
Abstract
Abstract
Background:
The non-steroidal anti-inflammatory drug diclofenac has been associated with intestinal anastomotic leakage, although the underlying pathophysiology is unclear. Previous data suggest that reactivation of biliary diclofenac metabolites by microbial β-glucuronidases in the gut plays a role in harming the intestinal mucosa, and that microbiome-targeted glucuronidase inhibition prevents this damage. Here, the microbial glucuronidase inhibitor Inh1 was examined for its ability to reduce diclofenac-induced anastomotic leakage in rats.
Methods:
Ninety male Wistar rats were allocated to five groups. In the two diclofenac groups, group DCF received diclofenac (3 mg/kg per day) and group DCF-Inh1 additionally received 800 mcg/kg per day of glucuronidase inhibitor Inh1 solution orally. In non-diclofenac groups, animals received either Inh1 (800 mcg/kg per day; group Inh1) solution, the vehicle (methylcellulose; group Veh), or no solution (group Ctrl). All solutions were provided from the day of surgery until sacrifice on day three. Plasma concentrations of diclofenac were determined. Outcomes were anastomotic leakage, leak severity, and anastomotic strength.
Results:
Anastomotic leak rates were 89% in group DCF and 44% in group DCF-Inh1 (p = 0.006). Leak severity was reduced in group DCFic-Inh1 (p = 0.029). In non-diclofenac cohorts, mostly minor leakage signs were observed in 25% in group Ctrl, 39% in group Inh1 (0.477), and 24% in group Veh (p = 1.000). Bursting pressure and breaking strength were not significantly different. Plasma concentrations of diclofenac were not changed by Inh1.
Conclusion:
Microbial glucuronidase inhibitor reduces diclofenac-induced anastomotic leakage severity, which suggests a harmful effect of diclofenac metabolite reactivation in the gut. This finding improves the understanding of the pathogenesis of anastomotic leakage.
T
Diclofenac is excreted mostly through bile and we demonstrated previously that alterations in bile composition disturb healing of anastomoses [9] (unpublished data). This finding shows similarities with results of studies on NSAID-induced enteropathy [9–15]. A range of compounds, including NSAIDs such as diclofenac, are detoxified by addition of glucuronic acid moieties by liver-resident UDP-glucuronosyltransferase (UGT) enzymes, and excreted through bile. In the gut the glucuronic acids are enzymatically cleaved from drug conjugates by microbial ß-glucuronidase. These re-activated previously detoxified conjugates damage the intestinal epithelium, and in the case of NSAIDs, result in enteropathy and mucosal damage [16–18]. We have demonstrated previously that inhibiting bacterial ß-glucuronidase using potent, bacteria-selective, non-lethal inhibitors protects the intestinal mucosa from damage resulting from the anti-cancer drug CPT-11, which is also excreted as a glucuronide [19]. In subsequent studies, we have applied this inhibitor, termed Inhibitor 1 (Inh1), in a model of NSAID-induced enteropathy [180. By co-administering Inh1 with an ulcerogenic dose of diclofenac, we found that Inh1 reduces the multiplicity and area of small intestinal ulcers, reduces epithelial permeability, and decreases systemic concentrations of serum alkaline phosphatase, a widely accepted biomarker of enteropathy [20]. Notably, pharmacokinetics of diclofenac remained unchanged, indicating the analgesic benefit of the compound is not affected by Inh1 treatment. Similar results were observed with ketoprofen and indomethacin [16,17].
We hypothesize that toxic aglycones released by re-activation of drug conjugates, such as diclofenac-acyl-glucuronide in the gut, impairs anastomotic integrity (Fig. 1). In the present study this is investigated by inhibiting β-glucuronidase in a validated rat model for diclofenac-induced anastomotic leakage [10].
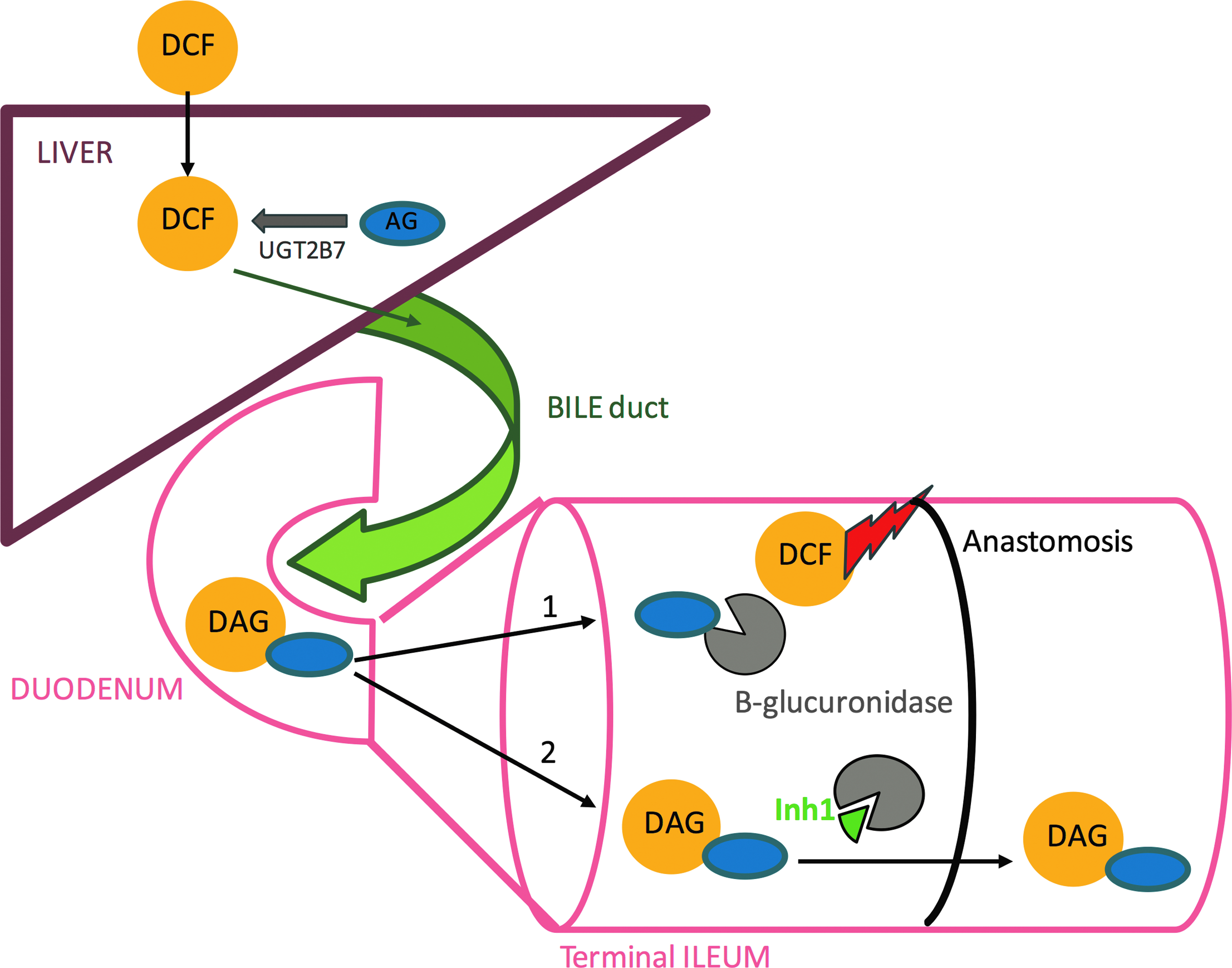
Following glucuronidation of DCF in the liver, DAG enters the gut through biliary excretion. In the gut (terminal ileum) DAG is either cleaved by bacterial glucuronidase, resulting in reactivation of the metabolite which is believed to injure the bowel wall and anastomosis (arrow 1). Or, inhibition of enzymatic hydrolysis by Inh-1 preserves the DAG metabolite which can be safely excreted through the feces (arrow 2). DCF = diclofenac; DAG = diclofenac-acyl-glucuronide; UGT2B7 = uridine diphosphate glucuronosyltransferase 2B7; AG = acyl-glucuronide (UDPGA, uridine diphosphate glucuronic acid); Inh1 = inhibitor 1.
Methods
Ethics
This experiment was done according to the EU Directive 2010/63/EU and European Federation of Laboratory Animal Science Associations guidelines, and was approved by the Animal Ethics Committee, and executed in the Central Animal Laboratory, of the Radboud university medical center (AEC-number 2013-200).
Animals and peri-operative care
Ninety adult male Wistar rats (weight 299 ± 24 g; Harlan, Horst, The Netherlands) were used. The rats were accustomed to laboratory conditions and housed two per cage at 22°C–23°C with a 12-h day cycle. They had free access to standard rodent chow (Ssniff Bio Services, Uden, The Netherlands) and water throughout the experiment. The cages were enriched with a rat retreat and sizzle nest and were placed randomly on the shelves. All animals were checked at least twice daily. Humane end points were defined; animals were killed if they showed signs of severe discomfort (e.g., weight loss >20% or severely reduced activity).
Materials
Diclofenac sodium injection fluid (Centrafarm, Etten-Leur, The Netherlands) dissolved in saline to 3.33 mg/mL was used for intra-muscular injections. The β-glucuronidase-inhibitor Inh1 was obtained as described previously [19]. It was first dissolved in dimethyl sulfoxide (DMSO; 20 mg/mL) and further in 0.5% methylcellulose (Sigma Aldrich, St. Louis, MO) in saline to a final concentration of 200 mcg/mL. Inh1 was administered 800 mcg/kg per day by oral gavage in two doses. Solution vehicle was methylcellulose (Sigma Aldrich, St. Louis, MO). Diclofenac sodium (Cayman Chemical Company Ann Arbor, MI) and 4-hydoxydiclofenac and 5-hydroxydiclofenac (Toronto Research Chemicals, North York, Canada), and diclofenac-acyl-β-glucuronide (LGC standards GMBH, Wesel, Germany) were used as standards for liquid chromatography mass spectrometry (LC-MS/MS) analyses and diclofenac-d4 (phenyl-d4-acetic) (JH Ritmeester, Nieuwegein, The Netherlands) was used as an internal standard of bile and plasma.
Study design
Animals were allocated randomly to two diclofenac groups and three non-diclofenac groups of 18 animals each by using www.randomization.com. Group DCF received diclofenac (1.5 mg/kg twice daily) intra-muscularly. The dose was based on the recommended daily dose in human beings (3 mg/kg per day) and on previous experiments [10]. Group DCF-Inh1 additionally received Inh1 (800 mcg/kg per day). In the non-diclofenac groups, animals received only Inh1 (800 mcg/kg per day) in group Inh1, vehicle (methylcellulose, 0.5 mL orally twice daily) in group Veh, or no solution in group Ctrl. All solutions were given orally twice daily from the day of surgery until sacrifice on day three. This period was used because diclofenac-induced leakage occurs mostly before day 3, when the anastomosis is at its weakest and postponing sacrifice would increase suffering [10,21].
Operative procedures
In random order, all animals were subjected to the following operation, which was done by experienced researchers (S.Y. or R.L.) blinded to group allocation. For analgesia, 0.02 mg/kg buprenorphine (Temgesic; Schering Plough, Houten, The Netherlands) was given subcutaneously every 12 h, starting approximately one hour before the operation until 48 h post-operatively. No antibiotic agents were given and animals were not fasted. Anesthesia was 5% (induction) or 2,5–3,5% (maintenance) with isoflurane (Abott, Hoofddrop, The Netherlands) in a 1:1 mixture of oxygen and pressurized air. Rats were shaved, iodized, draped with sterile covers, and then operated on through a 4–5 cm midline laparotomy using strict aseptic techniques under a microscope (Wild M650; Heerbrugg, Switzerland, at 10–16 × magnification). Body temperature was kept at 38°C with heating pad and lamp. One centimeter of ileum was resected at 15 cm proximal to the cecum. Subsequently an inverted anastomosis was made with a single layer of eight interrupted inverted (Lembert) Ethilon 8-0 sutures (Ethilon 8-0; Ethicon, Norderstedt, Germany). The abdominal wall was closed with a running suture (Vircryl 3-0; Ethicon, Norderstedt, Germany) and the skin with staples. Post-operatively 10 mL of 0.9% sodium chloride at 37°C was administered subcutaneously for rehydration, and subsequently rats were housed two per cage.
Outcome assessment
Animals were euthanized by cardiac or inferior vena cava puncture combined with cervical dislocation under general anesthesia with isoflurane. A re-laparotomy was done and the anastomosis was inspected macroscopically for signs of leakage by researchers blinded to the group randomization. The signs were graded according to an Anastomotic Complication Score (ACS): 0 for no abnormalities; 1 for small anastomotic abscesses; 2 for free pus or large abscesses; and 3 for fecal peritonitis or visible dehiscence (Fig. 2). Anastomotic leakage was defined as having a grade 1, 2, or 3 ACS. The final score was confirmed by agreement between the two researchers.
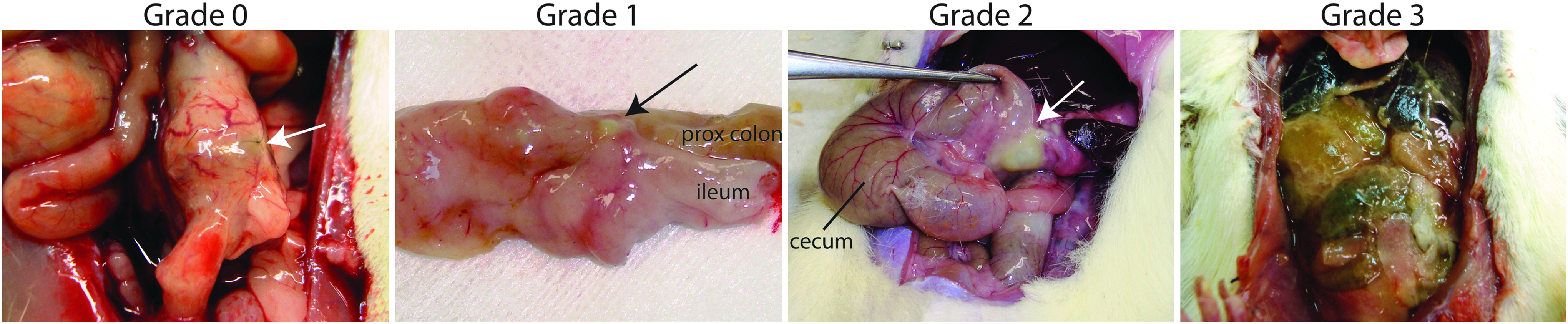
Anastomotic Complication Score examples. Grade 0 = no abnormalities; Grade 1 = minor abscess; Grade 2 = free pus; Grade 3 = generalized peritonitis or visible dehiscence.
Mechanical strength
All anastomoses were carefully resected and any scar tissue or adhesions covering the anastomosis were left in place. These segments were infused with 0.9% sodium chloride containing methylene blue at 2 mL/min to determine the strength of the weakest spot within the anastomoses. The segments were clamped 2 cm from the anastomosis. The maximum pressure (mm Hg) just before the sudden loss of pressure in case of failure was recorded as bursting pressure (BP).
To determine the maximal suture-holding capacity or scar strength, the segments were attached to a tensiometer (Single Column Testing Machine with 20N load cell, Zwick/Roell, Ulm, Germany) and pulled apart at 3 cm/min. The highest force measured before rupture was recorded as breaking strength (BS) and is noted as Newton.
Analysis of diclofenac plasma concentrations by LC-MS/MS
After removing proteins of the plasma samples diclofenac concentrations were determined with LC-MS/MS, using an Acquity UPLC (Waters, Milford, MA) coupled to a Xevo TQ-S (Waters) triple-quadrupole mass spectrometer. The compounds were separated on an HSS T3 analytical column (1.8 mcm; 100 × 2.1 mm; Acquity UPLC®, Waters, Ireland). As internal standard we used deuterated diclofenac: Diclofenac-d4 (phenyl-d4-acetic) (JH Ritmeester, Nieuwegein, The Netherlands). The elution gradient was as follows: 0 min, 40% B; 7–10 min, 80% B; and 11–14 min, 40% B. Solvent A consisted of 0.1% formic acid in water and Solvent B consisted of 0.1% formic acid in methanol. The column temperature was set at 40°C, and the flow rate was 300 mcL/min. The effluent from the UPLC was passed directly into the electrospray ion source. Positive electrospray ionization was achieved using nitrogen as a desolvation gas with ionization voltage at 1,000 V. The source temperature was set at 550°C and argon was used as collision gas. Detection of diclofenac and the internal standard was based on isolation of the protonated molecular ion, [M + H]+ and subsequent MS/MS fragmentations and a multi-reaction monitoring (MRM) were carried out. The following MRM transitions were used: for diclofenac m/z 295.9 (parent ion) to m/z 215.0 and 250.0 (both product ions), for diclofenac-d4 m/z 300.0 (parent ion) to m/z 219.0 and 254.0.
Sample size calculation and statistics
Sample size was determined with expected leak rates of 70%–80% in the positive control group (group DCF) and 0%–20% in the control group (group Ctrl) [10]. Group DCF-Inh1 was compared with group DCF. In the non-diclofenac cohort groups Inh1 and Veh were compared with group Ctrl. Anticipating analysis of leak rates with Fisher exact test and detection of an absolute difference of 50% in either direction, 18 animals per group were needed. A Mann-Whitney U test was used for the graded anastomotic complication score and an independent t-test for continuous variables (strength tests). In the non-diclofenac cohort, analysis of variance (ANOVA) and Kruskal-Wallis were used to compare the three groups. The spread of data is presented as standard deviation. P values <0.05 were considered statistically significant.
Results
Animal welfare and mortality
All animals experienced minor discomfort on the first post-operative day indicated by dirty eyes or nose and reduced activity. One animal in group DCF died on day two because of leakage and two animals in group DCF-Inh1 were killed on day two because of leakage-related illness (Table 1). Rats that died prematurely of leakage were included in analysis of leak rates and severity but were not used for strength tests. Four rats (three in group DCF; one in group DCF-Inh1) showed considerable signs of illness on day three. In the non-diclofenac groups three animals died prematurely of other causes: one peri-operative isoflurane overdose (group Ctrl), and two because of ileus and diarrhea without signs of leakage at autopsy (one in group Ctrl; one in group Veh). These rats were excluded from statistical analysis and were not used for strength tests. Weight loss from day 0 to day 3 was 10.0% ± 2.6% in group DCF, 9.6% ± 2.6% in group DCF-Inh1 (p > 0.05), 7.7% ± 2.7% in group Veh, 7.7% ± 2.5% in group Inh1 (p > 0.05), and 7.4% ± 2.7% in group Ctrl (p > 0.05).
Killed on day 2 because reaching humane end point.
Died on day 2 due to ileus and diarrhea without signs of leakage.
Died of peri-operative isoflurane overdose.
Weight loss is comparable among groups.
AL = anastomotic leakage; ACS = Anastomotic Complication Score (score 0, no abnormalities; score 1, minor abscess; score 2, free pus; score 3, generalized peritonitis or visible dehiscence); DCF = diclofenac; Inh1 = inhibitor 1; Veh = vehicle; Ctrl = SD = standard deviation.
Anastomotic leakage
Anastomotic leak rates were 89% in group DCF and 44% in group DCF-Inh1 (p = 0.006; Fig. 3A). Leak severity according to anastomotic complication scores was reduced by the inhibitor (p = 0.029; Fig. 3B). In the non-diclofenac groups leak rates were 25% in group Ctrl, 39% in group Inh1 (p = 0.477), and 24% in group Veh (p = 1.000). Leak severity was comparable for the non-diclofenac groups.

Anastomotic healing assessed by: (
Anastomotic strength
All bursts and breakings occurred at the anastomotic line. Mean burst pressure values and breaking strength were not statistically different between diclofenac groups (Figs. 3C and 2D).
Mean bursting pressure was 32 ± 27 mm Hg in group DCF and 42 ± 29 mm Hg in group DCF-Inh1 (p = 0.245; Fig. 3C). In the non-diclofenac cohort, bursting pressures were slightly higher than in the diclofenac groups but without substantial difference between groups (52 ± 14 mm Hg in group Veh, 43 ± 21 mm Hg in group Inh1, and 48 ± 23 mm Hg in group Ctrl; p = 0.329). Breaking strength (Fig. 3D) was 0.17 ± 0.09 N in group DCF, 0.16 ± 0.12 N in group DCF-Inh1 (p = 0.757); 0.23 ± 0.17 N in group Veh, 0.22 ± 0.10 N in group Inh1, and 0.25 ± 0.12 N in group Ctrl (p = 0.742).
LCMS/MS analysis of diclofenac concentrations in plasma
Plasma concentrations of diclofenac decreased 60 min after intra-muscular administration in all diclofenac groups (Fig. 4). There was no substantial difference between groups at any timepoint.
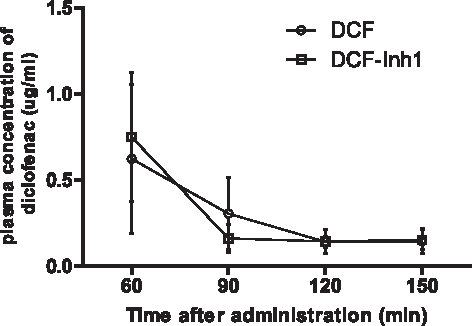
Liquid chromatography mass spectrometry (LC-MS) analysis showing no significant difference in plasma concentrations of diclofenac two hours after intramuscular administration.
Discussion
Oral administration of Inh1 reduced anastomotic leak rate and severity substantially in diclofenac-treated rats. In groups receiving Inh1 or vehicle, minor signs of anastomotic healing disturbance were observed.
The finding that administration of a glucuronidase inhibitor reduces signs of leakage suggests that, without inhibition, cleavage of diclofenac-acyl-glucuronide metabolites to diclofenac aglycones disturbs ileal anastomotic healing. To assess whether administration of Inh1 could lead to weaker systemic action by preventing re-uptake of diclofenac molecules, we determined plasma concentrations of diclofenac at different time points. These showed similar pattern as without inhibition making a systemic action unlikely [15,22]. The harmful effect of re-activated diclofenac metabolites is in line with other studies demonstrating that drug aglycones cause mucosal damage in the terminal ileum [18,19,23]. Findings also correspond with results of former anastomotic healing experiments, in which it was demonstrated that diverting or replacing bile, and thereby preventing the entrance of drug metabolites into the gut, reduces severity of diclofenac induced leakage (unpublished data).
In the present study, a certain amount of leakage (33%) still occurred despite Inh1 treatment. Several explanations are possible. First, diclofenac is excreted through bile in multiple forms, including unconjugated diclofenac [24,25]. This means that even if β-glucuronidase is blocked, other active diclofenac metabolites might reach and harm anastomotic tissue [26]. Second, inhibition of β-glucuronidase by Inh1 was insufficient. In contrast to previous studies in which a single high dose of diclofenac was given to mice, in the present study diclofenac was administered twice daily for three days [18]. This results in a longer exposure to drug metabolites. The amount of inhibitor we administered was increased accordingly, but may have been insufficient still. Efforts were made to administer higher doses of Inh1 (4000 mcg/kg day) but preparation of the highly concentrated solution was troublesome and included severe clumping. Third, the remaining leak rate in group DCF-Inh1 could theoretically be a result of counteraction caused by intrinsic toxicity of Inh1 as a relatively high leak rate was observed in the inhibitor-only group. However, it mostly concerned low grade healing disturbances without other remarkable signs of toxicity and previous toxicity studies have shown no adverse effects [19] Another plausible explanation for remaining leakage in group DCF-Inh1 is the pharmacologic action of diclofenac, which involves cyclo-oxygenase (COX)-1/2 inhibition. Whereas pharmacologic COX-1/2 inhibition is believed to be less relevant in NSAID induced-enteropathy, the associated inhibition of prostaglandin E synthesis may play a role by interfering with inflammatory and proliferative processes in the healing cascade [15,27,28].
The mechanism of topical damage and healing disturbance by NSAID molecules is believed to be a multi-stage process in which re-uptake of diclofenac aglycones initially causes mitochondrial injury and cell death [29,30]. Subsequently, activation of TLR4 on macrophages initiates an excessive inflammatory response [30–32]. This disturbs the macrophage-mediated balance of inflammatory and proliferative processes during wound healing. Excessive inflammation involves increased collagen breakdown and may thereby cause weak anastomotic scar tissue and leakage [33,34]. Alternative mechanisms by which hepatic clearance of diclofenac can cause bowel damage are the formation of more toxic bile acid micelles and an increase in harmful enteric gram-negative bacteria [14,15].
A valid and reproducible rat model was used to study the influence of Inh1 on clinically relevant anastomotic leakage. In contrast to clinic though, animals were not fasted and no prophylactic antibiotic agents were given, in accordance to previous studies with this model. Fasting is considered to cause major discomfort to rats and both fasting and antibiotic agents could disturb the mucosa and microbial glucuronidase activity and thereby the objective of this study.
In the control group absolute leak rate was more than 20%, but it only concerned minor signs of healing disturbance. It is believed that such disturbances would also be found in clinic if every anastomosis would be checked and clinical relevance of such disturbances is hard to predict. The vehicle methylcellulose can have a laxative effect and thereby influence bowel physiology. Although no diarrhea was observed, this may have slightly confounded findings because three grade 2 complications were noticed in the vehicle group.
The mechanical strength results show that bursting pressure corresponds only moderately to leakage signs and that much larger sample sizes would be needed to detect differences. In accordance with previous studies, breaking strength poorly correlated with leakage. Because leakage is a much more relevant outcome the additional value of strength test is arguable. To confirm previous Inh1 studies, we attempted to measure mucosal permeability and ulceration with immunohistochemistry to have supportive evidence for leak reduction. However, quantitative analysis was not possible because destruction by peritonitis and ileus did not reveal sufficient samples.
The detrimental effect of reactivated diclofenac metabolites in the gut, as suggested in the present study, is believed to be similarly relevant in human beings. In human beings, diclofenac metabolism also involves glucuronidation in the liver [24,35–37]. This, however, also depends on individual pharmacokinetics, because disposition of drugs that are predominantly eliminated via acylglucuronidation can vary among human beings [37]. Differences in drug metabolism may explain why NSAIDs have not been identified convincingly as a cause of leakage. It is possible that NSAIDs only harm anastomoses in a particular group of patients [38].
In the current study an anastomosis of the distal ileum was used to assess the effect of Inh1 because previous studies found that both diclofenac-induced enteropathy and diclofenac-induced leakage are most severe in this particular segment. However, this mechanism may also be relevant for colonic and colorectal anastomoses. Altered bowel content and physiology after partial or sub-total colectomy may lead to comparably high concentrations of diclofenac metabolites and bile salts, and thus comparably high risk [39].
In the current experiment Inh1 was used to evaluate the relevance of diclofenac-acyl-glucuronide reactivation in leakage pathophysiology and not as a potential therapeutic agent for preventing leakage in human beings. Although this does not exclude its therapeutic potential in certain situations, it is simply easier to avoid diclofenac use because alternative analgesics are available [40].
The present study suggests that re-activation of diclofenac metabolites in the gut leads to anastomotic healing disturbances. Administration of Inh1 to block this process reduces signs of leakage, but could not prevent a leak in all cases. In subsequent experiments a stronger effect could be aimed for by increasing frequency of Inh1 administration, instead of increasing Inh1 concentration.
In general, the present study contributes to the evidence that intraluminal compounds are relevant in leakage pathophysiology [41]. This means that in order to reduce the clinical burden of anastomotic leakage, more research should be done beyond the scope of known partially non-correctable risk factors and etiologies (e.g., ischemia). It should seek to clarify the role of potential harmful intra-luminal factors, which may also include specific bacterial virulence factors and some enteral nutrients [23,24,41].
Administration of glucuronidase inhibitor Inh1, aiming at preventing re-activation of diclofenac-acyl-glucuronid metabolites in the gut, reduces diclofenac-induced anastomotic leakage. This suggests a harmful effect of diclofenac metabolite reactivation on anastomotic healing. These findings improve our understanding of the pathogenesis of anastomotic leakage.
Footnotes
Acknowledgments
Research was partly financed by EFRO grant (2011-014237). A.P.B. was supported by T32DK007737. M.R. was supported by the US National Institutes of Health grants CA098468 and CA207416 (MRR).
Author Disclosure Statement
M.R. is co-founder of Symberix, Inc., a pharmaceutical company developing microbiome-targeted therapeutics. All other authors have no conflicts of interest concerning the current article.