
Abstract
Abstract
Background:
Video education has many advantages over traditional education including efficiency, convenience, and individualized learning. Learning sterile surgical technique (SST) is imperative for medical students, because proper technique helps prevent surgical site infections (SSIs). We hypothesize that video education is at least as effective as traditional skill demonstration in teaching first-year medical students SST.
Methods:
A video series was created to demonstrate SST (https://www.youtube.com/playlist?list=PLcRU-gvOmxE2mwMWkowouBkxGXkLZ8Uis). A randomized controlled trial was designed to assess which education method best teaches SST: video education or skill demonstration. First-year medical students (n = 129) were consented and randomly assigned into two groups: those who attended a skill demonstration (control group; n = 70) and those who watched the video series (experimental group; n = 59). The control group attended a pre-existing 90-minute nurse educator-led skill demonstration. Participants then completed a 30-item multiple choice quiz to test their knowledge. Each group then received the alternate education method and completed a 23-item follow-up survey to determine their preferred method.
Results:
Seven 2- to 6-minute videos (30 minutes total) were created on surgical attire, scrubbing, gowning and gloving, and maintaining sterility. The experimental group (n = 51) scored higher on the quiz compared with the control group (n = 63) (88% ± 1% versus 72% ± 1%; p < 0.0001). Students preferred the videos when it came to convenience, accessibility, efficiency, and review, and preferred the skill demonstration when it came to knowledge retention, preparedness, and ease of completion.
Conclusions:
Video education is superior to traditional skill demonstration in providing medical students with knowledge of SST. Students identified strengths to each method of teaching. Video education can augment medical students' knowledge prior to their operating room experience to ensure that a sterile environment is maintained for patients. The ultimate goal is to reduce SSIs.
V
Video education is successful in teaching medical skills because it has numerous advantages. Videos are accessible and efficient; they allow the viewer to learn at their own pace, provide superior visualization of the topic being studied, and cognitively pre-train the mind for real-life experience [3,7,8]. Perhaps the greatest advantage of using videos to learn is convenience. Videos can be accessed via desktop, laptop, or mobile, and they can be paused, fast-forwarded, and replayed infinitely. The convenience of videos as an educational tool has become exceedingly important in era of duty-hour restrictions, where clerks and residents spend less time in the hospital. This could be why medical students and residents are actively seeking out medical education videos. Glass et al. [9] found that 41.6% of senior residents and 24.5% of junior residents from the Resident and Associate Society of the American College of Surgeons used online videos and lectures. Similarly, Barry et al. [10] surveyed medical and radiation therapy students and found that 50% watched videos to help them with anatomy lessons at least once per week. Many of these advantages associated with video education make it a more appealing option than traditional skill demonstration.
Videos on sterile surgical technique (SST), the processes used during invasive medical procedures to reduce the spread of micro-organisms, appear to be particularly popular; a YouTube (San Bruno, CA) search of the topic returns approximately 31,300 results [11]. This popularity may be because learning proper SST is imperative for many different groups of medical professionals. Practically, proper technique is required to participate in surgical procedures inside the operating room and to perform other sterile procedures outside of the operating room, such as suturing and catheterization. More importantly, it is crucial to learn these skills correctly because improper technique can cause surgical site infections (SSIs) that have severe consequences for patient health and can result in increased healthcare costs. For example, Merkow et al. [12] found that SSIs are the leading cause of unplanned readmission following surgery and Kirkland et al. [13] found that SSIs increase length of hospitalization, need for intensive care unit admission, and mortality. SSIs also burden the healthcare system by creating the need for additional resources, which increases the cost of hospitalization for infected patients [13]. Therefore, it is important to ensure that healthcare students are trained properly to perform SST. Videos are a promising method with which to accomplish this task.
The purpose of this study was to compare the effectiveness of video education and traditional skill demonstration in teaching first-year medical students SST, and to determine which method students preferred to use. We hypothesize that video education is at least as effective as traditional skill demonstration in teaching first-year medical students SST.
Methods
Video production
A video series was created to educate medical students on SST. (The videos may be accessed on YouTube at https://www.youtube.com/playlist?list=PLcRU-gvOmxE2mwMWkowouBkxGXkLZ8Uis) The topics were chosen by a surgeon and medical student. The content was based on the University of Alberta Hospital's mandatory skill demonstration session to reflect what a medical student would be expected to know and do when participating in the operating room. Scripts were written for each topic before filming to ensure that all necessary information was included in the videos and was organized in a clear, logical manner. The scripts were written to ensure the type, amount, and presentation of information was suitable for the target audience. To ensure accuracy of the information, a surgeon and surgical nurse educator edited the scripts before they were filmed, and oversaw the filming.
Although there are already many videos teaching SST in existence, we decided to create new videos to ensure that we made a series that was comprehensive, patient-focused, and easy to follow. For example, while many existing videos only cover a certain portion of SST, such as scrubbing or gowning and gloving, we made a series that covered every process from start to finish. We also noticed that although many videos described the processes of SST well, they failed to relate the importance of proper technique to patient health and safety. We chose to highlight this importance so viewers would think about the reason behind proper technique when learning about and performing SST. We also tried to make the videos easy to follow by using a narrator, actor, written headings, and easy stepwise process to aid learners in knowledge retention.
The videos were filmed from August 2–5, 2016 in the University of Alberta Hospital Operating Suite to introduce students to the operating room and demonstrate SST in a realistic environment. The videos featured a narrator who explained key concepts and an actor who demonstrated techniques. Once the videos were completed, they were edited to include written headings, summaries, and Web page links.
Participants
To assess the effectiveness of these videos, a randomized controlled trial was designed. The study protocol received approval from the University of Alberta Research Ethics Board (Pro00000067022) in August 2016. In September 2016, first-year medical students were recruited from the University of Alberta for this study. First-year medical students were chosen for this study because surgical sterility is part of the medical education curriculum. Furthermore, first-year students were the least likely to have had prior experience with SST. Recruitment took place at various optional and mandatory student events and via the classes' social media page and e-mail. This ensured that the whole class, and not just those interested in surgery, knew about the study. The only inclusion criteria was being a first-year medical student at the University of Alberta. Individuals were excluded if they were not first-year medical students.
Consent and randomization
Participants were given a consent form to sign prior to starting the study. The consent form explained the purpose and the flow of the study. Participants were requested to provide their e-mail address for further communications. The consented participants were randomly assigned into two groups: those who attended a skill demonstration session first (control group) and those who watched the video series first (experimental group). Randomization was performed using computer-generated random numbers. Participants who were randomly assigned an odd number joined the control group and participants who were randomly assigned an even number joined the experimental group.
Education method
After consent and randomization, the control group attended a skill demonstration and the experimental group watched the video series. Dates for the skill demonstration were organized between September 2016 and January 2017, and control participants were free to sign up for whichever session suited their schedule. The skill demonstrations that the participants attended were the pre-existing University of Alberta Hospital sessions that are mandatory for all students who intend to participate in the operating room. Students attended the 1.5-hour long session in groups of six or fewer. The sessions were led by a surgical nurse educator. During the skill demonstration, students toured the operating room to learn about the operating room environment, surgical attire, water-based and waterless scrubbing, gowning and gloving, maintaining sterility in the operating room, handling simple surgical tools, and sharps safety. The nurse educator explained and demonstrated proper technique, and then students practiced the techniques under her supervision.
For the experimental group, an e-mail containing a link for the video series was sent in October 2016. The participants were free to watch the videos at their leisure and as many times as they wanted. The videos were hosted on a private YouTube page that only those with the link could access. Experimental participants were asked not to share the link with anyone to minimize the opportunity for the control group to access the videos.
Quiz
After each student completed their randomly assigned educational format, they were instructed to take an online 30-item multiple-choice quiz on SST. Control participants received a link to the quiz from the nurse educator and experimental participants accessed the quiz through a link on YouTube. Participants were asked to complete the quiz as soon as possible and received up to a total of three e-mail reminders to do so.
The quiz was created to test knowledge that first-year medical students are expected to have prior to participating in the operating room. It included 10 questions on scrubbing, 10 questions on gowning and gloving, and 10 questions on maintaining sterility in the operating room. A medical student, surgeons, and the nurse educator wrote and edited the questions. In addition to these questions, students were asked to report their age, gender, level of interest in surgery, and prior knowledge of SST. They were also asked to confirm whether or not they had completed the skill demonstration and watched the videos to ensure that they complied with their assigned educational format prior to writing the quiz.
Alternate education method and follow-up survey
After completing the quiz, participants received the alternate educational format. The control group was e-mailed a link to the videos, while the experimental group was e-mailed a sign-up link to choose a date for their skill demonstration.
After each participant had completed the alternate educational format, they were requested to complete a 23-item follow-up survey created to determine which educational format they preferred. The control participants accessed the survey through a link on YouTube and experimental participants were e-mailed the link. The survey consisted of four sections: general feedback, video feedback, skill demonstration feedback, and additional comments. The questions in each section were presented as either forced response or long answer (Supplementary Table S1 [see online supplementary material at http://www.liebertpub.com/sur]).
Analysis
Participants' age, gender, prior knowledge of SST, and level of interest in surgery were analyzed using the Mann-Whitney U test, Fisher exact test, and χ2 test to determine whether or not there was a significant difference in these parameters between the control and experimental groups.
Average quiz scores were calculated, and an unpaired t-test with Welch correction was performed to determine significance between the groups. Spearman ρ correlation was used to determine whether there was a relation between quiz scores and prior knowledge of SST or interest in surgery.
Quiz questions that were answered correctly less than 50% of the time were reported. Fisher exact test was used to determine if there was a difference in the number of correct answers to these questions between the control and experimental groups. Spearman ρ correlation was used to determine if there was a relation between both the quiz and follow-up survey for the groups. Significance was considered at p < 0.05.
Results
Video production
Seven 2- to 6-minute videos were created: (1) Surgical Dress (2:26 minutes), (2) Water-Based Scrub (4:31 minutes), (3) Waterless Scrub (4:09 minutes), (4) Common Errors (4:13 minutes), (5) Gowning and Gloving with Assistance (5:42 minutes), (6) Self -Gowning and Gloving (3:45 minutes), and (7) Maintaining Sterility (5:56 minutes; Fig. 1). The series was approximately 30 minutes in total.
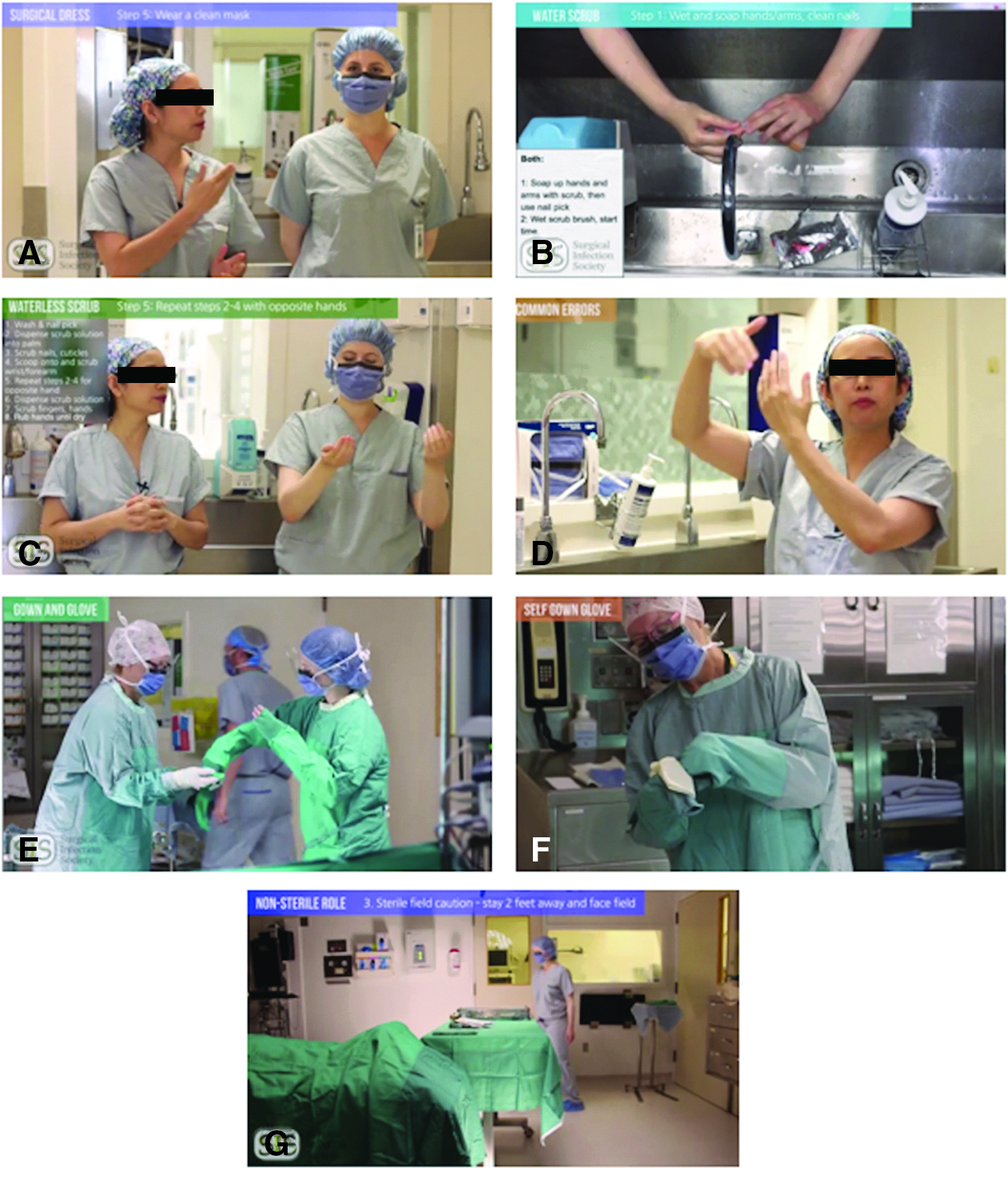
Surgical education video series. (
The video on surgical dress showed viewers the necessary surgical gear that must be donned and in which situations it must be worn. It also explained how each piece is important in preventing the spread of infection from the healthcare providers to the patients, and vice versa. In the videos on waterless and water-based scrubbing, the process was described in a step-by-step fashion while an actor demonstrated. The video on common errors was designed to make students aware of common breaches of sterility and teach them how to resolve those situations. Examples of the errors discussed included contaminating oneself during the scrub process and forgetting to wear a mask in the operating room. Two videos were created on gowning and gloving to teach students how to complete the process with the assistance of a scrub nurse and alone. The video on maintaining sterility showed viewers how to remain sterile as a sterile member of the team and as a non-sterile member of the team.
Each of the processes described in the videos were broken down into simple steps that were narrated and demonstrated in the operating room. To provide an additional learning modality, headings and summaries were used on-screen to help the viewer follow along and remember the steps.
Participants
One hundred twenty-nine students consented to participate in the study; this was 80% of the first-year class (Fig. 2). Seventy of these participants were randomly assigned to the control group and 59 to the experimental group. Of these, 64 control and 51 experimental participants completed the quiz, and 49 control and 48 experimental participants completed the follow-up survey. One control participant wrote the quiz after completing both education methods, so their data were excluded from the analysis.

Study flow and participation. One hundred twenty-nine participants were consented; 70 were randomly assigned to the control group and 59 were randomly assigned to the experimental group. Sixty-four control participants completed the quiz and 49 completed the follow-up survey. Fifty-one experimental participants completed the quiz and 48 completed the follow-up survey. *One participant completed the quiz after receiving both education methods, so their data were removed from the analysis.
The average age was 23.3 for control and 22.5 for experimental groups (Table 1). The control group comprised 57% females and the experimental group comprised 69% females. The percentage of students who reported prior knowledge of SST was 19% in the control group and 27% in the experimental group. In the control group, 8% were not interested in surgery, 67% were somewhat interested, and 25% were extremely interested. In the experimental group, 4% were not interested in surgery, 65% were somewhat interested, and 31% were extremely interested. There was no significant difference in any of these parameters between the control and experimental groups.
Mann-Whitney U test.
Fisher exact test.
χ2 test.
These variables were self-reported by participants who completed the quiz. p values were calculated to determine whether or not there was a significant difference in these variables between the control and experimental group.
SD = standard deviation
Quiz
There was a difference between the control (n = 63) and experimental (n = 51) group's averaged quiz results, with lower scores in the control group (72% ± 1% vs. 88% ± 1%; p < 0.0001; Fig. 3). The scores ranged from 16 to 29 in the control group and 15 to 30 in the experimental group (Fig. 4). There were 3 participants in the control group and 31 participants in the experimental group who scored 90% or higher. None of the participants in the control group achieved a perfect score, however 4 participants in the experimental group did achieve a perfect score.
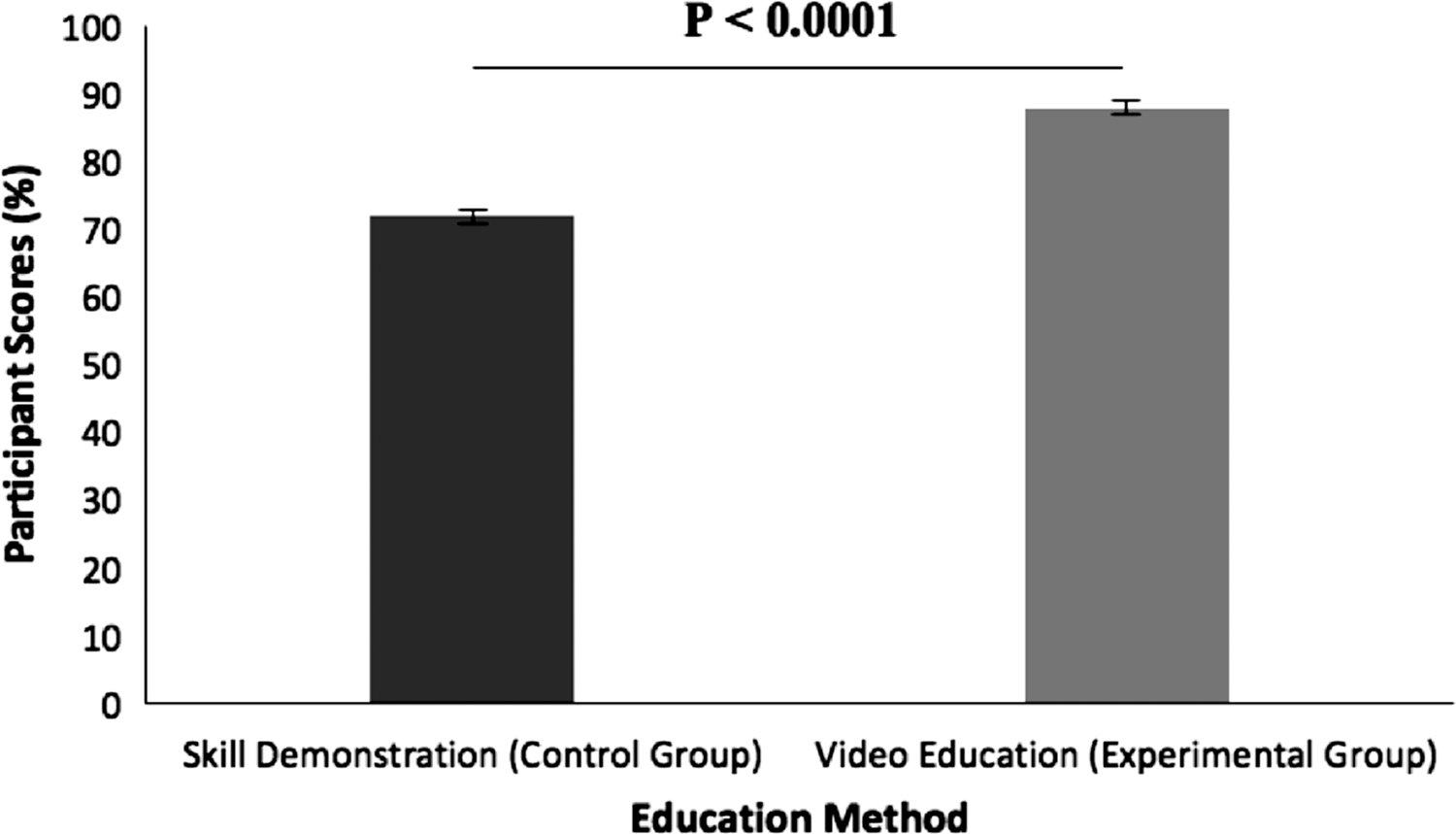
Statistical comparison of control (n = 63) and experimental (n = 51) group quiz score percentages. The average score percentage was 72% ± 1% for the control and 88% ± 1% for the experimental group. There was a significant difference between the groups (p < 0.0001).
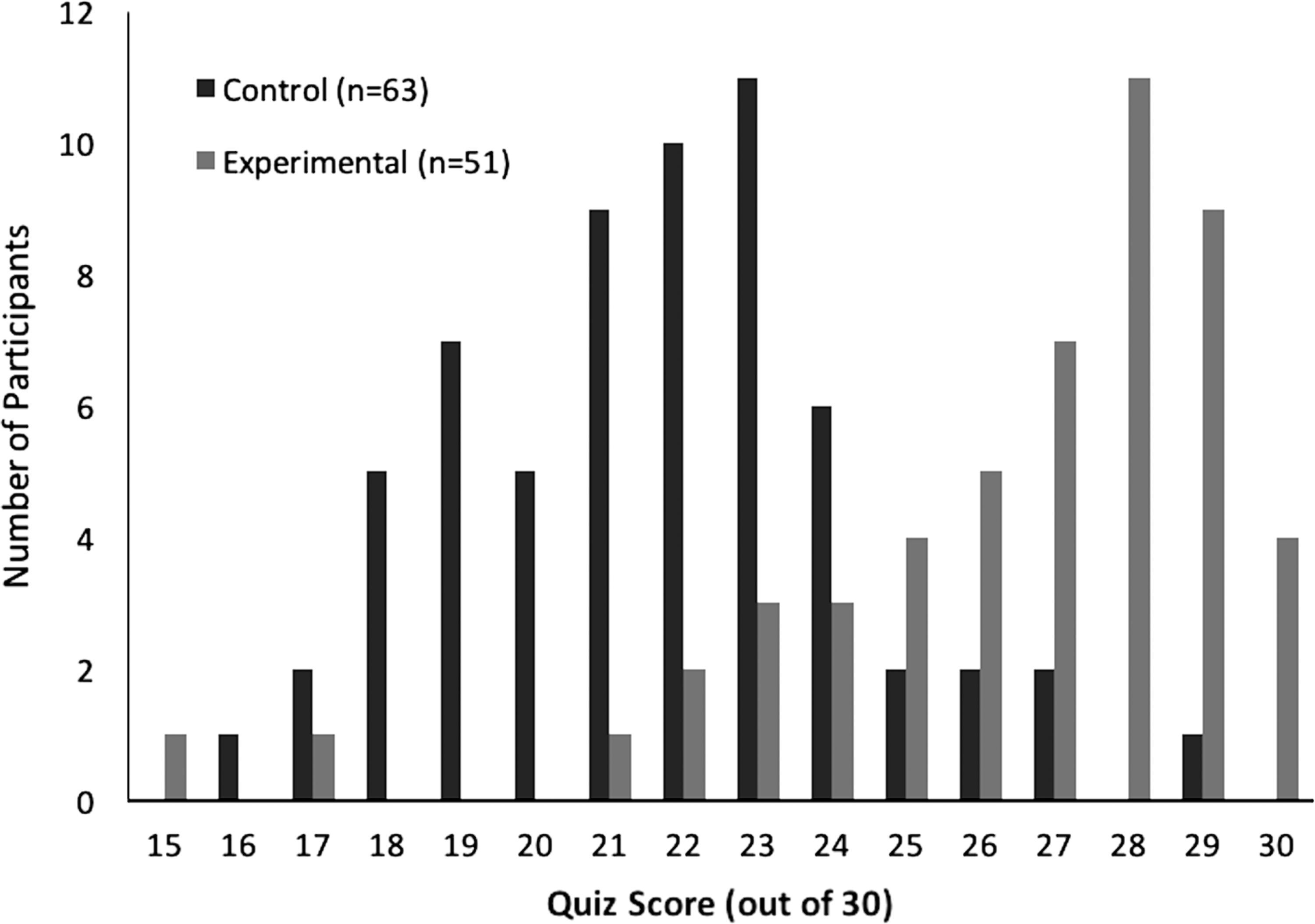
Individual control (n = 63) and experimental (n = 51) group quiz scores. Scores ranged from 16 to 29 in the control group and from 15 to 30 in the experimental group.
Four questions were answered correctly by less than 50% of participants. These questions tested knowledge on: the sterile portions of a surgical gown; gowning and gloving protocol; sterile field limits; and mask usage. The scores for the control and experimental groups were as follows: 18 correct versus 31; 12 correct versus 42; 12 correct versus 52; and 24 correct versus 29, respectively.
A post hoc power analysis with a significance of p < 0.05 and difference in the test score between the 2 groups (72 ± 1% [control, n = 63] and 88 ± 1% [experimental, n = 51]) was scored resulting in a power analysis of 100%.
Follow-up survey
The video series was the top choice when the students were asked which method was the most convenient (82%), accessible (94%), efficient (75%), and which they would use to review SST (80%; Fig. 5). The skill demonstration was the top choice when students were asked which method was easier to complete (40%), helped them retain the most knowledge (64%), and made them feel more prepared to scrub in (51%). The majority of participants (97%) thought that the videos supplemented the skill demonstration.
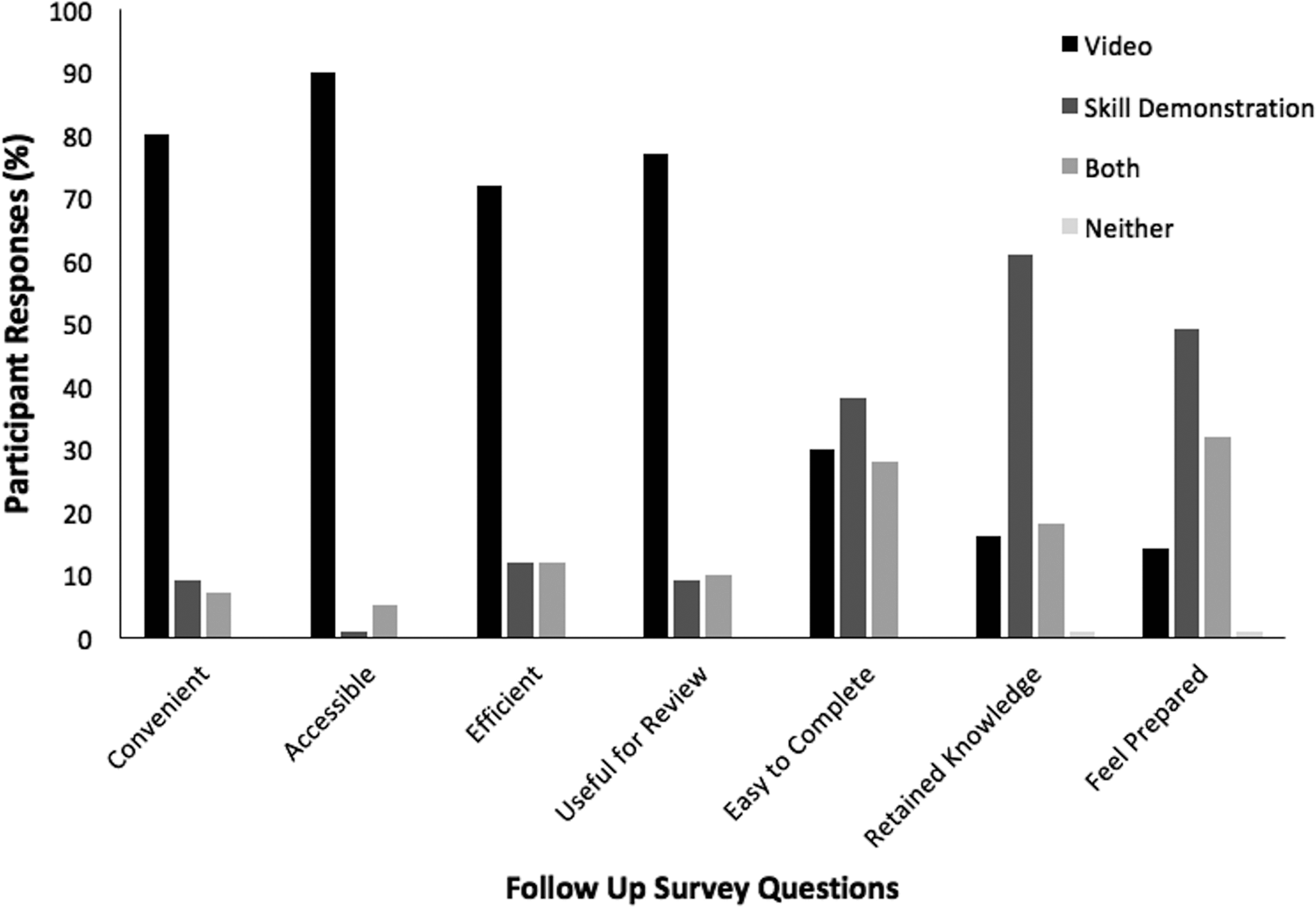
Participant responses to follow-up survey (n = 96). Participants were asked to select which education method (video, skill demonstration, both, or neither) was the best in regards to convenience, accessibility, efficiency, usefulness in reviewing the material, easiness to complete, knowledge retention, and preparation. Video was the top choice for convenience (82%), accessibility (94%), efficiency (75%), and usefulness for review (80%). Skill demonstration was the top choice for easiness to complete (40%), knowledge retention (64%), and preparation (51%).
When asked if they watched the videos after the study, 28% of participants said they watched the videos at least once more. The most common reason listed for not re-watching the videos was because students had not had an operating room experience yet and thus had not needed to use the videos (n = 37). Fifteen students said they would watch the videos in the future. When participants were asked what they liked about the videos, the top response was that they could learn at their own pace by doing things like pausing, re-winding, and re-watching the videos (n = 36). For example, one student said, “I could go through the videos at my own pace and even go backwards if I missed or didn't understand something.” The top dislike was that students did not get to physically practice the techniques while watching the videos (n = 33). When asked which video they liked the most, the top answer was “all” (n = 19), followed by the scrubbing videos (n = 24; 16 did not specify which scrubbing video so responses were combined). When asked to suggest improvements, the most common response was “nothing” (n = 35), followed by adding a video to the series that oriented students to the operating room and reviewed the roles of operating room team members and how to identify them (tied, n = 5).
When asked if participants went back to see the nurse educator for a skill demonstration after the study, 1% said yes. The most common reason given for not returning to see the nurse educator was that students had not scrubbed in yet and so had not needed to (n = 33). Others said that they had not “had a reason for taking up her time” and that they didn't “want to bother [her].” Four students said they would see her in the future. When participants were asked what they liked about the skill demonstration, the most common answer was that the session was hands-on and allowed them to practice the techniques (n = 56). When asked about what they disliked, the most common answer was that the session was too long (n = 24). For example, one student said that the session “was long so I forgot some stuff by the end.” The most-liked part of the skill demonstration was the section on scrubbing (n = 30; 28 did not specify which scrubbing video so responses were combined). The top suggestion for improving the session was “nothing” (n = 40), followed by including handouts or resources for students to help them remember and review what they had learned (n = 8).
When students were asked if they had any additional comments to share, the most common answer was “no” (n = 65), followed by the opinion that using the videos and skill demonstration together was a valuable learning experience (n = 13). For example, one student said, “I watched the video three times before coming in for the in-person scrubbing, so as the nurse was showing the steps to us, I already knew what they were—allowing me to pay full attention to doing it right, and having that real practice solidified my knowledge.”
Quiz score and correlations
A Spearman ρ correlation analysis showed that there was no significant correlation between quiz scores and prior knowledge of SST or interest in surgery (Table 2). However, there was a relation in the control group for those who were interested in surgery and had prior knowledge of sterile surgical technique (0.36, p = 0.002). Using Spearman ρ correlation coefficients, it was determined that there was no relation between participants' quiz scores and how they perceived the convenience, accessibility, efficiency, ease, knowledge retention, and preparedness of the two educational formats (Table 3).
Spearman ρ correlation analysis revealed that there was no effect of prior knowledge and interest in surgery upon the participant's quiz score.
Spearman ρ correlation analysis revealed that students' opinions about each method's convenience, accessibility, efficiency, ease of completion, knowledge retention, and preparation had no effect on their quiz performance. Correlation coefficient value present.
Upon noting that four questions in the quiz were answered incorrectly more than 50% of the time, a Fisher exact test was used to determine if the video educational format had an effect on reducing errors in these questions. For each question, more experimental than control participants answered correctly. This was significant for two of the four questions (Table 4). Spearman ρ correlations showed a significant correlation between quiz score in the experimental group and all four questions (Table 5). There was a correlation between quiz score in the control group and one of these questions.
Correlation is significant at the 0.0001 level.
There were four questions on the quiz that were answered incorrectly by more than 50% of participants. The relation between these questions and the educational format was assessed. There were a higher number of correct answers in the experimental group for each question. Fisher's exact test revealed that the number of correct responses was significantly different (p < 0.0001) between the control and experimental groups for two questions, one asking about the sterile areas of a gown and one asking about the sterile field in the operating room.
Correlation is significant at the 0.01 level (2-tailed).
Correlation is significant at the 0.05 level (2-tailed).
A Spearman ρ correlation was done to assess the correlations in both the control and experimental groups. There was a significant relation in the experimental group between quiz score and answering the questions correctly. Significance was only observed in one of the questions in the control group. Correlation coefficient values present.
Discussion
It is important that medical students learn how to perform SST for many reasons. Primarily, proper technique is necessary to prevent SSIs, which have dire consequences for patient health. Surgical site infections increase cost, number of unplanned re-admissions, length of hospitalization, need for intensive care, and mortality [12,13]. On a practical level, learning SST is a requirement of the medical profession, regardless of specialty. From an education standpoint, mastery of SST can lead to a better surgical experience for medical students, because surgeons are more likely to allow students to participate in procedures if they can demonstrate competence in these techniques [14]. Poor understanding and improper use of SST can lead to negative student experiences during surgical rotations, which can influence students' future career choices. For instance, Goldacre et al. [15] showed that 44.9% of U.K. medical graduates felt that medical school experiences greatly influenced their career choice. However, learning SST can be difficult for medical students, who often find the operating room to be an intimidating place; this is why both students and surgeons agree on the importance of having an orientation prior to surgical experience [14,16]. The present video series was created to meet this need and help reduce the above mentioned consequences of improper SST.
The seven-part video series was used to orient and educate medical students on performing and maintaining surgical sterility. A randomized controlled study was designed to compare the videos with the gold standard skill demonstration to determine which method was better at teaching SST and which method was preferred by the students. The present study recruited 80% of the first-year medical student class, thereby obtaining a representative sample size. The study design also allowed for direct comparison of the educational methods in learning multiple aspects of SST.
Video education was more effective at teaching sterile surgical technique
Quiz scores demonstrated that the videos were more effective at teaching first-year medical students SST. Because the experimental group only watched the videos before completing the quiz, their scores represented the effectiveness of the video series in teaching SST. The fact that there was no difference in prior knowledge or interest in surgery between the groups supports that the videos and not these factors were responsible for the higher quiz scores. The quiz questions were chosen to reflect what a first-year medical student should know when participating in the operating room, therefore the difference in scores suggests that the videos were better at highlighting essential elements of SST than the skill demonstration. The experimental group also outperformed the control when it came to answering the most difficult questions on the quiz. Of the four questions with less than 50% correct responses, the experimental group scored higher than the control group each time. This suggests that the students in the experimental group remembered more details than in the control group. Analysis also showed that the experimental participants' quiz scores were correlated to their answers to these four questions. This illustrates that video education does have an effect on quiz performance. The demonstrated superiority of video as an educational method over traditional education was also observed by Shippey et al. [2] who likewise found that video education was better than skill demonstration at helping medical students retain knowledge about sub-cuticular suturing after one week. Others who compared the two education methods in teaching surgery-related topics suggested that the methods were equally effective [4,17] or worked best when both methods were combined together [5,17,18].
There are many possible reasons why the videos may have outperformed the skill demonstration in the present study. Videos have many inherent advantages over traditional skill demonstration, including accessibility, convenience, efficiency, and self-paced learning [3,7,8]. The accessibility and convenience of the videos make them a more attractive option. The fact that students can learn from the videos at any time and location encourages its use. The efficiency of videos allows viewers to learn a large amount of information in a short period of time, which is important to students and higher level surgical trainees who are expected to achieve competency in the face of decreased work hours [7]. The self-paced learning style allows students to review the information as many times as they wish. These advantages give students more opportunity to use the videos, and thus more opportunity to learn from them, potentially explaining the higher quiz scores from the experimental group.
Although the control group performed well on the quiz, they likely did not match the experimental group's scores because of the inherent disadvantages of traditional education. Lack of control over learning pace and inability to review content at a later date makes this educational method less convenient and makes it less likely that students will choose this method or learn from observing the demonstration only once [7]. Another factor that may play a role is the lack of reproducibility in skill demonstration compared with video education. Unless it is edited, a video series will remain the same each time it is watched. Skill demonstrations differ each time they are given, even if given by the same educator. This is because oral education is susceptible to human error [19] and because there are many factors involved in a live demonstration that are difficult to control, such as the environment, the educator's mood, and the dynamic of the group attending the session. The reproducibility of the videos ensures that all students will be given the same information in the same way each time. Another potential reason is that, even though students liked observing and practicing SST, it did not translate to knowledge retention and performance on the quiz.
Video education augments skill demonstration
Determination of which education method students preferred was less clear. The videos were reported to be more convenient, accessible, efficient, and useful for review than the skill demonstration, which fits with current literature [3,7,8] on the topic and the inherent qualities of video technology. Surprisingly, the skill demonstration was found to be easier to complete, despite the fact that many students commented that the sessions were too long. Students also reported that the skill demonstration helped them feel more prepared and retain more knowledge over time. This was attributed to the hands-on component of the session, which helped them remember and feel comfortable with the techniques. Although this feedback made determining overall educational method preference difficult, statistical analysis showed that how participants felt about the two different methods had no bearing on their quiz performance. For instance, although the follow-up survey results suggested that students perceived better knowledge retention after attending the skill demonstration, their quiz scores did not reflect this. This fits with current literature that demonstrates that individuals' self-assessment of their knowledge lacks accuracy compared with external assessment of their knowledge [20,21].
The video-specific feedback showed that students appreciated the flexibility and the individualized learning, but disliked that they could not physically practice the steps or ask questions. To address the inability to ask questions, a Frequently Asked Questions section could be created and added to the YouTube page hosting the videos to answer common student questions. Additionally, the interactive YouTube Comments section could be used to answer individuals who post questions. The page could also host YouTube Live sessions with experts on a regular basis to allow viewers to ask questions and receive answers in real time.
The skill demonstration-specific feedback made it clear that students valued the hands-on practice and enjoyed touring the operating room and interacting with the nurse educator, but disliked that the sessions took a long time to complete. Perhaps this is why only 1% of participants went back to see the nurse educator, while 28% of video participants re-watched the videos. This could be attributed to the fact that the skill demonstration was 90 minutes long, while the video series was only 30 minutes long. This could also explain why 82% of people thought the videos were more convenient and 94% thought they were more accessible than the skill demonstration.
Overall, the value of combining video education and skill demonstration was expressed by the students in this study and in the literature [4,5,17,18]. Thirteen students mentioned specifically in the survey that they saw value in using both methods. It also seemed like many of the “dislikes” regarding one method were represented as “likes” by the other method. For example, the most common dislike about the videos was that they were not hands-on, while this was the most liked thing about the skill demonstration. Similarly, students disliked the time commitment associated with the skill demonstration, but liked that they could learn at their own pace with the videos. Using the methods together would make up for their disadvantages. Other studies that showed effective learning by combining educational formats illustrated improved knowledge in the following areas: changing sterile dressings [4], scrub technique [5], suturing and knot tying [17], and hand-sewn small bowel anastomoses [18]. Ideally, this video series could be used to augment skill demonstration for teaching SST.
Limitations and future research
It is important to recognize the limitations of the study. Although the experimental participants did much better on the quiz, we do not know for sure whether this translates into better clinical performance of SST. A potential next step would be to repeat this study, but assess students' clinical performance of the skills rather than quiz performance. A modified version of the Student Observation Scale created by Patel et al. [22] could be used to rate performance. Furthermore, our quiz was developed by the study team, therefore we cannot report on its validity and reliability. To limit the opportunity for bias that creating the quiz ourselves presented, we based the content of the quiz and videos on the content of the skill demonstration session. In addition, the nurse educator who taught the skill demonstration was involved in creating the video scripts and quiz questions. This ensured that the quiz questions were not geared toward one education method, but rather tested knowledge of SST, which both education methods were designed to teach.
The study was unable to control for cheating on the quiz. To address this, an appeal was made to the students' professionalism during the recruitment and consent process, and they were asked not to share information with each other throughout the study (i.e., not to share the video link). Students were also assured that their quiz results would remain anonymous and have no bearing on their medical school grades or education to remove the temptation to cheat. To address this concern in the future, multiple monitored quiz writings could be arranged.
Conclusions
Video education is superior to traditional skill demonstration in helping first-year medical students retain knowledge on SST. Students who watched the videos displayed greater knowledge on the topic than those who attended a skill demonstration session. Video education is a great method to use when teaching medical students because it is convenient, accessible, and efficient [3,7,8]. Students can manipulate the videos by pausing and re-winding to learn at their own pace and can review the videos as many times as they wish. Video education can augment skill demonstration in teaching medical students about SST, the ultimate goal of which is to reduce SSIs.
Footnotes
Acknowledgments
We would like to thank Reid McKibbon and Benjamin Roth for their expert videography and creativity in producing the videos; Laura Smith, R.N., for her contributions to the videos and quiz; Kevin Verhoeff, Karl Narvacan, and Shauna Regan for their help with participant recruitment; the University of Alberta Hospital and operating room staff for their patience, support, and help with filming; the Surgical Infection Society for using the video series and quiz on their website to teach SST.
Author Disclosure Statement
Dr. Daithi Heffernan is the chair of the Informatics Committee for the Surgical Infection Society. Dr. Kamal Itani is the President of the Surgical Infection Society. Dr. Rachel G Khadaroo is a Councilor at Large and member of the Informatics Committee for the Surgical Infection Society.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.