
Abstract
Abstract
Background:
Sepsis is a global healthcare issue and continues to be the leading cause of death from infection. Early recognition and diagnosis of sepsis is required to prevent the transition into septic shock, which is associated with a mortality rate of 40% or more.
Discussion:
New definitions for sepsis and septic shock (Third International Consensus Definitions for Sepsis and Septic Shock [Sepsis-3]) have been developed. A new screening tool for sepsis (quick Sequential Organ Failure Assessment [qSOFA]) has been proposed to predict the likelihood of poor outcome in out-of-intensive care unit (ICU) patients with clinical suspicion of sepsis. The Surviving Sepsis Campaign Guidelines were recently updated and include greater evidence-based recommendations for treatment of sepsis in attempts to reduce sepsis-associated mortality. This review discusses the new Sepsis-3 definitions and guidelines.
S
Sepsis-3: New Definitions
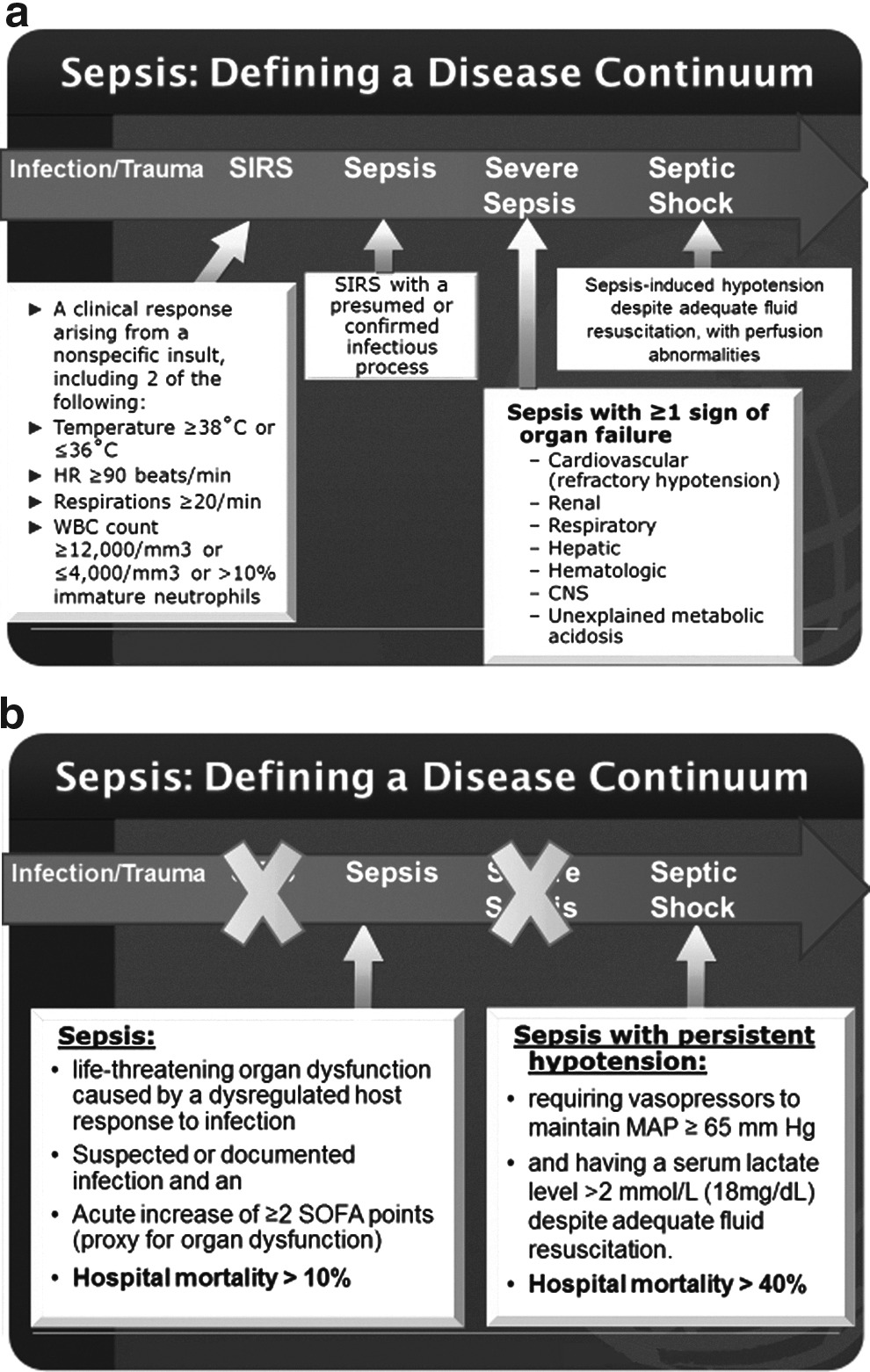
Initial sepsis definitions were developed at a 1991 consensus conference [2] with a subsequent update in the sepsis definitions in 2001 that simply expanded the list of signs and symptoms of sepsis to reflect clinical bedside experience [3]. The initial sepsis definitions included sepsis (systemic inflammatory response syndrome [SIRS] and suspected infection), severe sepsis (sepsis and organ dysfunction) and septic shock (sepsis and hypotension despite adequate fluid resuscitation; Fig. 1).
Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3): (
An international task force with 19 participants was convened by the Society of Critical Care Medicine (SCCM) and the European Society of Intensive Care Medicine (ESICM) to revise the current sepsis and septic shock definitions. Using an expert Delphi consensus process, this group developed the new Sepsis-3 definitions [4,5]. They moved away from the association between infection and inflammation and completely abandoned SIRS criteria.
Sepsis is defined as life-threatening organ dysfunction caused by a dysregulated host response to infection. The clinical criteria for sepsis include suspected or documented infection and an acute increase of two or more Sequential Organ Failure Assessment (SOFA) points as a proxy for organ dysfunction. Septic shock is defined as a subset of sepsis in which underlying circulatory and cellular/metabolic abnormalities are profound enough to increase mortality substantially. Septic shock is defined by the clinical criteria of sepsis and vasopressor therapy needed to elevate mean arterial pressure ≥65 mm Hg and lactate >2 mmol/L (18 mg/dL) despite adequate fluid resuscitation (Fig. 1).
The mortality rate associated with the new septic shock definition is high (40%) compared with a mortality rate of 10% with the new sepsis definition. A systematic review identified 44 studies reporting septic shock outcomes, and the Delphi process identified hypotension, lactate concentration, and vasopressor therapy as clinical criteria to identify patients with septic shock. Based on these parameters, specific patient groups with or without these clinical criteria were developed, and their prevalence and associated mortality rates were examined in the SSC database (Table 1). The group requiring vasopressors to maintain mean arterial pressure 65 mm Hg or greater and a lactate concentration >2 mmol/L (18 mg/dL) after fluid resuscitation (group 1) had a higher mortality (42.3%) in risk-adjusted comparisons with the other five groups. This analysis led to the new Sepsis-3 septic shock definition [6]. It should also be noted, however, that patients who met the Sepsis-2 criteria for septic shock (group 2) with hypotension, requiring vasopressors, but without lactate elevation, also had a high mortality rate of 30.1%. The higher mortality rate associated with this new definition of septic shock has important implications for trial design in septic shock and may allow decreased sample size for future septic shock trials [7].
Meets criteria for new Sepsis-3 septic shock definition.
Meets criteria for old Sepsis-2 septic shock definition.
Data compiled from: Shankar-Hari M, Phillips GS, Levey ML, et al. Developing a new definition and assessing new clinical criteria for septic shock. For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016;315:775–787.
Sepsis-3 = Third International Consensus Definitions for Sepsis and Septic Shock.
Controversy remains regarding the inclusion of lactate in the Sepsis-3 septic shock definition and the exact lactate measurement (> 2 mmol/L) used in the definition. One study analyzed a prospective cohort of ICU patients with sepsis (n = 632) and documented that patients meeting the Sepsis-3 definition of septic shock had a higher mortality than patients meeting the Sepsis-2 definition (38.9% vs. 34.0%), but only lactate values ≥6 mmol/L were associated with increased ICU mortality [8]. Others report concern that lactate is a sensitive but not specific indicator of cellular or metabolic stress rather than “shock.”
SIRS versus SOFA and qSOFA in Sepsis
A retrospective analysis of the Australian and New Zealand Intensive Care Society (ANZICS) database (2000–2013) included 109,663 patients with infection and organ failure to validate the severe sepsis definition [9]. It was reported that 87.9% of patients had two or more SIRS criteria but 12.1% did not. Using SIRS alone missed one in eight patients with severe sepsis. The study confirmed that each additional SIRS criteria increased mortality by 13% in a linear manner without a transitional increase when two SIRS criteria were met. They concluded that the use of two or more SIRS criteria alone lacked both sensitivity and specificity for diagnosing severe sepsis in ICU patients.
The subsequent analysis of clinical criteria for the new Sepsis-3 definitions compared SIRS criteria, the SOFA score, the Logistic Organ Dysfunction System (LODS) score, and the quick SOFA (qSOFA) score (range, 0–3 points, with one point each for systolic hypotension [≤ 100 mm Hg], tachypnea [≥ 22/min], or altered mentation). The SOFA score (Table 2) is widely used in critical care research, but is not a common clinical tool used at the bedside in the ICU [10].
Fio2 = fraction of inspired oxygen; MAP = mean arterial pressure; Pao2 = partial pressure of oxygen.
Adapted from Vincent et al. [10].
Catecholamine doses are given as μg/kg/min for at least 1 hour.
Glasgow coma scale scores range from 3–15; higher score indicates better neurological function.
The qSOFA score (Fig. 2) was developed as a simple screening tool to identify patients with possible sepsis. A qSOFA score of two or more identifies a patient at greater risk of poor outcome. Among non-ICU encounters in patients with suspected infection, qSOFA had a predictive validity for in-hospital mortality (area under the receiver operating characteristic curve [AUROC] 0.81) that was greater than the full SOFA score (AUROC 0.79) and SIRS (AUROC 0.76; Table 3). In contrast, however, in the ICU, the predictive validity for in-hospital mortality was lower for qSOFA (AUROC 0.66) and SIRS (AUROC 0.64) compared with the full SOFA score (AUROC 0.74) [5].

Quick Sequential Organ Failure Assessment (qSOFA) score for sepsis.
AUROC = area under the receiver operating curve; SIRS = systemic inflammatory response syndrome; SOFA = Sequential Organ Failure Assessment score; qSOFA = quick Sequential Organ Failure Assessment score.
The use of the SOFA score in the Sepsis-3 definition is challenging, because SOFA is a complicated score that is not calculated routinely in ICUs at the bedside. Systemic inflammatory response syndrome and qSOFA are scores that are easily calculated at the bedside for use in the screening of patients with possible sepsis. A retrospective cohort analysis of the ANZICS database that was used to assess SIRS in the severe sepsis definition was also used to compare the prognostic accuracy of the SOFA score, SIRS criteria, and qSOFA score for in-hospital mortality among adults with suspected infection admitted to the ICU. The SOFA score increased by two or more points in 90.1%; 86.7% had SIRS score of two or more, and 54.4% had a qSOFA score of two or more. An increase in SOFA score of two or more had greater prognostic accuracy for in-hospital mortality (AUROC 0.753) than SIRS (AUROC 0.589) or the qSOFA score (AUROC 0.607) [11].
Interestingly, qSOFA failed validation in a study of 30,677 patients with suspected infection from the emergency department and ward at the University of Chicago. Systemic inflammatory response syndrome, qSOFA, Modified Early Warning Score (MEWS), and National Early Warning Score (NEWS; Table 4) were compared. Using the highest non-ICU score of patients, two or more SIRS had a sensitivity of 91% and specificity of 13% for the composite outcome (death or ICU transfer) compared with 54% and 67% for qSOFA of two or more, 59% and 70% for MEWS of five or more, and 67% and 66% for NEWS of eight or more, respectively. The authors concluded that the qSOFA score should not replace general early warning scores when risk-stratifying patients with suspected infection [12].
The NEWS initiative flowed from the Royal College of Physicians’ NEWSDIG, and was jointly developed and funded in collaboration with the Royal College of Physicians, Royal College of Nursing, National Outreach Forum and NHS Training for Innovation.
In contrast, an international prospective cohort study from Europe included 879 patients in the emergency department with suspected infection and examined qSOFA as a mortality predictor. The overall in-hospital mortality was low (8%). The qSOFA performed better than SIRS and SOFA in prediction of in-hospital mortality (AUROC 0.8 qSOFA vs. 0.77 SOFA and 0.65 SIRS). Both qSOFA and SOFA had lower sensitivity (qSOFA 70%, SOFA 73% vs. SIRS 93%), and SIRS had lower specificity (qSOFA 79%, SOFA 70%, SIRS 27%) [13]. The use of qSOFA versus SIRS score for a sepsis screen actually depends on whether you desire increased sensitivity or specificity.
There is still controversy regarding the new Sepsis-3 definitions [14–16]. Some organizations have not endorsed the new Sepsis-3 definitions, including the American College of Chest Physicians [17], the Infectious Disease Society of America, the Latin American Sepsis Institute [18], American College of Emergency Physicians, none of the emergency medicine societies, and none of the hospital medicine societies. Additional prospective validation of the new Sepsis-3 definitions is clearly warranted.
SSC Guidelines
The SSC guidelines for the management of severe sepsis and septic shock were first published in 2004 [19] with an update in 2008 [20] and 2012 [21]. The overall goal of the SSC was to reduce mortality from severe sepsis and septic shock. Active participation in the SSC was associated with increased guideline adherence and reductions in sepsis-related mortality [22]. Adherence to the SSC guidelines was promoted via the use of SSC bundles, which included elements to be completed in a specific timeframe after the diagnosis of sepsis.
SSC bundles
The SSC bundles have changed during the SSC guideline updates (Table 5). The differences between the 2008 and 2012 bundles included an increase in fluid resuscitation recommended for sepsis-induced tissue hypoperfusion (20 mL/kg crystalloid in 2008; 30 mL/kg in 2012 for treatment of hypotension or elevated lactate) and discontinuation of the 2008 sepsis management bundle (steroids, activated protein C, glycemic control, and low plateau pressures in mechanically ventilated patients).
A global, prospective, observational quality improvement study of compliance with the 2012 SSC bundles in patients with severe sepsis or septic shock included 1,794 patients from 62 countries, and documented that overall compliance was low, at only 19% for the three-hour bundle, and 36% for the six-hour bundle. However, SSC bundle compliance was associated with a 40% reduction in the odds of dying in hospital with the three-hour bundle and 36% for the six-hour bundle [23].
The most recent guideline update was published in 2016 [24] and includes new three-hour and six-hour SSC bundles (Table 6). The most recent SSC bundles focus on early antibiotic treatment and fluid resuscitation to be initiated within three hours. Early identification of patients with sepsis, early intravenous fluid resuscitation, and early intravenous antibiotic administration are the mainstay of sepsis management.
From: www.survivingsepsis.org
Consistent in all of the SSC bundles is the recommendation for antibiotic administration within one hour of diagnosis of sepsis. In a study of 28,150 patients with severe sepsis and septic shock, in-hospital mortality was 19.7%, and delay in the first antibiotic administration was associated with increased risk of death [25].
The major change from the 2012 SSC bundle is the removal of early goal-directed therapy recommendations (resuscitation targets central venous pressure [CVP] ≥8, central venous oxygen saturation [ScVO2] ≥ 70%, and normalization of lactate) in the six-hour SSC bundle. The 2016 SSC bundle recommends serial re-assessment of volume status and tissue perfusion with dynamic assessments of fluid responsiveness including physical examination to evaluate for hypoperfusion, bedside cardiovascular ultrasound, passive leg elevation, or fluid challenge.
The new SSC guidelines 2016 also recognize that we are in an era of “personalized” medicine and “one size does not fit all.” Therefore, the SSC bundle recommendations are not meant to be implemented without interval re-evaluation. For example, in a patient with sepsis with severe hypoxemia and acute respiratory distress syndrome or heart failure, fluid resuscitation of 30 mL/kg may not be appropriate and vasopressor or cardiotonic medications may be indicated to optimize tissue perfusion [26]. We are beginning to determine risk factors for patients who are not fluid responsive in septic shock (heart failure, hypothermia, immunocompromised, hyperlactemia, and coagulopathy) and may need to investigate alternate therapies in this population with sepsis with a phenotype for refractory hypotension [27].
SSC Guidelines 2016 Changes
A number of evidence-based changes in recommendations are evident in the 2016 SSC Guidelines (Table 7). The most substantial change in the new guidelines is that for initial resuscitation, protocolized care with early goal-directed therapy is no longer recommended. There are no changes in recommendations regarding vasopressors (norepinephrine first-choice vasopressor, add vasopressin or epinephrine if not at target mean arterial pressure) and steroids (consider for patients with septic shock refractory to adequate fluids and vasopressors). The new guidelines include a number of strong recommendations with moderate or high-quality evidence (Table 8). A few of these changes are highlighted below.
CVP = central venous pressure; ScVO2 = central venous oxygen saturation; MAP = mean arterial pressure; TTE = transthoracic echocardiography; IV = intravenous.
ARDS = acute respiratory distress syndrome; HFOV = high-frequency oscillatory ventilation; VTE = venous thromboembolism; GI = gastrointestinal.
Mean arterial pressure target
The new guidelines continue to recommend a target mean arterial pressure of 65 mm Hg over higher targets. A multi-center open-label trial of 776 patients with septic shock confirmed that resuscitation with a higher mean arterial pressure target of 80–85 mm Hg had no impact on 28-day or 90-day mortality [28]. But the new guidelines now also recommend: “When a better understanding of any patient's condition is obtained, this target should be individualized to the pertaining circumstances.” This again reflects a move toward personalized card of the patient with sepsis in the ICU.
Early goal-directed therapy
A single-center randomized trial of early goal-directed therapy (six-hour resuscitation protocol to achieve specific blood pressure, CVP, ScVO2, and hemoglobin, compared with usual care in patients with septic shock reported a reduction in hospital mortality from 46.5% to 30.5% [29]. Early goal-directed therapy was recommended in all previous SSC guidelines, but has been removed from the 2016 guidelines.
Three multi-center randomized controlled clinical trials (Protocolized Care for Early Septic Shock, Australasian Resuscitation in Sepsis Evaluation, and Protocolised Management in Sepsis) showed no benefit to early goal-directed therapy in the treatment of septic shock. Protocolized Care for Early Septic Shock (ProCESS) [30] was conducted in the United States, Australasian Resuscitation in Sepsis Evaluation (ARISE) [31] was conducted in Australia and New Zealand, and Protocolised Management in Sepsis (ProMISE) [32] was conducted in the United Kingdom. A trial-level meta-analysis confirmed no overall benefit from early goal-directed therapy in septic shock [33]. A patient-level meta-analysis of the three trials included 3,723 patients, and 90-day mortality was similar for early goal-directed therapy (24.9%) and usual care (25.4%). A sub-group analysis of patients with worse shock (higher lactate, combined hypotension and high lactate, or higher predicted risk of death) also confirmed that early goal-directed therapy was not associated with improved survival. Early goal-directed therapy was associated with increased ICU days, cardiovascular support, and higher costs [34].
Blood product transfusion
The 2016 SSC guidelines includes a significant change in the recommendation for red blood cell (RBC) transfusion: “We recommend that RBC transfusion occur only when hemoglobin concentration decreases to <7 g/dL in adults in the absence of extenuating circumstances, such as myocardial ischemia, severe hypoxemia, or acute hemorrhage (strong recommendation, high quality of evidence).” This is different than the 2012 guidelines that recommended early goal-directed therapy with a target hemoglobin of 10 g/dL in the early resuscitation of patients with sepsis. This significant change is based on the results of the Transfusion Requirements in Septic Shock (TRISS) trial that compared a transfusion threshold of 7 versus 9 g/dL in patients with septic shock after ICU admission. No differences in 90-day mortality, ischemic events, or use of life support was identified and significantly fewer RBC transfusions were administered in the 7 g/dL threshold group [35]. A sub-group analysis of the TRISS trial also observed no survival benefit in any sub-groups of transfusion with a higher hemoglobin threshold [36]. The three early goal-directed therapy trials reviewed above also provide additional indirect evidence that targeting a hemoglobin concentration of 10 g/dL in the early goal-directed therapy protocol group was not associated with improved outcomes.
Source control
Two new best practice statements are included in the 2016 guidelines recommending prompt source control of infection as quickly as possible:
1. We recommend that a specific anatomic diagnosis of infection requiring emergent source control be identified or excluded as rapidly as possible in patients with sepsis or septic shock, and that any required source control intervention be implemented as soon as medically and logistically practical after the diagnosis is made (BPS). 2. We recommend prompt removal of intravascular access devices that are a possible source of sepsis or septic shock after other vascular access has been established (BPS).
Summary
Early recognition and diagnosis of sepsis is required to prevent the transition into septic shock, which is associated with a mortality rate of 40% or more. New definitions for sepsis and septic shock (Sepsis-3) have been developed. The new Sepsis-3 definition is “life-threatening organ dysfunction caused by a dysregulated host response to infection.” The clinical criteria for sepsis include suspected or documented infection and an acute increase of two or more SOFA points as a proxy for organ dysfunction. Septic shock is defined by the clinical criteria of sepsis and vasopressor therapy needed to elevate mean arterial pressure ≥65 mm Hg and lactate >2 mmol/L (18 mg/dL) despite adequate fluid resuscitation. A new screening tool for sepsis (qSOFA) has been proposed that includes Glasgow Coma Score of 13 or less, respiratory rate of 22 or more per minute, and systolic blood pressure ≤100 mm Hg. A qSOFA score of two or more identifies a patient at greater risk of poor outcome. The SSC guidelines were updated recently and include greater evidence-based recommendations for treatment of sepsis in attempts to reduce sepsis-associated mortality.
Footnotes
Author Disclosure Statement
No competing financial interests exist.