
Abstract
Abstract
Background:
We evaluated the Surveillance of Surgical Site Infection (SSI), Auditing, and Feedback (SAF) effect on the rate of compliance with an SSI care bundle and measured its effectiveness in reducing the SSI rate.
Method:
A prospective cohort study from January 2014 to December 2016 was classified into three phases: pre-SAF, early-SAF, and late-SAF. Pre-operative baseline characteristics of 24,677 patients who underwent orthopedic, cardiovascular thoracic surgery (CTVS) or urologic operations were recorded. Univariable analyses of the SSI rates in the pre-SAF and post-SAF phases were performed. Percentage compliance and non-compliance with each care component were calculated. Correlation between reduction in the SSI rate and increase in compliance with the pre-operative, peri-operative, and post-operative care-bundle components was performed using the Spearman test.
Results:
There was a significant decrease in the SSI rate in orthopedic procedures that involved surgical implantation and in mitral valve/aortic valve (MVR/AVR) cardiac operations, with a relative risk (RR) ratio of 0.19 (95% confidence interval [CI] 0.12–0.31) and 0.08 (95% CI 0.03–0.22), respectively. The SSI rate was inversely correlated with the rate of compliance with pre-operative (r = -0.738; p = 0.037), peri-operative (r = - 0.802; p = 0.017), and post-operative (r = -0.762; p = 0.028) care bundles.
Conclusion:
Implementation of the Surveillance of SSI, Auditing, and Feedback bundle had a profound beneficial effect on the SSI rate, thereby reducing healthcare costs and improving patient quality of life.
S
Among those preventive measures is the “care-bundle” concept, developed by the Institute for Healthcare Improvement (IHI) USA in 2001. Many studies have reported the effectiveness of care bundles [7–9], and there now are evidence-based guidelines on the efficacy of the care-bundle approach in preventing SSI.
Promoting awareness of infection among surgical staff by developing an active surveillance system on SSI is an effective strategy for reducing SSI rates [10]. Further to implementation of a care bundle, auditing and feedback of the compliance rate is a major contributing factor to high-quality patient care, thereby reducing the SSI rate to a minimum [11, 12]. However, studies of multi-disciplinary teams involved in evaluating the effectiveness of a hospital surveillance system and monitoring the care-bundle compliance rate in reducing SSI are limited [13].
Our hospital baseline SSI rate is low, as we strictly follow and periodically update and implement all the best practice guidelines for their prevention [14–18]. A multi-disciplinary hospital infection control team constituted more than a decade ago ensures adherence to best practices. We took the view that our actions had to be aimed at reducing all healthcare-associated infections. Although we have been collecting our data for several years on a number of infections to map our progress, an effective surveillance system for SSI and an audit and feedback on care-bundle compliance was lacking. As a result, improper reporting of SSI cases, lack of awareness of SSI among surgical staffs, and incomplete and duplication of care-bundle compliance records frequently were observed. Hence, the main aim of the present study was to demonstrate the effectiveness of a surveillance system and to present the efficacy of audit and feedback on care-bundle compliance measurement in reducing SSIs associated with orthopedic, CTV, and urologic operations by comparing SSI rates in pre-SAF and post-SAF data.
Patients and Methods
Study design and setting
This was a prospective cohort study, conducted at a 300-bed (51-bed intensive care unit [ICU]) tertiary-care hospital totally free of cost with cardiology, CVTS (18-bed ICU), urology (13-bed ICU), ophthalmology (six-bed ICU), plastic surgery (six-bed ICU), orthopedics (eight-bed ICU), and gastroenterology departments offering free healthcare services to almost 100,000 patients annually.
The study was classified into three phases: (1) Pre-SAF phase, from January–December 2014; (2) early post-SAF phase, from January–December 2015; and (3) late post-SAF phase, from January–December 2016.
Data collection and definitions
All patients who underwent orthopedic, CTV, or urologic surgery from January 2014 to December 2016 were included in the study, and there were no exclusion criteria. Cases of SSIs were recorded according to the CDC criteria [14]. The following pre-operative characteristics of the patients were recorded: age, gender, surgery in the past year, hospitalization in the past year, exposure to antibiotics in the past three months, diabetes, hypertension, type of surgery (elective versus emergency), and classification of surgery.
Care-bundle components were developed based on following guidelines:
1. CDC and Prevention Guideline for the Prevention of Surgical Site Infection [14]; 2. Selection and administration of antibiotic prophylaxis within 60 minutes prior to incision was based on American Society of Health-System Pharmacists (ASHP) Guidelines [17]; and 3. Surgical incision care and maintaining normothermia based on National Institute for Health and Clinical Excellence (NICE) guidelines [16,18].
Pre-SAF phase (2014)
During the earliest phase, there was no systematic monitoring or recording of data. Cases of SSI were identified and reported during patient's revisit by clinicians and were treated empirically according to hospital antibiotic policy guidelines and then escalate or de-escalate according to the culture report.
A multidisciplinary team, encompassing surgical, anesthesia, nursing, and clerical staff, was involved in the implementation of the SSI care bundle across all the ICUs and wards from January 2014 according to the CDC guidelines, in addition to compliance with hand hygiene [14]. Education and training were provided to all the identified multi-disciplinary groups by the hospital infection control (HIC) team. Instruction manuals and checklists on the SSI care bundle were provided, and posters describing infection control practices, including appropriate handwashing steps, were displayed in all ICUs and wards. Readiness, recognition, prevention and response, reporting, and system learning of care-bundle components before any surgical procedure were explained. Enforcement responsibilities were delegated to individual members/teams involved in the care bundle.
SAF approach (2015 and 2016): Hospital surveillance system
Stage 1—Data collection
For every patient, our surgical team collected data such as age, gender, surgery in the past year, hospitalization in the past year, prior exposure to antibiotics, pre-operative and post-operative hospital stay, co-morbidities, duration of surgery, and type of surgery classified as clean, clean–contaminated, or contaminated according to the CDC guidelines. This information was entered on a standard form and filed with the patient's medical records.
Stage 2—Follow-up of patients
This information was uploaded into our electronic hospital information system (eHIS) by our HIC team clerical staff for follow- up by an HIC practitioner. All surgical patients were followed up for 30 days, for one year if there was an implant.
Stage 3—Confirming SSI cases
Post-operative instructions were given to patients on managing pain, incision care, hand hygiene, diet, and other activities by surgeons at the time of discharge; and a revisit was scheduled. Surgeons were responsible for diagnosing SSI based on CDC guidelines. The surgeon's diagnosis was confirmed by an HIC practitioner based on the patient's clinical history and microbiology culture report.
Stage 4—Root Cause Analysis (RCA)
For all the confirmed SSI cases, surgeons performed root cause analysis (RCA) based on various factors such as the patient's current medical condition; peri-operative, intra-operative, and post-operative care; duration of surgery; and antibiotic prophylaxis to identify contributing factors. Preventive measures were taken to control the spread of infection. Detailed monthly reports on the SSI rate were presented to HIC team executives, and a meeting was conducted every month to discuss hospital SSI and appropriate direct preventive measures.
Auditing and feedback on care-bundle compliance
Stage 5—Audit Tool
The audit tool was developed by our hospital IT professionals based on the Infection Prevention and Control Assessment Tool designed by the CDC [19, 20]. The aim was to assess SSI care-bundle practices and determine the area(s) requiring quality improvement (Supplementary Fig. 1).
Stage 6—Compliance and feedback
Care-bundle checklists downloaded from the CDC website [19] were filled out for each patient and included in the audit. The percentage compliance with each care-bundle component was calculated by the HIC team, and regular feedback from audit results was provided to wards and ICUs regarding adherence to elements to improve surgical care. Feedback on noncompliance with any of the components was given to the surgical team during the department meeting conducted weekly in order to raise awareness of the significance of the particular bundle component.
Further to this research, surveys were conducted periodically to evaluate staff knowledge of care-bundle implementation guidelines. Measurements by the All or None (AON) approach, as defined by IHI [7], were included in the audit (Supplementary Fig. 1).
Statistical analyses
Statistics were analyzed using SPSS version 23.0 (SPSS, Inc., Chicago, IL). Categorical variables were expressed as percentage and frequencies and continuous variables as mean and standard deviation (SD). The overall SSI rate and the SSI rate specific to operations in orthopedics, CTVS, and urology were calculated as the number of cases of SSI per 100 procedures. Comparisons between the pre-SAF and post-SAF phases were performed using the χ2 test, and the relative risk (RR) ratio and 95% confidence interval (95% CI) were calculated. Percentages of care-bundle compliance and non-compliance in relation to combinations of care bundles were calculated. Changes in SSI rate and bundle compliance were assessed using monthly/quarterly data throughout the study period, and correlation between the SSI rate and bundle compliance was assessed using the Spearman rank test. An ITS analysis of SSI rate calculated by the autoregressive integrated moving average (ARIMA) model and automating time series forecasting was performed using the expert modeler tool in SPSS software. All statistical tests were two-tailed and evaluated at a <0.05 level of significance.
Results
A review of cumulative SSI data from 2014 to 2016 revealed a 0.4% relative reduction. During the study period, a total of 32,014 patients underwent surgery, of whom 204 developed an SSI. Out of 32,014 operations, 10,626 were performed during the pre-SAF phase and 21,388 in the post-phase. The baseline characteristics of the patients are presented in Table 1.
SAF = surveillance, auditing, and feedback; SD = standard deviation.
Operations and SSI rate
Table 2 presents analyses of the types of all major operations performed. A total of 5,322 orthopedic procedures, 2,950 cardiac operations, and 16,405 urologic procedures were performed.
No. of infected patients/total no. of operations × 100.
CI = confidence interval; CTVS = cardiovascular thoracic surgery; OF – Open fracture type I, II and III (based on Gustilo open fracture classification); RR = relative risk.
A significant reduction in the SSI rate was observed for overall orthopedic operations (p < 0.0001; RR 0.36; 95% CI 0.24–0.52]). During the pre-SAF phase, external/internal fixation of implants (which accounted for 27.6% of all orthopedics procedures) had the highest SSI rate (10.0%). A statistically significant decline in the SSI rate for this type of operation was achieved post-SAF (1.3%; p < 0.0001 RR 0.19; 95% CI 0.12–0.31). Further, the SSI rate for CTVS operations declined from 2.7% to 1.8% during the study period (p < 0.04; RR 0.59; 95% CI 0.35–0.99). In particular, a statistically significant reduction in the SSI rate was seen for cardiac valve replacement procedures (p < 0.0001; RR 0.08; 95% CI 0.03–0.22). The SSI rate for urologic surgery involving either the upper or the lower urinary tract declined from 0.2% to 0.1%, although this change was not statistically significant.
Figure 1 presents the SSI rate reported by month. For ITS analysis, the ARIMA (1, 1,0) served as the best fit model, with a stationary R2 value of 0.537, and the Ljung-Box statistic (Q 13.6, DF 17; p = 0.69) indicated statistically non-significant autocorrelations with time (residuals). Time series forecasting predicts an SSI rate of 0.44 for the subsequent year (2017) with a 1.23 95% upper conference limit and a −0.35 95% lower conference limit. A model summary of ARIMA and forecasting is presented in Supplementary Appendix 1.

Incidence of surgical site infection (SSI) during study period. Interrupted time series plot of monthly SSI rate with autoregressive integrated moving average (1, 1,0), UCL = 95% upper confidence limit, LCL = 95% lower confidence limit, and forecasting of SSI.
Audit results on bundle compliance
Figure 2 presents audit results on compliance with overall and pre-operative care (includes skin preparation of surgical site, antibiotic prophylaxis, and screening for methicillin-resistant Staphylococcus aureus [MRSA]), peri-operative care (includes maintaining normothermia and glycemic concentration), and post-operative care (includes incision care) components per annual quarter starting at 92.7% and increasing to 99% by the end of 2016.

Percentage compliance with care bundle after surveillance, auditing, and feedback phase. Percentage compliance with pre-operative care (skin preparation of surgical site, antibiotic prophylaxis, and methicillin-resistant Staphylococcus aureus screening) peri-operative care (maintaining normothermia and glycemic concentration), and post-operative care (surgical site care) components and overall compliance at quarterly intervals during early (2015) and late (2016) implementation phases.
Compliance with all eight individual care components is presented in Table 3. The percentage of AON increased from 88% during early implementation to 94.7% during late implementation. Zero percent noncompliance with all care components was observed during the entire study period. The average percentage of only partial adherence to care components was reduced from 1.9% in 2015 to 0.6% in 2016.
Compliance with all care components.
MRSA = methicillin-resistant Staphylococcus aureus; SAF = surveillance, auditing, and feedback.
Figure 3 also presents the correlation between the SSI rate and bundle compliance post-SAF. The overall SSI rate was inversely correlated with compliance for pre-operative (r = −0.738; p = 0.037), peri-operative (r = −0.802; p = 0.017), and post-operative (r = −0.762; p = 0.028) care. Increased compliance with the care bundles therefore had a profound effect on the reduction of SSI.
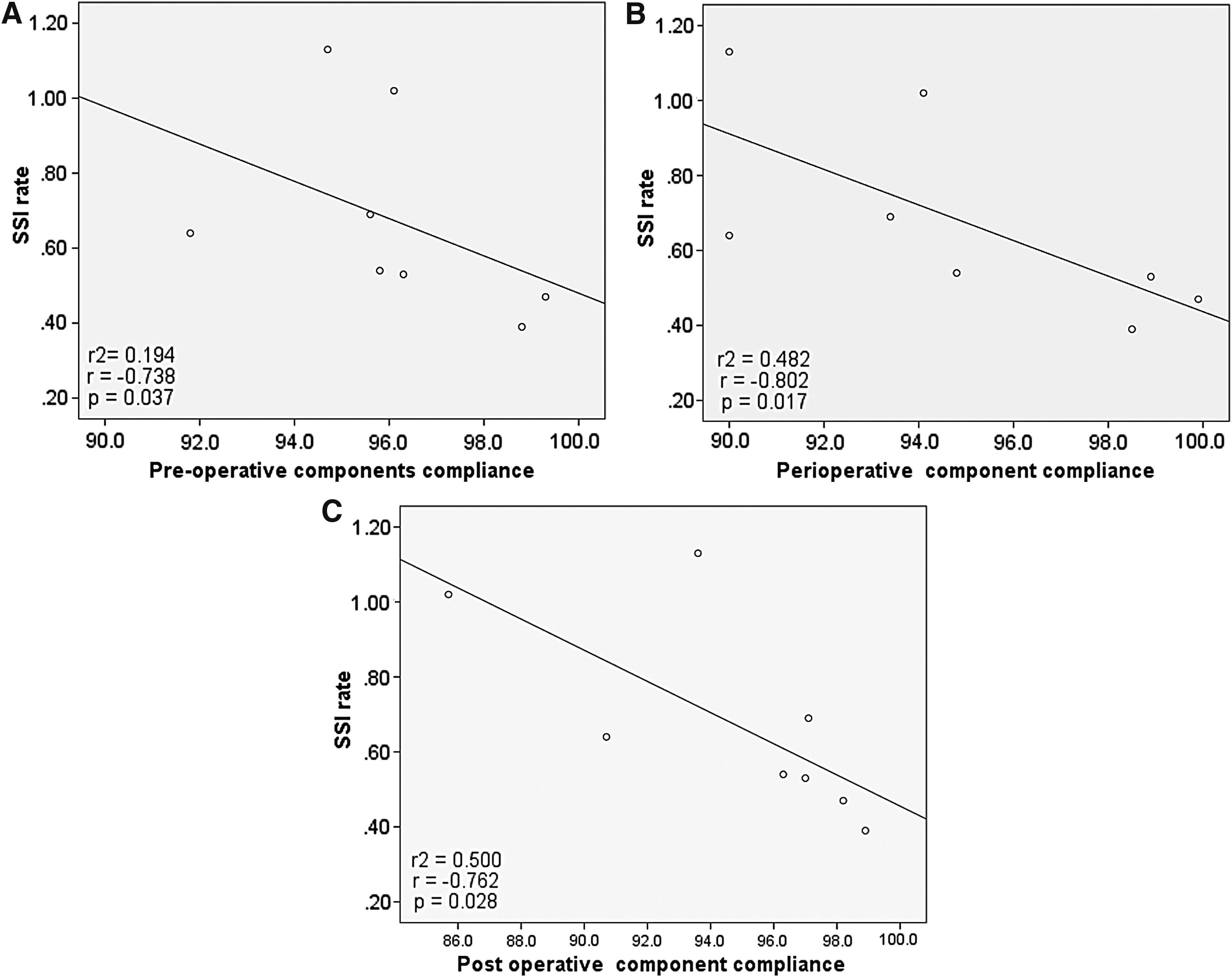
Correlation between SSI rate and percentage compliance after surveillance, auditing, and feedback phase.
Although cefazolin was used as routine surgical prophylactic antibiotic, there was a problem with extended-spectrum β-lactam-producing E.coli cases in the year 2014 in urology, which accounted for 69.2% of the overall 27.5%. Similarly, orthopedics contributed 70% to 12.7% of the overall MRSA cases. Hence, in view of the patient's clinical history, fluoroquinolones were used as antibiotic prophylaxis for patients undergoing specific urologic procedures such as percutaneous nephrolithotomy. In orthopedics, the MRSA bundle was implemented, and vancomycin was administered to appropriate patients [21, 22].
Discussion
This study shows that surveillance for SSI and audit and feedback on care-bundle compliance can significantly reduce the SSI rate. Our hospital infection control committee was constituted more than a decade ago, and all the best-practice guidelines are updated periodically and implemented. However, monitoring and recording of adherence to these best practices were not in place. Importantly, our baseline SSI rate (Table 2) meets the benchmark set by International Nosocomial Infection Control Consortium (INICC) for developing countries [24]. However, our higher-order goal was to provide high-impact intervention and improve the efficiency of patient care. Hence, by developing a surveillance system and audit tools, we investigated the effect of the SAF approach to prevent SSI and improve compliance with individual SSI-bundle components. In concordance with the proposal by Rioux et al. [10] regarding SAF approach implementation to reduce SSI, our study shows a significant decrease in the SSI rate, from 0.8 % (pre-SAF) to 0.2% (post-SAF) (see Fig. 1). It is noteworthy that the reduction in the SSI rate was achieved in spite of no concomitant decrease in the number of operations performed during the study period. In fact, there were 9% and 15% increases in procedures involving internal and external fixation of implants and MVR/AVR, respectively. In spite of this increase, a statistically significant reduction in SSI was achieved for these procedures. Interestingly, a zero SSI rate was achieved for arthroscopy, stent removal, and double-J stenting in the late post -SAF phase.
Few studies have discussed the effect of audit and feedback on compliance rates for individual care components [10,24]. Pre-operative antibiotic prophylaxis was the key component of the care bundles in the majority of the studies reviewed by Gillespie et al. [13]. Antibiotic prophylaxis was chosen according to international surgical prophylaxis guidelines and, when necessary, based on our hospital half-yearly cumulative antibiograms. In our study, the compliance rate for surgical antibiotic prophylaxis (care component 4) was highest throughout the study period. This is in concordance with a study by Crolla et al. [25], where the highest compliance rate was seen for antibiotic prophylaxis. A significant compliance percentage was observed for individual care components and full adherence with some components (Table 3). During the early post-implementation phase (2015), we had a >95% compliance rate for care components 4 and 8. During the late post-implementation phase, >95% compliance was observed for all of the care components. Stringent compliance monitoring by our HIC team and the AON-bundle compliance approach resulted in a decrease in the percentage of partial adherence from 2.6% to 1.6%. We observed that the increase in the percentage compliance with bundle care was significantly associated with a reduction in the SSI rate (see Figs. 2 and 3).
It is important to note that our results are not in agreement with many published studies such as those of Crolla et al. [25], Zywot et al. [26], and Van der Slegt [27] as our SSI rates were low for the operations included in our study, This difference in results may be attributable to our institution's higher-order treatment mission and goals, with a specific emphasis on a clean healthcare environment, research, and knowledge sharing by our multidisciplinary international experts serving as visiting healthcare professionals, periodically updating guidelines on infection control and antibiotic policy and stewardship.
Compliance with hand hygiene and other infection control aspects in healthcare represents a complex, socially entrenched, and ritualistic behavior [28]. As our hospital is a part of a spiritual organization, the medical and paramedical staffs in various cadres understand patient care and discharge their duties with great responsibility and accountability. This culture and team dynamics has helped our healthcare workers adhere to protocol-driven guidelines and infection control behavioral aspects.
We also observed that, although there was a 50% reduction in the number of MRSA isolates, there was not a significant reduction in infections with this organism in spite of implementation of the “pre-operative screening for MRSA” care bundle (Table 3). These organisms were isolated predominantly (85%) from the department of orthopedics during the post-implementation phase, and all the affected patients had a history of hospitalizations and antibiotic exposure. Strict infection control of incision site prior to surgery and adherence to infection control measures with specific reference to contact precautions have been recommended to the department of orthopedics.
Our study has many limitations. The main one is that we have not included the care component “discontinuing prophylactic antibiotics within 24 hours of completion of surgery.” Compliance with the above-mentioned care-bundle results in reduction of drug resistance. Although this care component was followed as a surgical site infection prevention measure, it was not recorded under the care-bundle components. Another limitation is the average age of the population of patients under study. This is secondary to the fact that our hospital attends to 100,000 outpatients annually, and approximately 80% of them are critically ill requiring surgery. Providing surgical care to all these patients is not truly feasible; a priority for surgical intervention was given on the basis of the impact of surgery on the quality of the patient's life and the patient's emergency and need for surgery. Hence, it happened that our average age was 48 years during the study period.
In conclusion, this study indicates that surveillance of the SSI rate created sufficient awareness among surgical staff, and audit and feedback on care-bundle compliance led to a significant increase in the compliance rate. The SAF approach was associated with a significant reduction in the SSI rate to a dramatically lower number and provided high-impact intervention, thereby improving surgical patient care. Furthermore, it resulted in reduced use of healthcare resources and avoided duplication of care bundles.
Footnotes
Acknowledgment
We acknowledge the tremendous efforts of our HIC team members in implementing the care bundle at our institute and the ICU and ward nurses for their dedication. We are grateful to Mr. Soundararajan Kannan and Mr. Inamanamelluri Venkata Ramachandra, Department of Information Technology, SSSIHMSPG, for providing access to the anonymized hospital metadata.
Author Disclosure Statement
No competing financial interests exist. This research project received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.