
Abstract
Abstract
Background:
This purpose of this study was to investigate the effects of blood stream infections (BSIs) on the prognosis of patients with complicated intra-abdominal infections (IAIs) and to make predictions based on patients' characteristics on admission.
Patients and Methods:
One hundred eighty-seven patients with complicated IAI in 2014 and 2015 were included in our retrospective analysis, except for those diagnosed with central line-associated blood stream infections (CLABSIs). Patients with BSIs were compared with patients without BSIs. Multivariable logistic regression was applied to identify factors associated with BSIs and also the subtypes of BSIs. The predictive score systems were established further.
Results:
Seventy-four patients (39.6%) with complicated IAIs developed BSIs after admission. Four factors evaluated on admission were associated independently with BSIs including alanine aminotransferase (ALT) ≥66 U/L (two scores), insensitivity to initial empirical antibiotic agents (IIEA; three scores), Sepsis-Related Organ Failure Assessment (SOFA) score of two or more (three scores), and generalized peritonitis (four scores). A total score of five or more was regarded as the critical value in the combined test to predict BSIs, with a sensitivity of 0.78 and a specificity of 0.73. Blood stream infections were further divided as secondary BSIs and non-secondary BSIs. The risk factors of secondary BSIs included IIEA (three scores), SOFA score of two or more (five scores), and generalized peritonitis (eight scores), where a total score of nine or more was regarded as the critical value in the combined test, with a sensitivity of 0.68 and a specificity of 0.87, whereas the risk factors of non-secondary BSIs included IIEA (three scores), SOFA score of two or more (three scores) and procalcitonin (PCT) ≥0.43 mcg/L (three scores), where a total score of six or more was regarded as the critical value in the combined test, with a sensitivity of 0.75 and a specificity of 0.70. Moreover, BSIs were linked with the worse clinical outcomes in organ functions, hospitalization costs, and mortality.
Conclusions:
Our new scoring methods may have potential advantages on the early prediction and recognition of BSIs in patients with complicated IAIs.
I
Blood stream infections (BSIs) were proved to be a negative factor for prognosis [7–9]. By secreting toxin into the blood stream, pathogens could induce the inflammatory reaction and attack the host again, thus exacerbating the patient's illness [10]. Patients in a state of immunosuppression were susceptible to bacterial dissemination [11,12]. Therefore, the occurrence of BSIs might be an indicator of the affected patient's poor condition. Early recognition of the risk factors of BSIs may be a practical way to prevent them and reverse the deterioration of primary diseases. However, the risk factors and impacts of BSIs on patients with complicated IAIs were rarely reported. The aim of our study was to find the risk factors for BSIs (including secondary and non-secondary BSIs) and the relation to clinical outcomes for patients with complicated IAIs as well as to establish scoring methods for early prediction.
Patients and Methods
Inclusion and exclusion criteria
The inclusion criteria were as follows: (1) at least 18 years old, (2) positive microbial culture of abdominal drainage fluid, (3) confirmation of abscess in abdominal space or peritonitis on admission by physical examination and computed tomography (CT) scanning, and (4) at least one blood culture in hospital when BSIs were suspected. The patients were included in our analysis only when all inclusion criteria were met. The exclusion criteria were a state of septic shock on admission and central line-associated BSIs in hospital. Central line-associated blood stream infections (CLABSIs) were ruled out because they were related to the aseptic technique and catheter care rather than complicated IAIs [13,14]. Patients with septic shock were also excluded because most of them experienced obviously delayed transfers or non-standardized treatment of complicated IAIs. A majority of patients were referred to the emergency department first and then transferred to our department. The medical documents from two departments were checked to preclude errors of participants' enrollment in our study.
Definition of terms
In this study, BSIs were defined as newly presented BSIs of patients with complicated IAIs more than 48 hours after admission [15], provided that CLABSIs were ruled out. Central line-associated BSIs were diagnosed when highly suspected by meeting one of the following three criteria: (1) the same bacteria were obtained in blood cultures and catheter tip cultures taken at the same time, with a positive semi-quantitative (>15 colony forming units per catheter segment) or quantitative (>103 colony forming units per catheter segment) culture; (2) simultaneous quantitative cultures of blood samples with a ratio of ≥3:1 (central venous catheter [CVC] vs. peripheral); (3) a differential period of CVC culture versus peripheral blood culture positivity of two hours [16,17]. The definition of secondary BSIs was referred to a recent version of U.S. Centers for Disease Control and Prevention (CDC) guideline with meeting one of the following two criteria [18]: (1) at least one organism from the blood specimen matches an organism identified from complicated IAIs, which is collected during the secondary BSI attribution period (infection window period: three days before and after the date of event plus repeat infection time frame: 14 days after the date of event); (2) an organism identified in the blood specimen is an element that is used to meet the National Healthcare Safety Network (NHSN) site-specific infection criterion, and therefore is collected during the window period of complicated IAIs. Non-secondary BSIs were defined as BSIs excluding CLABSIs and secondary BSIs. The state of shock was considered when using noradrenaline for hypotension in a dose of more than 0.1 mcg/kg per minute on admission [15]. Insensitivity to initial empirical antibiotic agents was confirmed when the result of the microbiologic culture indicated that at least one pathogen was not susceptible to the antibiotic agents administrated in the first 48 hours after admission or the dose was not adequate [19]. Respiratory failure was defined by the need for more than 24 hours of mechanical ventilation. Sequential Organ Failure Assessment score (SOFA) was based on six different scores consisting of respiratory, cardiovascular, hepatic, coagulation, renal, and neurologic factors.
Study design and patients
Patients with complicated IAIs were transferred from peripheral hospitals to our national center of intra-abdominal infections. Some developed BSIs after admission, leading to an increased threat to patients. To recognize the risk factors and predict BSIs earlier, 187 patients with complicated IAIs were reviewed over a two-year period (from January 2014 to December 2015). Among 187 patients, 74 patients had at least one positive blood culture after 48 hours of hospitalization whereas 93 patients had blood cultures with negative results and 20 patients were not suspicious of BSIs. For those with positive blood cultures, 46 patients were secondary BSIs and 28 patients were non-secondary BSIs based on the definitions above. Patients with BSIs in hospital were compared with those without BSIs. Basic information was obtained by means of retrospectively referring to the patients' medical documents including the age, body mass index (BMI), gender, underlying disease, number of surgeries before transfer, baseline characteristics at the first 24 hours of hospitalization, and results of laboratory tests as well as microbiologic cultures on admission.
Patients were grouped into non-BSI and BSI, and sub-grouped into non-BSI and secondary BSI and non-BSI and non-secondary BSI to identify the risk factors and generate scoring systems. The differences of clinical outcomes such as organ failure, mortality, and hospitalization costs between the non-BSI and BSI groups were also analyzed for exploring the effects of BSIs on the prognosis of patients. All patients received normalized drainage and antibacterial agents within 24 hours after admission.
Statistical analysis
Basic information including age, gender, underlying disease, classification of infections, patient's condition on admission, and the results of laboratory tests was analyzed via a χ2 test for qualitative variables and a two-sided t-test for quantitative variables. A multivariable stepwise logistic regression model (backward Wald model) was built to identify any independent factors for BSIs, secondary BSIs, and non-secondary BSIs on patients with complicated IAIs. Only significant parameters (p < 0.05) were included in the multivariable model. All potential explanatory parameters (p < 0.05) would be submitted to a collinearity analysis in a correlation matrix. Intercorrelated variables were be kicked out in the multivariable model (tolerance <0.3 and variance inflation factor >3). Odds ratios (OR) and their 95% confidence intervals (CI) were reported. The constant would be included in case of statistical significance. The Hosmer-Lemeshow test was used to evaluate the model's goodness of fit. The statistical significance of each regression coefficient was assessed with Wald χ2 test [20].
According to the odds ratios in the multivariable analysis, scoring methods were developed and tested by receiver operating characteristic (ROC) curves [21]. The best score's cutoff was detected by the Youden index to maximize the sum of sensitivity and specificity. The data of clinical outcomes for the two groups were also analyzed through a χ2 test and a two-sided t-test. The survival curve in the first month of hospitalization was demonstrated using life table and compared by Wilcoxon test.
Results
One hundred eighty-seven patients were included in our retrospective analysis. Of these, 74 (39.6%) experienced BSIs after admission. The primary diseases of those patients are listed in Table 1, where trauma and tumor are the most frequent. The results of blood sample culture and peritoneal drainage fluid culture are presented in Table 2 Gram-negative bacteria comprised more than 60% of clinical samples of complicated IAIs and BSIs, of which the extended-spectrum β-lactamase (ESBL)-producing Escherichia coli and ESBL-producing Klebsiella pneumoniae in the complicated IAIs are 33.8% and 21.3%, respectively, whereas in the BSIs are 43.8% and 31.8%, respectively. For secondary BSIs, the proportion of the gram-negative bacteria was also more than 60%. The susceptibility patterns of some common pathogens are shown in Supplementary Table S1 (see online supplementary material at http://www.liebertpub.com/sur), where Escherichia coli, Klebsiella pneumoniae, and Acinetobacter baumannii are main bacteria that lead to the failure of initial empirical antibiotic agents because of ESBL-producing bacteria.
Results are expressed as the number (proportion, in %).
BSI = blood stream infection; IBD, inflammatory bowel disease.
Results are expressed as the number (proportion, in %).
BSI = blood stream infection; IAI = intra-abdominal infections.
Predictive factors of BSIs
Demographic data are reported in Table 3. Age, BMI, gender, underlying diseases, and the classification of infections turned out to lack statistical significance. The condition of patients on admission differed substantially between the BSI group and non-BSI group. More patients received parenteral nutrition in the BSI group than in the non-BSI group (54.1% vs. 38.1%, p = 0.03). The average number of surgeries before patients' transfer in the BSI group (1.41) was higher than in the non-BSI group (1.16). Forty-six patients (62.2%) in the BSI group were proved to have generalized peritonitis whereas in the non-BSI group there were 27 (23.9%; p < 0.001). The percentage of pneumonia in patients transferred to our department was 70.3% (52/74) in the BSI group and 59.3% (67/113) in the non-BSI group (p = 0.16). The mean of SOFA scores on admission was 4.9 in the BSI group compared with 1.3 in the non-BSI group (p < 0.001). The microbiologic culture confirmed that 41 (55.4%) patients in the BSI group were insensitive to the initial empirical antibiotic agents compared with 27 (23.9%) in the non-BSI group.
Days from onset of cIAIs at the previous hospital until the time to transfer to our facility.
Results are expressed as the number (proportion, in %) or mean ± standard deviation.
BSI = blood stream infection; BMI = body mass index; SFTP = surgical frequency before transferring the patients; APACHE II = Acute Physiology and Chronic Health Evaluation II; SOFA = Sepsis-Related Organ Failure Assessment; IIEA = insensitivity to initial empirical antibiotics.
Table 4 provides the outcomes of laboratory tests in a dichotomous form, determined by their normal ranges or median values. Two items including alanine aminotransferase (ALT) ≥66 U/L and procalcitonin (PCT) ≥0.43 mcg/L were different between the BSI group and non-BSI group. To be precise, 32 (43.2%) patients exhibited ALT over 66 U/L in the BSI group whereas only 24 (21.2%) patients in the non-BSI group did so (p = 0.001). The proportion of PCT ≥0.43 mcg/L in the BSI group (44/74, 59.5%) was also higher than that in the non-BSI group (48/113, 42.5%; p = 0.02).
Platelet (normal, 125–350 × 109/L). WBC = white blood cell (normal, 3.5–9.5 × 109/L); ALT = alanine aminotransferase (normal, 13–66 U/L); AKP = alkline phosphatase (normal, 38–126 U/L); total protein (normal, 63–82 g/L); bilirubin (normal, 3–22 mcmol/L); creatinine (normal, 58–110 mcmol/L); PCT = procalcitonin (normal, <0.046 mcg/L); CRP = C-reactive protein (normal, 0–8 mg/L).
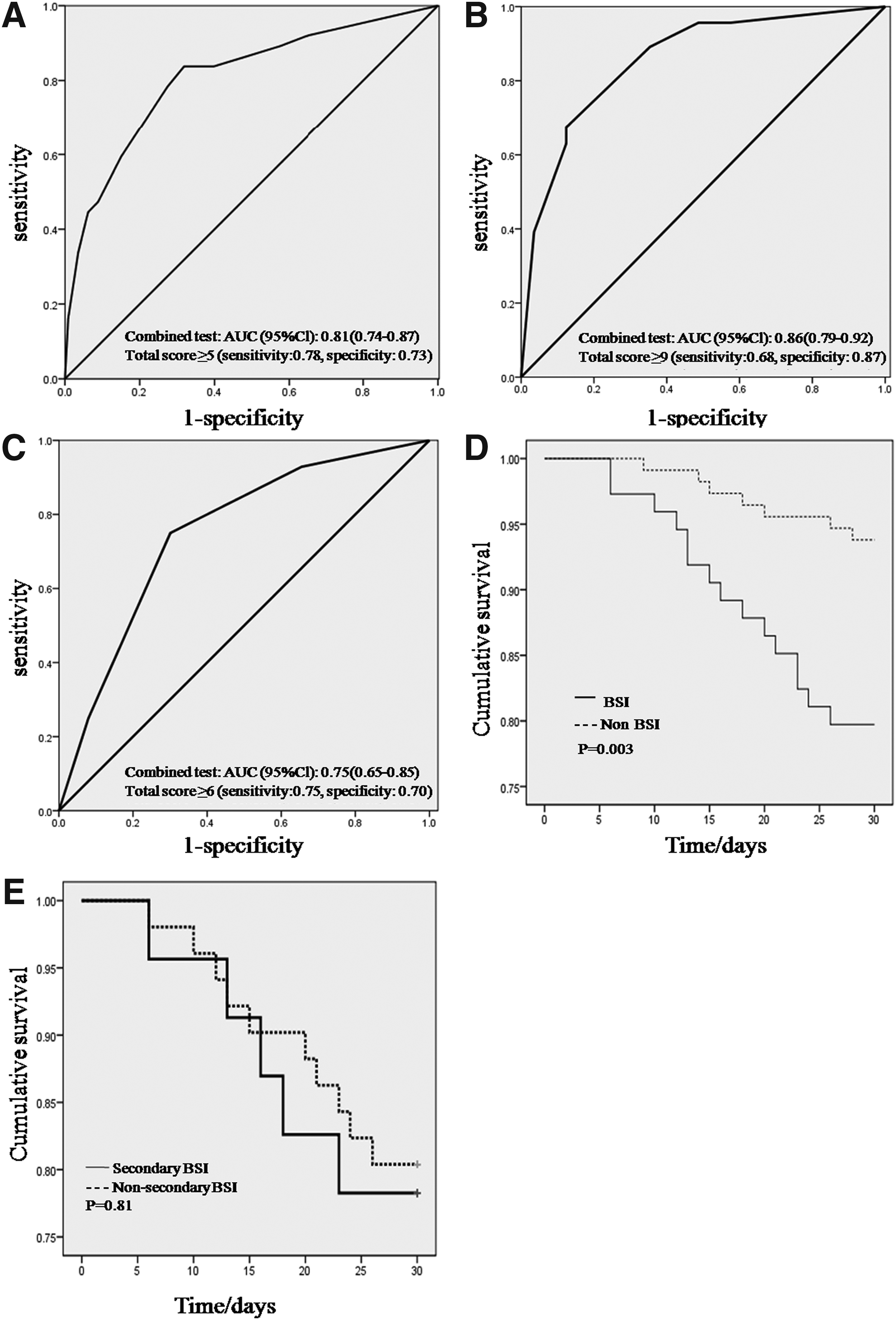
The results of the multivariable analysis are presented in Table 5. Four independent factors were predictive of BSIs: (1) ALT ≥66 U/L; (2) insensitivity to IIEA; (3) SOFA score ≥2; and (4) generalized peritonitis. The model's Wald χ2 statistic was 62.5 (p < 0.001). The Hosmer-Lemeshow test statistic was 5.2 (p = 0.64). These four factors were given 2, 3, 3, 4 scores respectively in Table 6, which could be used to forecast BSIs with AUC of 0.81 (Fig. 1A). The best score's cutoff was 5 with a sensitivity of 0.78 and specificity of 0.73. Supplementary Figure S1 shows the distribution of BSIs for each score in the combined test. In addition, three independent factors were associated with secondary BSIs: (1) IIEA; (2) SOFA score ≥2; and (3) generalized peritonitis. The model's Wald χ2 statistic was 49.3 (p < 0.001). The Hosmer-Lemeshow test statistic was 3.3 (p = 0.86). These three factors were given 3, 5, 8 scores, respectively, in Table 6, which could be used to forecast secondary BSIs with AUC of 0.86 (Fig. 1B). The best score's cutoff was 9 with a sensitivity of 0.68 and specificity of 0.87. For non-secondary BSIs, there were also three independent factors: (1) IIEA; (2) SOFA score ≥2; (3) PCT ≥0.43 mcg/L. The model's Wald χ2 statistic was 18.8 (p < 0.001). The Hosmer-Lemeshow test statistic was 3.37 (p = 0.64). These three factors were given three, three, and three scores, respectively (Table 6), which could be used to forecast secondary BSIs with AUC of 0.75 (Fig. 1C). The best score's cutoff was 6 with a sensitivity of 0.75 and specificity of 0.70.
(
ALT = alanine aminotransferase (normal, 13–66 U/L); IIEA = insensitivity to initial empirical antibiotics; SOFA = Sepsis-Related Organ Failure Assessment; PCT = procalcitonin (normal, <0.046 mcg/L); OR = odds ratio; CI = confidence interval.
ALT = alanine aminotransferase (normal, 13–66U/L); IIEA = insensitivity to empirical initial antibiotics; SOFA = Sepsis-Related Organ Failure Assessment; PCT = procalcitonin (normal, <0.046 mcg/L).
Impacts of BSIs on patient prognosis
The clinical outcomes were also different in the presence of BSIs as shown in Table 7. Organ failure concerning the respiratory, cardiovascular, and renal system was more pronounced in the BSI group than in the non-BSI group (p ≤ 0.01). Patients with BSIs were likely to stay in the intensive care unit longer and with higher costs (p < 0.001). Also, the BSIs might be responsible for the lower cumulative survival shown in Figure 1D. Further survival analysis was performed on the secondary BSIs and non-secondary BSIs, which revealed they had a similar one-month mortality (p = 0.81; Fig. 1E).
Results are expressed as the number (proportion, in %) or mean ± standard deviation.
LOS = length of stay; ICU = intensive care unit; RMB = renminbi.
Discussion
Our study clearly verified the negative associations of BSIs on clinical outcomes of patients with complicated IAIs in terms of organ failure, hospitalization costs, and as death rates. Four risk factors are related to the episodes of BSIs including ALT ≥66 U/L, SOFA score ≥2, IIEA, and generalized peritonitis. Regarding subtypes of BSIs, the risk factors of secondary BSIs include SOFA score ≥2, IIEA, and generalized peritonitis, whereas they are SOFA score ≥2, IIEA, and PCT ≥0.43 mcg/L for non-secondary BSIs.
To our knowledge, ALT is a vital biomarker of liver injury. Guo et al. [22] also observed the early liver dysfunction in the cohort of IAIs. Basic research revealed that the liver injury may be a result of intestinal mucosal barrier impairment, bacterial translocation, and deficiencies of local host immune defenses [23,24]. Deranged clearance of endogenous bacteria from portal and systemic circulation turns the gut into the major source of bacteria-related complications, including BSIs. Therefore, methods to protect the intestinal mucosal barrier are of clinical importance. In this study, we found that patients receiving enteral nutrition were less likely to present liver injury and BSIs. This phenomenon suggests that early enteral nutrition may have a protective role of liver damage and gut microbiota-related infections. The underlying mechanisms may attribute to maintenance of intestinal mucosal barrier functions and prevention of bacterial translocation [25,26].
Sepsis-Related Organ Failure Assessment score ≥2 is another risk factor of BSIs. In a current guideline (Sepsis-3), sepsis is defined as the co-existence of infections and SOFA score ≥2 [27]. This means that patients in a state of dysregulated response to infections and organ damage are more susceptible to BSIs. For example, Lonneke et al. [15] suggested that immunosuppression induced by sepsis increased the incidence rate of secondary infections with associated late mortality. On the cellular level, patients with sepsis were vulnerable to hyporesponsiveness, exhaustion, and apoptotic depletion of immunocytes and an increase in T-regulatory and myeloid-derived suppressor cells [28,29]. Therefore, supportive management is required as early as possible to reverse the process of sepsis and maintain a good immune state.
Insensitivity to initial empirical antibiotic agents was also related to BSIs. Although we attempted to become familiar with the local bacterial patterns, the failure of antibiotic therapy was encountered because of the shifting of drug-resistant microbes caused by ESBL-producing and carbapenemases-producing bacteria [30]. Two possible methods may be helpful to overcome the problem. On the technical level, the time needed to identify the bacterial species has been reduced [31,32] and also their antibiotic susceptibilities [33]; however, only a minority of hospitals can access them. A more practical way is to perform the early adequate source control as recommended in a revised version of IAIs guideline [34], since Sawyer et al. [35] found that source control was able to maintain the treatment effectiveness even if the duration of the antibiotic agents was decreased from eight days to four days.
Generalized peritonitis was also associated with BSIs. This finding was consistent with that reported by Dupont et al. [36], who recognized it as a predictive factor of candidemia. Generalized peritonitis resulted from a failure of source control in hospital before transfer and also increased the difficulties in starting source control in our center [37], leading to long-term residue of intra-abdominal bacteria that was favorable of their dissemination into blood. Therefore, once generalized peritonitis was persistent and the general conditions of patients deteriorated, the on-demand relaparotomy needed to be performed [38].
The limitation of our study is that it is a retrospective analysis with small samples, inevitably creating bias. Further prospective studies are needed to confirm our findings and clarify how these risk factors act on the BSIs. In addition, the definition of secondary BSIs is still not accurate because the culture results cannot confirm that the pathogens in the BSIs originated from the complicated IAIs. Genetic techniques are needed to overcome this disadvantage.
Conclusion
Our retrospective study first demonstrated that BSIs (regardless whether secondary BSIs or non-secondary BSIs) could be lethal factors for patients with complicated IAIs, ALT ≥66U/L (two points), IIEA (three points), SOFA score ≥2 (three points), and generalized peritonitis (four points) on admission are the risk factors for developing BSIs. A total score over five points has a satisfactory ability to predict the BSIs as well as allowing clinicians to have greater vigilance to restrict these risk factors at an early stage and to send blood cultures once new signs of infections occur.
Footnotes
Acknowledgments
This study was approved by the Institutional Review Board of Jinling Hospital and our work was in compliance with the Helsinki Declaration.
The data supporting the findings of our study were included in the tables, figures or supplementary materials.
Jinjian Huang, Jianan Ren and Steven W. M. Olde Damink designed this study. Jinjian Huang, Jiao Jiao, Xiuwen Wu collected the patients' data. Jinjian Huang and Luise Brakert analyzed the data and organized this article. Gefei Wang and Steven W.M. Olde Damink monitored this study and gave advice on this research. Jinjian Huang, Qinjie Liu and Jianan Ren revised the manuscript.
This research was funded by the National Natural Science Foundation of China (Grant no. 81571881) and Key Project of Jiangsu Social Development (Grant no. BE2016752).
We are very thankful to all staff in the Department of Microbiology at Jinling Hospital for providing the results of microbiological cultures.
Author Disclosure Statement
We declare no potential conflicts of interest with respect to the research, authorship, and publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.