
Abstract
Abstract
Background:
Surgical site infection (SSI) complicates approximately 2% of surgeries in the Veterans Affairs (VA) hospitals. Surgical site infections are responsible for increased morbidity, length of hospital stay, cost, and mortality. Surgical site infection can be minimized by modifying risk factors. In this study, we identified risk factors and developed accurate predictive surgical specialty-specific SSI risk prediction models for the Veterans Health Administration (VHA) surgery population.
Methods:
In a retrospective observation study, surgical patients who underwent surgery from October 2013 to September 2016 from 136 VA hospitals were included. The Veteran Affairs Surgical Quality Improvement Program (VASQIP) database was used for the pre-operative demographic and clinical characteristics, intra-operative characteristics, and 30-day post-operative outcomes. The study population represents 11 surgical specialties: neurosurgery, urology, podiatry, otolaryngology, general, orthopedic, plastic, thoracic, vascular, cardiac coronary artery bypass graft (CABG), and cardiac valve/other surgery. Multivariable logistic regression models were developed for the 30-day post-operative SSIs.
Results:
Among 354,528 surgical procedures, 6,538 (1.8%) had SSIs within 30 days. Surgical site infection rates varied among surgical specialty (0.7%–3.0%). Surgical site infection rates were higher in emergency procedures, procedures with long operative duration, greater complexity, and higher relative value units. Other factors associated with increased SSI risk were high level of American Society of Anesthesiologists (ASA) classification (level 4 and 5), dyspnea, open wound/infection, wound classification, ascites, bleeding disorder, chemotherapy, smoking, history of severe chronic obstructive pulmonary disease (COPD), radiotherapy, steroid use for chronic conditions, and weight loss. Each surgical specialty had a distinct combination of risk factors. Accurate SSI risk-predictive surgery specialty-specific models were developed with number of variables ranging from 9 to 21 and the C-index ranging from 0.63 to 0.81, indicating acceptable discrimination. The decile plot of predicted versus observed SSI rates showed strong calibration.
Conclusions:
Surgery specialty-specific risk factors of 30-day post-operative SSI rates have been identified for a variety of surgery specialties. Accurate SSI risk-predictive surgery specialty-specific SSI predictive models have been developed and validated for the VHA surgery population. These models can be used to develop optimal preventive measures for high-risk patients, patient-centered care planning, and surgical quality improvement.
S
Surgical site infection surveillance is a major component of hospital and surgery quality improvement programs. Feedback of the results of surveillance systems and benchmark activities have shown a reduction in SSI rates [1,7,18–21]. The U.S. Centers for Disease Control and Prevention's National Healthcare Safety Network (NHSN) has tracked SSI for decades on some orthopedic and cardiac procedures. In line with the U.S. Centers for Disease and Prevention Control (CDC) guidelines for the prevention of SSI, the Veteran Affairs Surgical Quality Improvement Program (VASQIP) has collected SSI as deep wound infection, organ/space SSI, and superficial infection as a major 30-day post-operative morbidity and has been publishing the SSI rate of each surgical program on a quarterly basis. Most of the known SSI risk factors are surgeon- and procedure-related, with some patient characteristics; therefore, reduced SSI rates are hoped to be achieved by controlling modifiable risk factors [3].
Hospitals with high proportions of complex surgical procedures and patients with many comorbidities would expect higher SSI rates. Therefore, risk adjustment that accounts for the difference in patient case mix and surgical complexity is critical to allow for fair comparisons between hospitals [12,22,23]. A valid SSI risk identification algorithm could predict the risk of SSI accurately, and the predicted SSI risk might be helpful in the selection of patient-centered interventions to decrease the incidence of SSIs in practice [24].
The VHA surgery population is unique in patients' demographics with a majority of elderly, male patients [25,26). Neumayer et al. [27] have developed an SSI prediction score for general and vascular surgery specialties of the VASQIP. Currently, however, there are no specialty-specific risk adjustment SSI models reported for the 10 major surgical specialties of VASQIP data.
The main objective of this study was to identify the unique set of SSI risk factors for each surgical specialty and develop surgical specialty-specific predictive models. The risk models were used to develop an SSI risk score calculator. The risk calculator can be used by clinicians pre-operatively for SSI prevention planning.
Patients and Methods
Data selection and study population
The VASQIP prospectively collects pre-operative demographics, comorbidities, operative characteristics, and 30-day post-operative outcomes for eligible cases in 136 VA medical facilities with an approved VHA surgery program in accordance with VHA policies and procedures. Eligibility for VASQIP is determined by annual review of Current Procedure Technology codes with measurable risk of 30-day mortality and morbidity attributable to the surgical procedure. In this study, all eligible assessed cases from fiscal years 2014 to 2016 of the following surgery specialties were included: neurosurgery, urology, podiatry, otolaryngology, general, orthopedic, plastic, thoracic, vascular, cardiac coronary artery bypass graft (CABG), and cardiac valve/other surgery.
Outcome measures
The primary outcome of interest was post-operative 30-day SSI that includes deep wound infection, organ/space SSI, and superficial infection. All post-operative outcomes of VASQIP assessed cases within 30 days were recorded by VHA Surgical Quality Nurses based on clinical diagnosis and laboratory results in accordance with standardized national definitions [25,26].
Statistical analysis
All statistical analyses were performed using SAS, version 9.4 (SAS Institute Inc., Cary, NC). The study samples of each surgical specialty were divided randomly into a 60% development sample and a 40% validation sample for logistic regression model development. After validating the models in the 40% validation sample, the development and validation samples were combined, and the final model coefficients were calculated using the overall sample. The coefficients of the final models were published on the VHA intranet in the form of an SSI risk calculator for pre-operative consultation and planning.
For initial screening of candidate predictor variables, all possible variables from the VASQIP database were considered. Missing data in the VASQIP database are rare. Some extreme values are mostly because of data entry errors or coding errors; therefore, these extreme values were set to missing. Missing data were imputed by the multi-imputation approaches using IVEWare software (Survey Research Center Director's Office University of Michigan, Ann Arbor, MI) [28]). Considering the non-linear association with the outcome and the purpose of simple implementation of the SSI risk calculator in clinical practice, some numeric variables were categorized based on clinical significance or standard practice.
The Hosmer and Lemeshow purposeful selection model building algorithm was used for initial predictor variable screening [29]. Several variables were included in the models regardless of statistical significance because of clinical importance. Some interaction terms were also examined in the model development process. The discrimination performance of the models was expressed by constructing area under the curve (AUC). The calibration performance of the models was assessed by constructing calibration plots, relating the predicted and observed probabilities. The goodness-of-fit of the final model was assessed by the Hosmer-Lemeshow test. The accuracy of the models was also judged by Brier scores.
Results
A total of 354,528 surgical procedures were included for the SSI predictive models development. The surgical specialties included in this study were: neurosurgery, urology, podiatry, otolaryngology, general, orthopedic, plastic, thoracic, vascular, cardiac CABG, and cardiac valve/other surgery. The procedure volumes varied among the surgical specialties ranging from 108,813 to 6,508 (Tables 1 and 2). The observed postoperative 30-day SSI rates varied substantially among different surgical specialties, ranging from 0.7% to 3.0% (urology vs. vascular surgery, p < 0.001, Tables 1 and 2). The mean and median duration of operation also varied among surgical specialties (Tables 1 and 2). Longer duration of operation was associated with increased SSI rate (Table 3). In general surgery, the SSI rate of surgeries with duration of operation of one hour or less was 1.2%, whereas SSI rate was 13.1% for operations longer than four hours (p < 0.001). Similar trends were identified in all other surgical specialties (Table 3).
RVU = relative value unit; SSI = surgical site infection.
CABG = coronary artery bypass graft.
SSI = surgical site infection; CABG = coronary artery bypass graft.
The VHA Surgery Programs are assigned surgical complexity level in accordance with VHA policy, standardizing the facility infrastructure and surgical procedure assignments to ensure high quality and safe delivery of surgical operations [25]. The complexity of surgical procedures was associated with observed SSI rate in most surgical specialties. Surgical site infection rates were higher in intermediate or complex procedures of general, orthopedic, otolaryngology, thoracic surgery, and urology. A similar pattern was not found in the vascular, plastic, and neurosurgery specialties (Table 4). Higher operative work relative value unit (RVU) was associated with higher SSI rates (Table 5). In general surgery, the SSI rate of procedures with RVU less than or equal 12 was lower than that of procedures with operation RVU greater than 12 (1.1% vs. 7.0%, p < 0.0001, Table 5). Emergent cases had a higher SSI rate compared with elective cases (1.7% vs. 4.5%, p < 0.0001). The proportion of emergent cases in cases with SSI and cases without SSI were 3.8% and 9.7%, respectively (p < 0.0001, Table 5).
RVU = relative value unit.
Other risk factors of SSI were American Society of Anesthesiology (ASA) classification, dyspnea, open wound/infection, wound classification, ascites, bleeding disorder, chemotherapy, smoking, history of severe chronic obstructive pulmonary disease (COPD), radiotherapy, steroid use for chronic conditions, and weight loss greater than 10% in the past six months (Table 6). The prevalence of patient comorbidities among surgical specialties was different. For example, the history of severe COPD of plastic surgery patients was 8.1% whereas it was 38.6% for thoracic surgery patients (p < 0.001). The proportion of patients with open wound infection was 1.4% and 22.9%, respectively, in urology surgery and vascular surgery (Table 6). The intra-operative characteristics also varied among surgery specialties. The mean operative times were 1.9 hours and 3.0 hours for general surgery and thoracic surgery, respectively (p < 0.001). The proportions of complex procedures were 0.1% and 17.3%, respectively, for orthopedic and neurosurgery (p < 0.001). The most common variables included were surgery duration, wound classification, and diabetes mellitus. The number of variables included in the specialty-specific predictive models ranged from 9 (cardiac valve/other surgery) to 21 (vascular surgery).
SSI = surgical site infection; BUN = blood urea nitrogen; COPD = chronic obstructive pulmonary disease.
For the specialty-specific SSI risk models, the c-index ranged from 0.63 (neurosurgery) to 0.81 (urologic surgery). The model calibration by predictive versus observed percentile plot also showed reasonable results (Fig. 1).
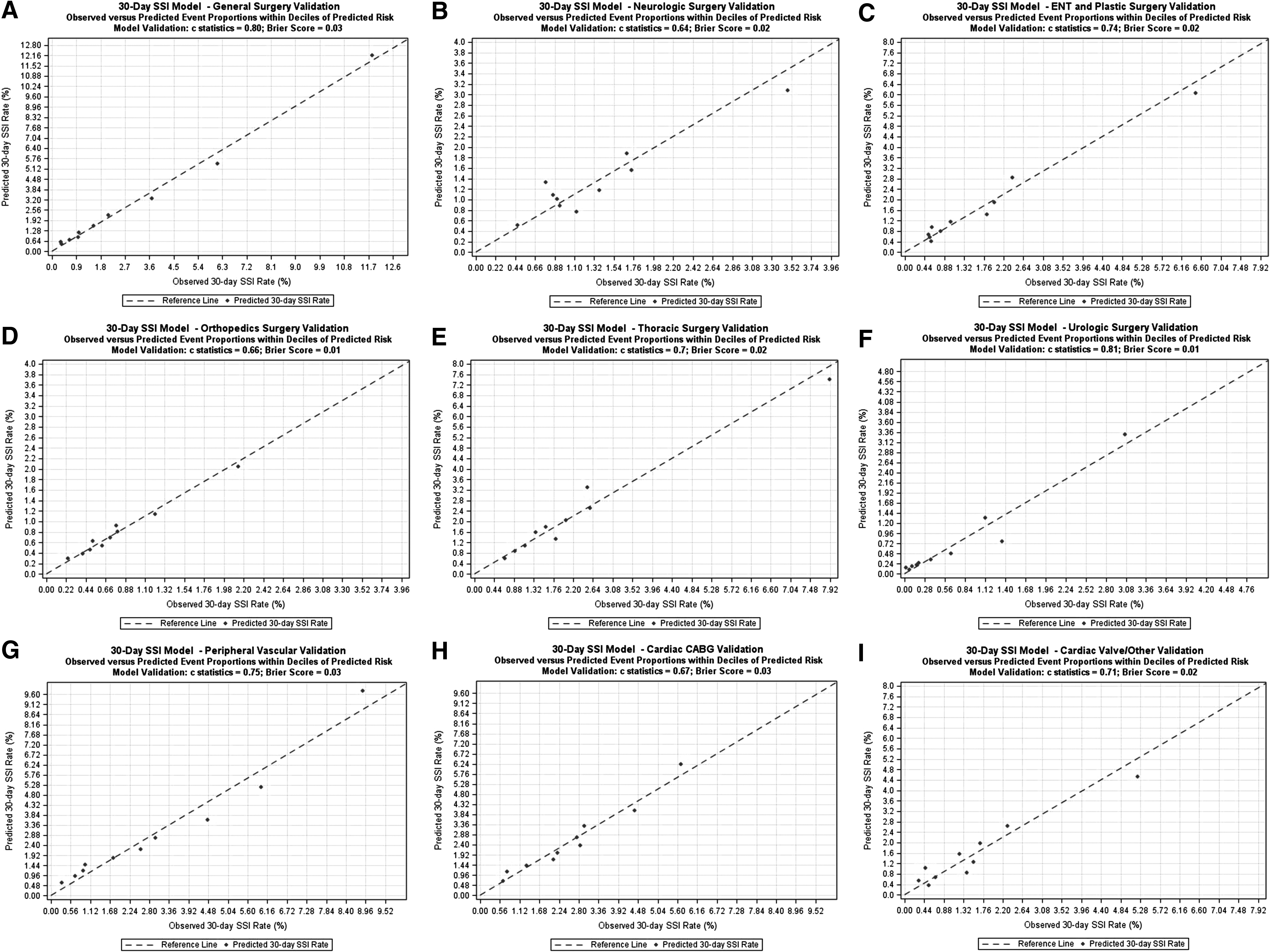
Plots of observed versus predicted 30-day post-operative surgical site infection (SSI) event proportions within deciles of predicted risk in the validation samples of multiple surgery specialties for predictive model calibration. (
Discussion
Identification of high-risk SSI patients is an essential step for patient-centered care to reduce post-operative complications. Surgical site infection risk factors for the VA surgery population have been identified and 10 surgery specialty-specific SSI models have been developed. Variables describing poor health status such as comorbidities, poor functional status, high ASA classification level, and increased body mass index are associated with increased risk of SSI. Some intra-operative factors are associated with increased risk of SSI such as extended duration of operation and surgical complexity. Therefore, a reduction of SSI rates could be achieved by controlling modifiable risk factors.
Despite widespread initiatives of preventive measures by government agencies and healthcare institutes, SSIs continue to occur although SSI rates have been decreasing consistently across the surgery specialties. Evidence suggests that there is still a remaining gap and a potential benefit to further reduce SSI in high SSI-risk patient groups. Given that patient-level and operative-level SSI risk factors have been identified in the VHA surgery population, patients with the greatest need for optimal preventive measures can be identified and patient-centered plans can be made prior to surgery. High reliability in post-operative complication prediction allows the patient and family to participate in the patient-centered care planning process and to discuss goals of care with the surgical team. In this report, we have identified the most common SSI risk factors as operative duration, type of surgery, and complexity of surgery procedures. However, each surgery specialty has its unique set of risk factors. We have developed surgery specialty-specific SSI predictive models because the variations of SSI incidence, operative characteristics, and pre-operative comorbidities of patients in different surgery specialties. Model validation results have shown excellent predictive performance of these models. A VASQIP online risk calculator including SSI risk has been developed based on these models. Our observation and other reports have shown that apparent differences between hospitals in SSI rates can be explained mostly by patient and intra-operative characteristics. The remaining part of observed unadjusted difference in SSI rates between hospitals are likely to be associated with quality of care difference among the hospitals. Therefore, these models can be applied to generate the observed/expected SSI ratios for SSI surveillance and surgical quality improvement.
This study is strengthened by including all VASQIP-assessed procedures from a variety of surgery specialties in VHA, a large integrated healthcare system with a common electronic health record, manual data entry at each VHA surgery program for pre-operative comorbidities, and 30-day post-operative outcomes. This study has limitations, the first of which is that it was retrospective. Second, most patients were older and predominantly male. The generalizability of the results and the application of the risk calculator to females and to the non-VA population may be limited. Nevertheless, this is the first surgery specialty-specific SSI predictive model for the VA surgery population that can be used for identifying high-risk patients, developing patient-centered care plans, and surgical quality improvement.
In brief, surgery specialty-specific SSI predictive models have been developed for the U.S. veteran surgery population. Overall model performance was acceptable. This report includes a detailed exposition of the model development process. These models can be used to predict post-operative 30-day SSI risk after VASQIP eligible surgical procedures in the VHA population and for surgery quality improvement.
Conclusions
Thirty-day post-operative SSI rates varied significantly across surgical specialties. Duration and complexity of surgery, comorbidities, and patient dependence and frailty were found to be associated with an increased risk of SSI. There were differences in operative characteristics and patients' demographic and clinical characteristics among surgery specialties. Therefore, surgery specialty-specific SSI predictive models have been developed and validated for the VHA surgery population. These models could be utilized to develop optimal preventive measures for high-risk patients, patient-centered care planning, and surgical quality improvement. Future studies would be focused to identify the distinct risk factors for different SSI types to better inform potential quality improvement strategies.
Footnotes
Author Disclosure Statement
No competing financial interests exist.