
Abstract
Abstract
Background:
Although approximately 15% of all patients with acute colonic diverticulitis have pericolic extraluminal air found on computed tomography (CT), studies on the natural course and treatment of these patients are scarce. It is not clear whether these patients behave as mild uncomplicated diverticulitis or as severe diverticulitis needing more aggressive treatment. Consequently, there is no consensus about the treatment, guidelines do not discuss this group of patients, and physicians treat these patients based on their own experiences and opinion. An evidence-based approach is needed to prevent overtreatment or undertreatment in patients with pericolic extraluminal air.
Methods:
PubMed and EMBASE databases were searched for all studies reporting clinical outcomes of the initial diverticulitis episode of CT-proven left-sided colonic diverticulitis. Primary outcome measures were the need for emergency surgery and percutaneous abscess drainage.
Results:
A total of eight studies with 251 patients with pericolic extraluminal air were included. Rates of emergency surgery in isolated patients with pericolic extraluminal air were reported in six studies, yielding a pooled rate of 6% (95% confidence interval [CI] 3%–12%). In three studies reporting a combined total of only 56 patients, no patient underwent percutaneous abscess drainage. The long-term (6 mo) need for surgery was 38% in one study, although reasons for surgery were lacking.
Conclusion:
An initial 94% success rate of non-operative treatment in left-sided colonic diverticulitis patients with pericolic extraluminal air seems to justify a conservative approach including antibiotic agents. Low-quality evidence indicates the need for surgery in up to 38% in the medium-long term.
D
Pericolic extraluminal air (also termed covered perforation, micro- perforation, or localized perforation) is found in approximately 15% of all patients with acute diverticulitis on computed tomography [5,6]. Despite this relatively large proportion of patients, studies on the natural course and optimal treatment of pericolic extraluminal air are scarce. It is not clear whether pericolic extraluminal air should be considered uncomplicated or complicated diverticulitis, whether patients have a higher need for emergency surgery, whether patients are at high risk for progression to abscesses or free perforation, whether patients should be treated with antibiotic agents, or should be excluded for outpatient treatment. Only one guideline discusses the treatment of pericolic extraluminal air and recommends routine antibiotic treatment based on expert opinion without discussing any literature [7]. Moreover, commonly used diverticulitis classifications do not clarify the place of pericolic extraluminal air in the diverticulitis spectrum. The Ambrosetti classification only describes extraluminal air as severe diverticulitis and the modified Hinchey classification does not include this type of diverticulitis [8,9]. This lack of consensus about the nature of pericolic extraluminal air and treatment based on the experiences or opinion of individual physicians causes a risk of overtreatment or undertreatment. In summary, pericolic extraluminal air in acute colonic diverticulitis patients is in need of evidence-based treatment. This systematic review sought to gather all available evidence on the natural course and treatment of patients with pericolic extraluminal air to be able to make an evidence-based recommendation for the treatment of these patients.
Methods
Study identification
Two authors (S.vD. and S.D.) searched PubMed and EMBASE databases independently with the following search terms: diverticulitis, diverticular, complicated, perforation, air, micro perforation, pneumoperitoneum, bubble, and gas (Supplementary Table S1; see online supplementary material at http://www.liebertpub.com/sur). No language limits were applied. The search was limited by dates later than 1980 and the last search was performed in February 2017. Reference lists of obtained articles were reviewed for any omitted studies. Meta-analysis of Observational Studies in Epidemiology (MOOSE) guidelines for reporting were followed [10]. A review protocol for this systematic review was not published or registered before this study was undertaken.
Study selection
Studies that were considered for eligibility included randomized clinical trials; prospective cohort studies and retrospective cohort studies; studies that reported outcomes of left-sided colonic diverticulitis patients with isolated pericolic extraluminal air; and studies confirmed with computed tomography (CT). No specific definition of pericolic extraluminal air was required, although a clear distinction from free air was required. Studies that only included patients who underwent emergency surgery were excluded. Reviews, letters, case reports, and case series smaller than five patients were also excluded. The two reviewers independently considered all studies retrieved from the search for eligibility against these criteria. Any disagreements were resolved through discussion.
Quality assessment
The two reviewers (S.vD. and S.D.) appraised each study critically using the Newcastle Ottawa Quality Assessment Scale for cohort studies [11]. Any disagreements were resolved through discussion.
Data extraction
The two reviewers (S.vD. and S.D.) reviewed each included article independently. Each reviewer extracted the data on a predefined evidence table, after which the two tables were compared. Any disagreements were resolved through discussion. Data collected from each article was study design and setting; inclusion and exclusion criteria for the study; routine treatment protocol; definition of pericolic extraluminal air; type of patients in the control group; reported outcome measures with results; and follow-up period. The corresponding author was contacted if reported results were insufficient for use in this systematic review.
Outcome measures
Primary outcome measures were need for emergency surgery and/or need for percutaneous abscess drainage during the initial acute diverticulitis episode. Other outcome measures that described the disease course of the acute diverticulitis episode were also reviewed as secondary outcome.
Statistical analysis
The rates of need for emergency surgery in the pericolic extraluminal air group were pooled and displayed using a forest plot and a random effects model. Statistical heterogeneity was assessed using χ2 and I2. Statistical analyses were conducted using RStudio (RStudio Inc., Boston, MA).
Results
Systematic review
The search retrieved 5,857 studies. After removal of 1,315 duplicates, the titles and abstracts of 4,542 studies were screened. A total of 4,353 studies were excluded after which 189 full-text articles were assessed for eligibility. Eight studies fulfilled the inclusion and exclusion criteria and were included in this review. The search strategy is shown in Figure 1. The reasons for exclusion of the remaining 181 full-text articles are listed in Supplementary Tables S2A and 2B.
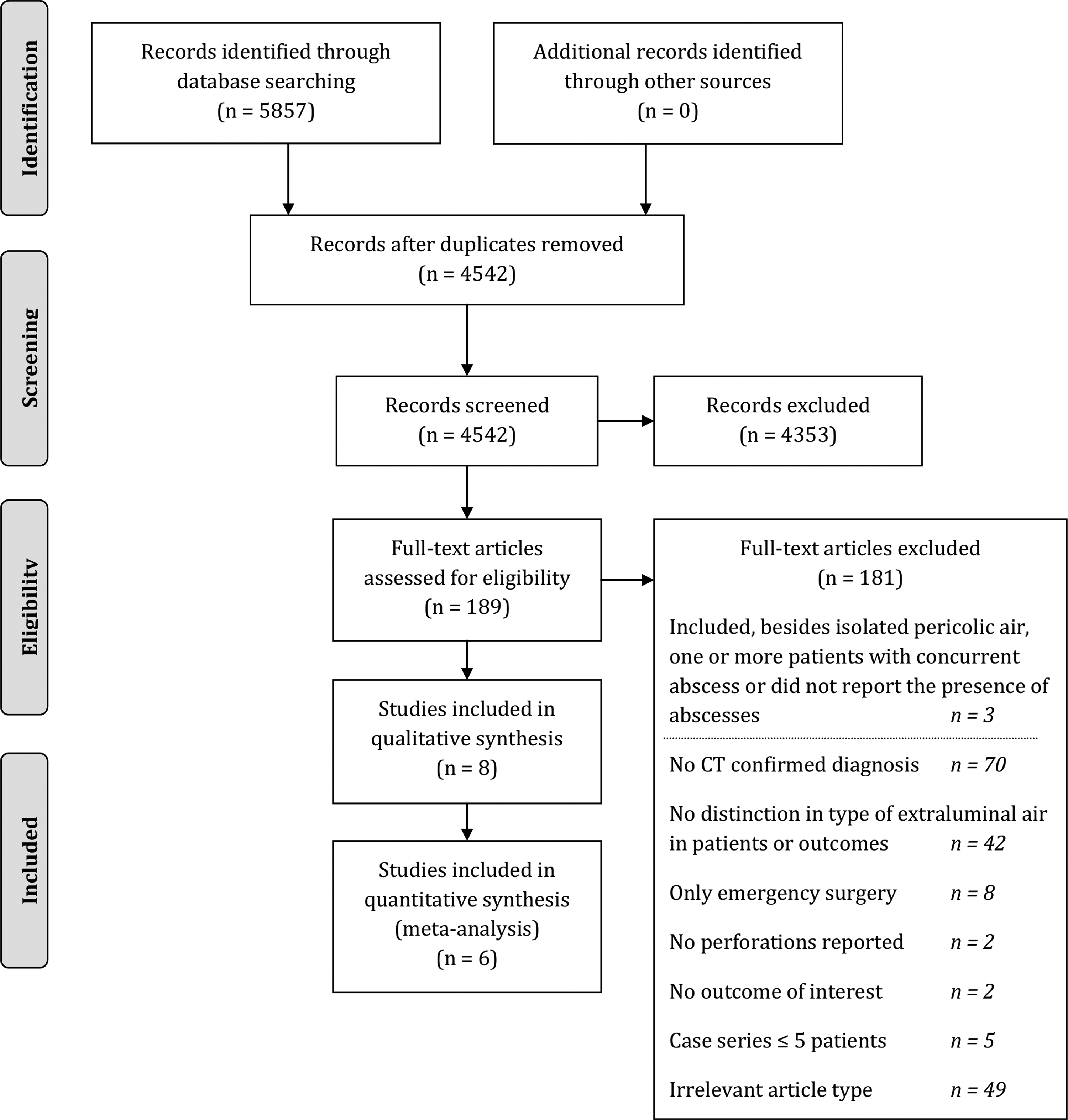
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (RISMA) flow diagram [22].
Study characteristics
Three prospective cohort studies [12–14] and five retrospective cohort studies [6,15–18] were included. Six studies were conducted in Europe and two studies in the United States. Although all studies separated patients with pericolic extraluminal air from patients with distant free air, a variety of definitions for pericolic extraluminal air was used. Only three studies clearly specified the location of the extraluminal air as within 5 cm of the inflamed bowel segment. Other studies applied definitions such as “contained perforation,” “localized pericolic free air,” and “air within the mesentery.” Because pericolic extraluminal air was not the primary aim of all studies, some studies applied inclusion criteria that may have caused selection bias for patients with pericolic extraluminal air. Specifically, a Spanish study only included patients without comorbidity and with absence of all systemic inflammatory response syndrome (SIRS) criteria [13].
In six studies all patients were treated with antibiotic agents, one study [14] only treated some of the patients with antibiotic agents, and one study [18] did not mention antibiotic treatment at all. The most reported outcome measure was need for emergency surgery (seven studies), followed by need for percutaneous abscess drainage (three studies). One study only reported a long-term outcome, namely, need for surgery within six months [17]. A control group was included in three studies, whereas only one study [13] compared the patients with pericolic extraluminal air to patients with uncomplicated diverticulitis. The other two studies [14,18] made a comparison of a group of patients containing perforations or abscesses. The complete evidence table is shown in Supplementary Table S3 and a summary of the included studies and results is shown in Table 1.
Numbers confirmed with authors because of incomplete data.
Pros = prospective cohort study; Retro = retrospective cohort study; NR = not reported; PEA = pericolic extraluminal air; CG = control group; SIRS = systemic inflammatory response syndrome.
Population characteristics
A total of 251 patients with pericolic extraluminal air were included in this review. Rates of emergency surgery were reported in 195 patients and percutaneous abscess drainages in only 56 patients.
Critical appraisal
Table 2 shows the Newcastle Ottawa risk of bias assessment. The main factors leading to risk of bias were the lack of control groups or the nonrepresentative nature of the control groups. Furthermore, only a few studies reported the duration of follow-up. Therefore, it is not clear if all studies reporting the need for emergency surgery had comparable follow-up duration and if the follow-up duration was sufficient to detect the true need for emergency surgery during the diverticulitis episode of pericolic extraluminal air.
Primary outcomes: need for emergency surgery and percutaneous abscess drainage
Seven studies reported rates of emergency surgery. Six studies provided crude data and could be pooled in a forest plot (Fig. 2). A pooled rate of 6% (95% CI 3%–12%) of patients with pericolic extraluminal air underwent emergency surgery. One study [18] only reported an adjusted odds ratio for the need for emergency surgery (0.03, 95% CI 0.01–0.08). However, because the control group consisted of all patients including free perforation, interpretation of this odds ratio is difficult.
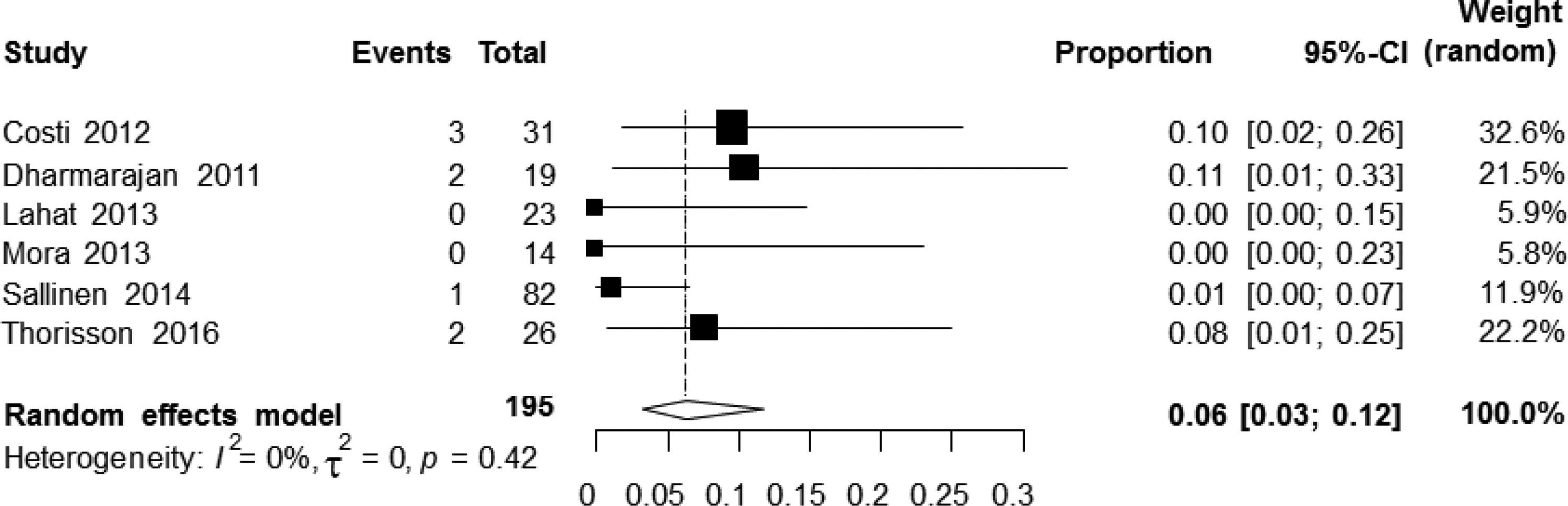
Forest plot of studies reporting rates of need for emergency surgery in patients with pericolic extraluminal air.
The need for percutaneous abscess drainage was reported in only 3 studies [12,13,16]. From a combined total of 56 patients, no patients underwent percutaneous abscess drainage. A comparison of rates of emergency surgery between patients with pericolic extraluminal air and patients with uncomplicated diverticulitis was reported in only one study [13]. In this study, no patients underwent emergency surgery or percutaneous abscess drainage in both the pericolic extraluminal air group and the uncomplicated control group [13].
Secondary outcome
One study did not only assess emergency surgery rates during the initial acute diverticulitis episode but reported a combined rate of emergency or elective surgery. This American study found that 37.5% (21/56) of patients underwent surgery within six months [17]. Reasons for these resections and the proportion of elective resections were not reported.
Discussion
This systematic review found a 6% (95% CI 3%–12%) need for emergency surgery rate in patients with isolated pericolic extraluminal air and left-sided colonic diverticulitis. Furthermore, data on the need for percutaneous abscess drainage were insufficient to draw conclusions. In the medium-long term (6 mo), need for surgery was 38% but reported in one study onlyand reasons for or timing of surgery were unclear.
Despite the frequent occurrence of pericolic extraluminal air in patients with acute diverticulitis, little is known about the natural course and required treatment. Only six studies reported the need for emergency surgery in this group of patients, and the number of patients was low. Also, no earlier systematic review was performed. The lack of interest in research on this frequent presentation of acute diverticulitis is remarkable. Consequently, only one guideline discusses this group of patients and only makes a recommendation based on expert opinion [7]. Presumably, patients with pericolic extraluminal air are currently treated based on personal experiences and opinions. It is unclear whether these patients are considered to be uncomplicated and treated conservatively, or considered complicated and treated more aggressively. This aggressive treatment may even include routine emergency surgery because of the fear of subsequent clinical deterioration. This systematic review showed that the vast majority of these patients has an initial benign course and does not need an emergent intervention.
This review is limited mainly by the source of the data. All included studies were observational cohort studies of which only three were prospective. Furthermore, the applied methods in these patients differed or were described poorly. The follow-up duration was not reported in five of eight studies and control groups were for the most part not available or not representative. Also, most studies did not define the decision process for emergency surgery, either for emergency surgery or for surgery during follow-up. Therefore, it is unclear for which reasons the patients needed surgery. The influence of the clinical condition of the patient at presentation was not described, and the presence of pericolic extraluminal air itself may have been decisive in the subjective decision whether or not to operate. The presence of extraluminal air may lower the threshold for surgery because of the fear of progression into free perforation, thereby the presence of extraluminal air is a self-fulfilling prophecy for surgery. Because some of the patients may develop an abscess instead of free perforation, one may deliberate whether some patients could also have been treated successfully with percutaneous drainage instead of surgery. However, the need for percutaneous drainage was only reported in three studies including 56 patients. Therefore, valuable information on the need for interventional treatment in these patients is missing. Also, the role of antibiotic agents in the treatment of pericolic extraluminal air remains unclear because almost all studies treated their patients with antibiotic agents routinely or the studies did not state whether antibiotic treatment was used. A strength of this systematic review is that although the available evidence is low quality and the number of patients is relatively low, all currently published evidence on pericolic extraluminal air was described because of the search and selection strategy. There were no selection criteria regarding patient characteristics or outcome measures, and a broad search was performed.
The 6% need for emergency surgery in patients with pericolic extraluminal air in this review is slightly higher than the 1%–2% need for emergency surgery in patients with uncomplicated diverticulitis reported in the literature [19–21]. However, because of the methodological limitations of the included studies, this rate is an estimate and requires confirmation in larger prospective studies applying a clearly defined treatment protocol. Moreover, percutaneous abscess drainage is a frequently used modality to treat diverticular complications and therefore information is needed whether these patients need drainage because of abscess formation during the course of their disease. Although pericolic extraluminal air seems to have a slightly more virulent course than uncomplicated diverticulitis, the 94% success rate of initial nonoperative treatment in these patients seems to justify a conservative approach. Because evidence on nonantibiotic treatment of these patients is lacking, routine antibiotic treatment seems appropriate.
Footnotes
Acknowledgments
The collaborators and members of the Dutch Diverticulitis Guideline Committee are: M.A. Boermeester, S.T. van Dijk, W.A. Draaisma (Academic Medical Center, Amsterdam, The Netherlands); J.B.C.M. Puylaert (Haaglanden Medical Center, The Hague, The Netherlands); W.A. van Enst (Knowledge Institute of Medical Specialists, Utrecht, The Netherlands); M.G.J. de Boer (Leiden University Medical Center, Leiden, The Netherlands); B.R. Klarenbeek (Radboud University Medical Center, Nijmegen, The Netherlands); R.J.F. Felt (VU University Medical Center, Amsterdam, The Netherlands); H. Otte (ZorgSaam Hospital, Terneuzen, The Netherlands).
Funded by the Association for Quality Funds Medical Specialists (SKMS).
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.