluded.
Information source
Baseline information (age, gender, etc.) of the patients as well as surgical type, clinical signs, American Society of Anesthesiologists (ASA) score, operative time, prophylactic antibiotic use, and SSI are shown in Table 1. Data were obtained from the hospital information system (HIS), the hospital infection full process monitoring system, the anesthesia information system, the laboratory information system (LIS), the electronic medical record (EMR), and the nursing information system.
is t-value for independent sample t-test.
General surgery: gastrointestinal surgery, cholecystectomy, thyroid surgery, mastectomy, hernia repair (hernioplasty and herniorrhaphy) and vascular surgery. The thyroid surgery, mastectomy, hernia repair (hernioplasty and herniorrhaphy) and vascular surgery were the clean operations included in the study.
Gynecologic: myomectomy (laparoscopic procedure) and ovarian cystectomy (laparoscopic procedure).
Definitions
Surgical site infection classification criteria currently used by the U.S. Centers for Disease Control and Prevention National Healthcare Safety Network (NHSN) and Healthcare Infection Control Practices Advisory Committee (HICPAC) was used. Surveillance for SSI was conducted by the hospital infection control teams using the “Notice on Printing and Issuing the Standard for Diagnosis of Hospital infections” (Trial Implementation; 2001) [21]. Surgical site infections were defined as superficial (involving the skin and subcutaneous tissue), deep, or organ/space (when involving deep organs or cavities approached during the operation) and could occur up to 30 days, unless there was an implant in which case surveillance was continued for 1 year. However, case ascertainment was limited to the duration of the patient's hospital stay.
Intervention
We performed a quasi-experimental study to compare the effect before and after ASP intervention. During the pre-intervention stage (January 1, 2010 through December 31, 2011), comprehensive surveillance was performed to determine the SSI baseline data. In the second stage of the study (intervention stage, January 1, 2012 through December 31, 2016), an infectious diseases physician and an infection control practitioner (ICP) identified the surgical patients daily and followed up on the duration of antimicrobial prophylaxis. The effectiveness of prevention and control on SSI during clean surgery was evaluated during changes in the ASP-related indicators before and after interventions. The study was approved by the Institutional Research Ethics Committee as well as the Pharmacy and Therapeutics Committee.
Indicators of prophylactic antibiotics use during clean surgery
According to the Guideline Principles for Clinical Use of Antibiotics [22] and the Regulations for Clinical Application of Antibacterial Agents [23], five goals were implemented during the clean surgery ASP. These were: (1) that the rate of prophylactic antibiotics used during clean surgery (number of prophylactic antibiotic agents used during clean surgery/number of clean surgeries × 100%) was <30%; (2) that the drug selection qualification rate (number of antibiotic agents selected from the drug catalog of prophylactic antibiotic agents [24]/number of prophylactic antibiotics used during clean surgery × 100%) was 100%; (3) that the rate of antibiotic administered within 120 minutes of the first incision (number of the antibiotic agents administered within 120 minutes of the first incision/number of prophylactic antibiotic agents used during clean surgery × 100%) was 100%; (4) that during surgeries lasting longer than 3 hours or with blood loss volumes more than 1,500 mL, the rate of re-dosing prophylactic antibiotic agents (number of prophylactic antibiotic agents re-dosed/number of surgeries lasting more than 3 hours or that were associated with more than 1,500 mL of blood loss × 100%) was 100%; and (5) that the discontinuation rate of prophylactic antibiotic agent use by 24 hours after surgery (number of prophylactic antibiotic agents discontinued by 24 hours after surgery/number of prophylactic antibiotic agents used during clean surgery × 100%) was 100%. Additional indicators included the intensity of antibiotic consumption [25] (consumption of antibiotics/patient bed-day at the same time × 100), the pathogen detection rate (number of pathogens detected/number of patients receiving antibiotic therapy at the same time × 100%.
Process informatization
To achieve the above goals and decrease the randomness of prescribing antibiotic agents, we designed computer-assisted decision support methodology to improve the rate at which prophylactic antibiotic agents are administered appropriately, which resulted in a limited number of antibiotic prescriptions (Fig. 1).
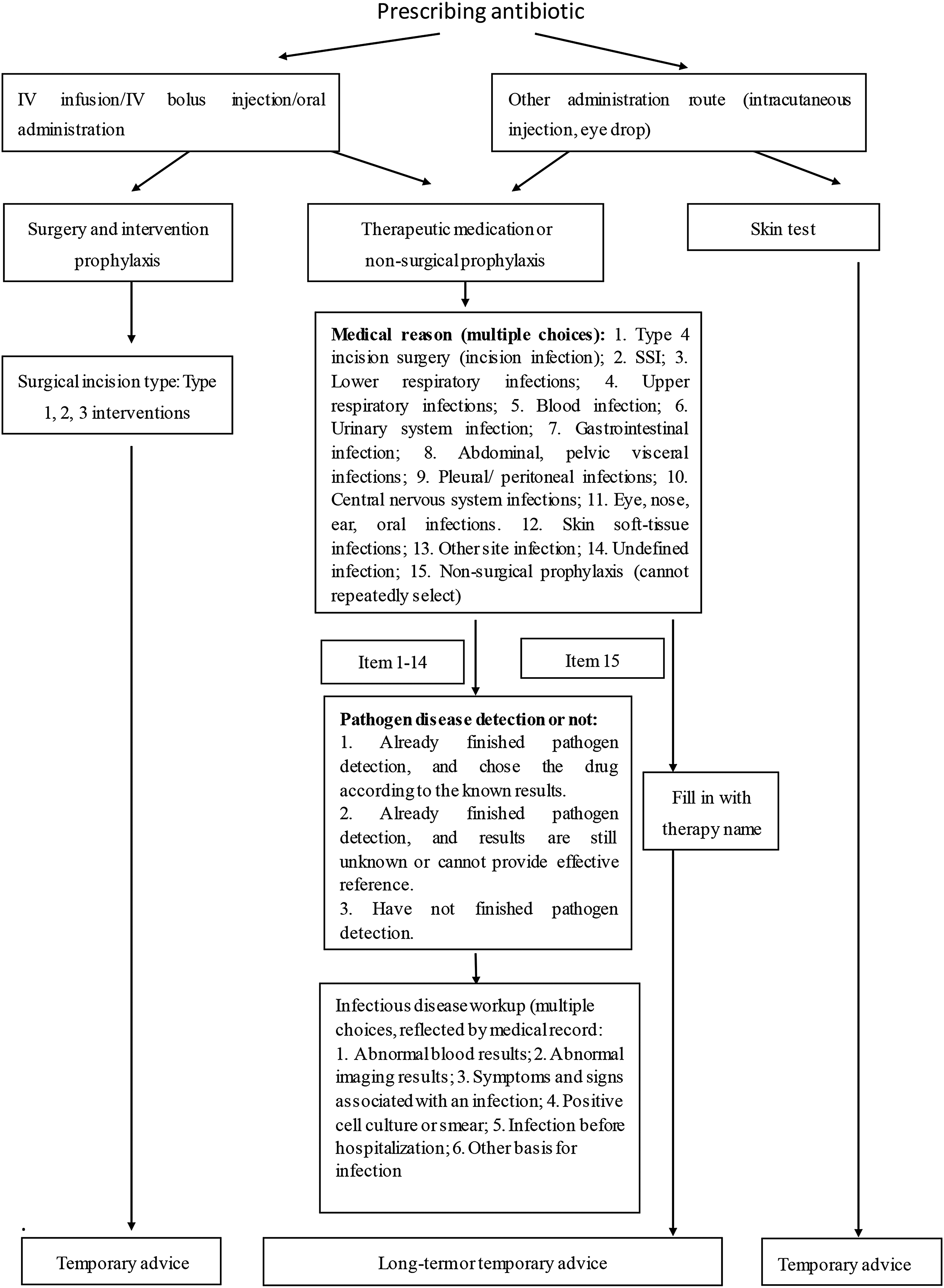
The prescription flow chart of antibiotic stewardship program. To achieve the above goals and decrease the randomness of prescribing antibiotics, we designed computer-assisted decision support methodology to improve the rate at which prophylactic antibiotics are administered appropriately, which resulted in a limited number of antibiotic prescriptions.
Training
Referring to the “Contents and Requirements” in the Guideline Principles for Clinical Use of Antibiotics [5], all of these decisions were announced to all surgeons, and regular surveillance was performed by the ICPs. Clinical staff was trained using a rational approach for administering antibiotic agents and establishing prevention and control of SSIs. Infection control practitioners were accompanied by the infectious diseases control specialists (IDCS) twice per week at the daily surgical unit visits and the surveillance results were shared with the surgeons in all surgical units. Also, monthly training seminars were given on antibiotic prophylaxis in surgical procedures.
Surveillance and feedback
Since 2012, ICPs from the hospital infection control and prevention department monitored each prophylactic antibiotic agent used during clean surgeries and clinicians were notified of any inappropriate medication given. Surgical data were monitored daily including pre-operative preparation, indicators of prophylactic antibiotic use, post-operative symptoms/signs of infectious disease, SSI condition, the need for patient re-admission within 30 days, and the need for second surgeries. The ways of surveillance results feedback in clinical practice as follows:
1. Data report: The department of nosocomial infection management summarizes the regulatory data regarding the use of antibiotic agents in the prevention of operation every month as one of the major content and provides clinical doctor with them in the form of “brief report of medical quality information.” 2. Infection control committee (ICC) meetings: In order to achieve an effective intervention, it was decided to bring about a synergy with the surgical departments and to plan the intervention in coordination with the surgeons. Thus, a series of meetings were held together with the infection ICC. The participants include the directors of every surgical unit, infection control nurses (ICNs), and IDCS. During these meetings, the following contents were discussed: (A) The indication for surgical prophylaxis, the type of antibiotic to be used, and the dose and duration of prophylaxis to be determined by the surgeon performing the surgery. (B) In order to administer the antibiotic at the correct point in time, the anesthesia technician instead of the ward nurse should be responsible for the initial prophylactic antibiotic dose. (C) Feedback the data of surveillance SAP and SSIs. 3. Trainings: ICPs were accompanied by the IDCS twice per week at the daily surgical units visits and the surveillance results were shared with the surgeons in every surgical units. The frequency of surveillance and feedback was increased in the surgical units where compliance with the guidelines was observed to be low.
Statistical analysis
The hospital infection whole process monitoring system was used to collect the data. Data were exported into EXCEL 2016 (Microsoft®, Redmond, WA) and analyzed by Statistical Package for the Social Sciences Version 24.0 software (IBM Corp., Armonk, NY); a p value <0.05 was considered statistically significant. The measurement data (such as age or operation time) that complied with a normal distribution were expressed as mean ± standard deviation (SD), and those that did not comply were expressed as median. The enumeration data (such as gender, ASA score, and SSI incidence) were expressed as percentage and ratio. Differences in monitored data (baseline information of patients before and after ASP intervention, indicators of prophylactic antibiotic use, and morbidity rate of SSI) were analyzed by t-test and χ2 test.
Results
Baseline characteristics
A total of 41,426 patients were enrolled in a class III, grade A hospital from January 1, 2010 to December 31, 2016. The average age was 58.8 ± 13.2, and the ratio of patients older than 65 was 41.8%. There were 16,405 males, which accounted for 39.6% of the patients. The ratios of the ASA scores in grade I–II accounted for 87.4%. There were 41,053 selective operations, and the first three clean surgical procedure were ophthalmic (14,292; 34.5%), plastic (10,895; 26.3%) and general surgery (10,357; 25.0%). The above baseline data had no statistical significance before and after ASP intervention (p > 0.05; Table 1).
Surgical site infection data and antimicrobial agents used in surgeries
During the study period (January 1, 2010 to December 31, 2016), the prophylactic antibiotic use rate in the 41,426 clean surgeries was reduced from 82.9% before intervention to 28.0% after intervention. The medication rate 0.5–2 hours before the first skin incision increased from 20.8% to 85.1%. The drug withdrawal rate 24 hours after surgery increased from 22.1% to 60.4%. The appropriate antibiotic use rate increased from 37.0% to 93.6%. Re-dosing of prophylactic antibiotic agents increased from 3.8% to 64.8%. The SSI rate during clean surgery reduced from 0.7% to 0.5% (Table 2, Fig. 2). All of these indicators reached statistical significance before and after ASP intervention (p < 0.05).
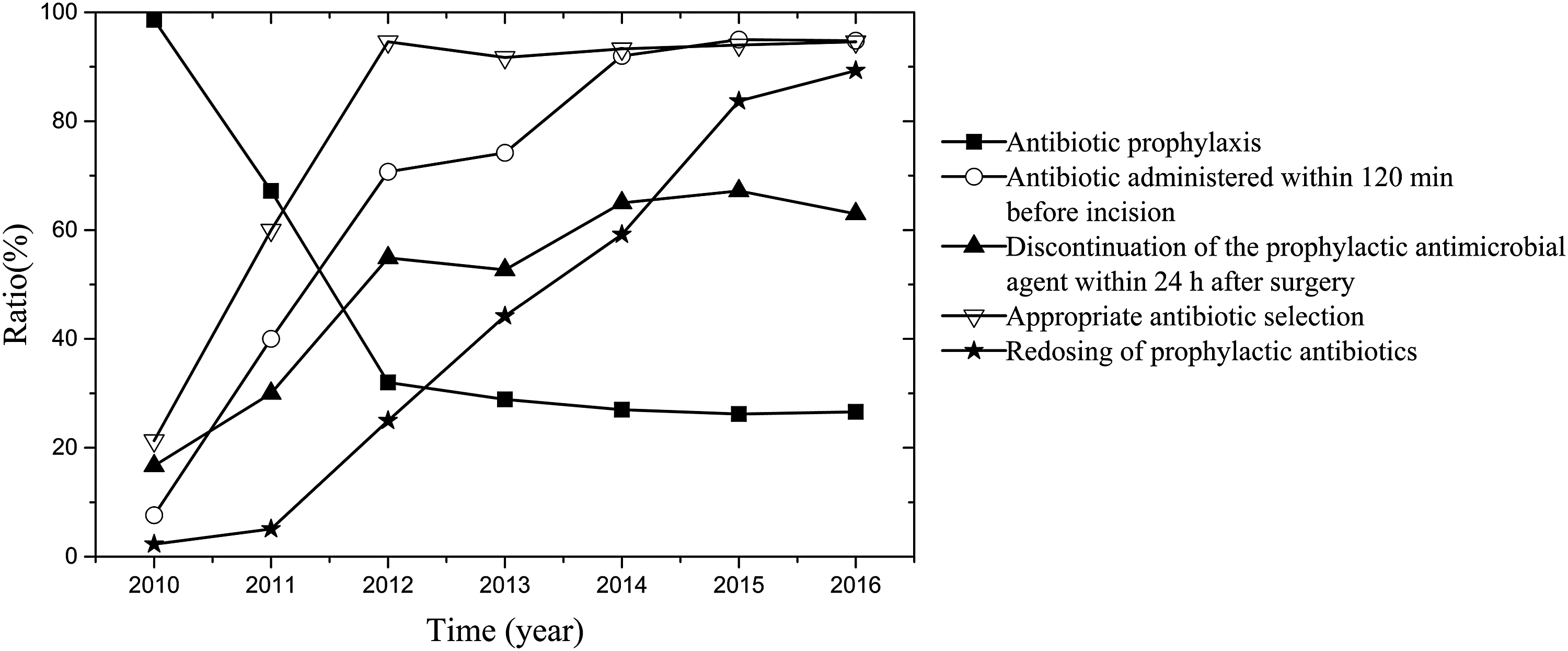
The trends of antibiotic prophylaxis indicators from the years 2010–2016. During the study period (January 1, 2010 to December 31, 2016), the prophylactic antibiotic use rate in the 41,426 clean surgeries was reduced from 82.9% before intervention to 28.0% after intervention. The medication rate 0.5–2 hours before the first skin incision increased from 20.8% to 85.1%. The drug withdrawal rate 24 hours after surgery increased from 22.1% to 60.4%. The appropriate antibiotic use rate increased from 37.0% to 93.6%. Re-dosing of prophylactic antibiotics increased from 3.8% to 64.8%. The surgical site infection (SSI) rate during clean surgery decreased from 0.7% to 0.5%.
The denominator is number of prophylactic antibiotics used.
The denominator is the number of surgeries lasting longer than 3 h or with greater than 1,500 mL of blood loss.
SSIs = surgical site infections.
Pathogen detection rates and the intensity of antibiotic use
During the study period, the pathogen detection rate increased from 16.7% before ASP intervention (January 1, 2010 to December 31, 2011) to 41.8% after ASP intervention (January 1, 2012 to December 31, 2016). The intensity of antibiotic consumption was analyzed through the quantitative calculation of the defined daily dose (DDD) for every 100 procedures. The intensity of antibiotic consumption decreased from 74.9 DDDs per 100 bed-days before ASP intervention to 35.2 DDDs per 100 bed-days after ASP intervention.
Discussion
Through this seven-year study and the continuous five-year ASP, the indicators of prophylactic antibiotics used during clean surgery (rate of prophylactic antibiotic use, the rate of antibiotic administered during within 120 minutes of the first incision, the discontinuation rate of prophylactic antibiotics by 24 hours after surgery, appropriate antibiotic selection rates, and rate of re-dosing prophylactic antibiotics) have been explained. Moreover, the SSI incidence during clean surgery did not increase during the study period but was well controlled. Other indicators that indicated appropriate antibiotic use (such as a reduced pathogen detection rate, and decreased intensity of antibiotic use) were greatly improved after ASP intervention. Thus, a long-term and continuous antibiotic stewardship program has substantial effects on the prevention and control of SSI during clean surgery.
Antibiotic stewardship program and prophylactic antibiotics use
Overuse or inappropriate antibiotic use not only increases bacterial resistance and makes treatment more difficult, but also severely threatens medical quality and safety [25]. With the increase in and variety of multi-drug–resistant organisms, such as methicillin-resistant Staphylococcus aureus (MRSA) and carbapenem-resistant Enterobacteriaceae (CRE), the WHO proposed ASP and then completed the WHO Global Strategy for Containment of Antimicrobial Resistance in 2001 [15]. In 2013, the U.S. Centers for Disease Control and Prevention (CDC) released a publication, Antibiotic Resistance Threats in the United States, 2013. In this publication, the CDC discusses the dangers of bacterial resistance in relation to antibiotic overuse in the United States and proposes solutions to tackle these problems [26]. China has already taken action to manage antimicrobial overuse and issued the Guidelines for Clinical Use of Antimicrobials in 2004 and 2015 and the Regulations on Clinical Applications of Antimicrobials in 2012. The aims of these guidelines are to promote appropriate antibiotic use in clinics and to control the antimicrobial resistance.
The ASP includes seven core measures [27]: a leadership commitment; accountability; pharmacist; action; tracking; reporting; and education. These core principles that were acquired by information-based systems limited the availability of antibiotic prescriptions, and standardized antibiotic therapy during clean surgeries through improvements in doctor and clinical staff training.
Standardization of peri-operative antibiotic administration is essential in the ASP. Excessive dependence on antibiotics to prevent SSI not only ignores the importance of the ASP core measures for SSI prevention and control but also results in the inappropriate use of peri-operative antibiotics. Antibiotic overdose, a prolonged course of antibiotic treatment, and the inappropriate use of antibiotics cannot prevent SSI, but they do increase the risk of bacterial resistance [28]. Ou et al. [29] reported that prophylactic drug rates in the peri-operative period of surgery were as much as 98.2%, but only 17.4% of surgical patients needed prophylactic antibiotics. In France [30], The Netherlands [31], and Turkey [32], the prophylactic drug rates were 41.7%, 28% and 34.3%, respectively. These results show that after using ASP, the rate of prophylactic antibiotics was decreased from 76.1% to 26.8%. Other indicators, such as the rate of antibiotic administered within 120 minutes of the first incision, the discontinuation rate of prophylactic antibiotics by 24 hours after surgery, appropriate antibiotic selection rate, and rate of prophylactic antibiotic re-dosing also tended to be rational.
Antibiotic stewardship program and SSI
Although antibiotic prophylaxis plays an important role in reducing the rate of SSIs, other factors such as attention to basic infection-control strategies [33], the surgeon's experience and technique, the duration of the procedure, hospital and operating room environments, instrument sterilization issues, preoperative preparation (e.g., surgical scrub, skin antisepsis, appropriate hair removal), peri-operative management (temperature and glycemic control) and the underlying medical condition of the patient may have a strong impact on SSI rates [34,35]. Patient-related factors associated with an increased risk of SSI include extremes of age, nutritional status, obesity, diabetes mellitus, tobacco use, coexistent remote body-site infections, altered immune response, corticosteroid therapy, recent surgical procedure, length of pre-operative hospitalization, and colonization with micro-organisms. Antimicrobial prophylaxis may be justified for any procedure if the patient has an underlying medical condition associated with a high risk of SSI or if the patient is immunocompromised (e.g., malnourished, neutropenic, receiving immunosuppressive agents) [36]. After implementing ASP, limiting drug selection and decreasing the rate of prophylactic antibiotic use, could the incidence of SSIs increase? It was reported that misuse of antibiotics does not enhance the effectiveness of antibiotics in preventing SSIs, but it can increase bacterial resistance [13]. Our results indicate that appropriate selection of antibiotics, good timing of medication administration, proper supplementary antibiotics, and an increased pathogen detection rate can enhance the antibacterial effect, and thus reduce the use of unnecessary antibiotics. And it can further prevent SSI and reduce bacterial resistance. The Guideline for the Prevention of Surgical Site Infection [37] and the Preoperative Measures for Surgical Site Infection Prevention [38] have proved that ASP is effective in the prevention of SSIs.
Antibiotic stewardship program and pathogen detection rate
In order to improve the pathogen detection rate, our hospital carried out major interventions as follow: (1) the pathogen detection rate before the use of antibiotic agents is included in the performance assessment of clinical departments. If the pathogen detection rate has not reached the designated goal, the income of clinical doctors will be influenced; (2) the study designed The Prescription Flow Chart of Antibiotic Stewardship Program (refer to Fig. 1 for details) to require surgeons to check whether pathogen specimens are kept before the use of antibiotic agents, which improves the pathogen detection rate as well as the consciousness of pathogen detection of surgeons before the use of antibiotic agents.
Advantages and limitations
The continuous seven-year investigation and five-year ASP promoted appropriate antibiotic use and prevented SSIs. Forty thousand clean surgeries were monitored prospectively for seven years uninterrupted, yielding a large sample size with good representation. Through informatization methods, ASP was implemented effectively and the feasibility and effectiveness of these methods were proven.
However, we did not evaluate the effectiveness of ASP on bacterial resistance or on health economics-related indicators. Thus, in the future, we will perform comprehensive and objective studies looking at the effects of ASP on these indicators. Also, results from single-center studies are limited, so that in the future studies, multi-center studies may be carried out to test the feasibility and effectiveness of ASP on SSI prevention.
Conclusion
Long-term, continuous, and persistent ASP promotes appropriate antibiotics use and has significant effects on the prevention and control of SSI during clean surgery. These successful experiences will be disseminated into medical institutions in specific area of China.
Footnotes
Acknowledgments
We thank all healthcare professionals in hospitals involved in the study.
This publication was supported by the Cooperative Agreement Number BJ-2016-042 from Beijing Hospital Nova Project.
Author Disclosure Statement
No competing financial interests exist.