
Abstract
Abstract
Background:
Clinical practice guidelines recommend a 2-g dose of cefotetan and cefoxitin for surgical prophylaxis. Pharmacokinetic data suggest benefit from higher cefotetan and cefoxitin dosing in obese patients. However, clinical studies examining higher dosing strategies in this at-risk population are lacking. The purpose of this study was to determine whether 3 g of cefotetan or cefoxitin administered pre-operatively for patients who weigh 120 kg or more is associated with a lower proportion of surgical site infection (SSI) compared with 2 g.
Patients and Methods:
Medical records of patients weighing 120 kg or more who had received cefotetan or cefoxitin (2 or 3 g) as surgical prophylaxis for intra-abdominal procedures between July 2012 and August 2015 were reviewed for the development of an SSI (primary outcome), study drug-related adverse events, and re-admissions attributed to SSIs (secondary outcomes). Relative risk calculations were performed for analysis of the primary and secondary outcomes.
Results:
One-hundred seventy-five procedures in 169 patients were included in the study. Cefotetan was used in 81% (141/175) of procedures. Three grams of cefotetan or cefoxitin was used in 20% (35/175) of procedures. The median body mass index (BMI) in both dosing groups was 42 kg/m2 and patients who received 3 g more often weighed more than 130 kg (relative risk [RR] 1.36, 1.01–1.76; p = 0.04). Surgical site infections occurred in 20.7% within the 2-g group and 22.9% in the 3-g group (RR 1.10, 0.55–2.20; p = 0.78). There was no difference in the number of study drug-related adverse effects in the 3-g compared with the 2-g group. Thirty-day re-admissions because of SSI also did not differ between the 2-g and 3-g groups (7.9% vs. 17.1%, respectively; p = 0.11).
Conclusion:
This small retrospective study did not find a difference in SSI rates between 3-g and 2-g surgical prophylaxis dosing for patients 120 kg or more with a median BMI >40 kg/m2.
C
Despite the higher rate of SSI in the obese population, no studies have assessed doses higher than 2 g of cefotetan or cefoxitin for surgical prophylaxis in obese, or extremely obese, patients. It is unknown whether doses greater than 2 g may reduce the proportion of SSIs without increased drug-related adverse events. However, Guidelines for Antimicrobial Prophylaxis in Surgery do recommend 3 g of cefazolin (a first generation cephalosporin) in patients weighing ≥120 kg for all procedures [1]. Recent pharmacokinetic studies of cefazolin have demonstrated an increased volume of distribution and clearance in obese patients as compared to non-obese patients [4–6]. Cefazolin tissue concentrations were evaluated in 38 extremely obese patients (BMI >40 kg/m2) who received 2 g of cefazolin pre-operatively, followed by a second 2-g dose three hours later, for Roux-en-Y gastric bypass surgery [6]. Therapeutic tissue concentrations (8 mcg/mL) were achieved in 10.2% of the highest BMI group (BMI ≥60 kg/m2), compared with 48.1% of the lowest BMI group (BMI 40–49 kg/m2).
In 2013, our institution changed surgical prophylaxis dosing guidelines to recommend 3 g of cefotetan or cefoxitin for surgical prophylaxis in patients weighing 120 kg or more. We studied whether 3 g of cefotetan or cefoxitin was associated with a lower proportion of subsequent SSI compared with 2 g in patients who weigh 120 kg or more.
Patients and Methods
This study was conducted at a 1,059-bed tertiary medical center in Baltimore, Maryland. A retrospective cohort of patients, weighing 120 kg or more, undergoing intra-abdominal procedures (Fig. 1) who had received cefotetan or cefoxitin (2 or 3 g) as surgical prophylaxis between July 2012 and August 2015 was established. From August 2015, in keeping with emerging evidence at that time and frequent cefotetan drug shortages, our institution changed antimicrobial prophylaxis for all intra-abdominal procedures from cefotetan to cefazolin plus metronidazole. Patients determined to have an active infection before the surgical procedure or who died within five days were excluded. For patients who underwent multiple procedures at the same site within 30 days (90 d for herniorrhaphy), only the first procedure was included. Of note, in February 2014, our institution implemented Early Recovery After Surgery (ERAS) protocol in colorectal surgery patients that included mechanical bowel preparation plus oral antibiotics [7]. The study was reviewed and approved by the Johns Hopkins University School of Medicine Institutional Review Board.
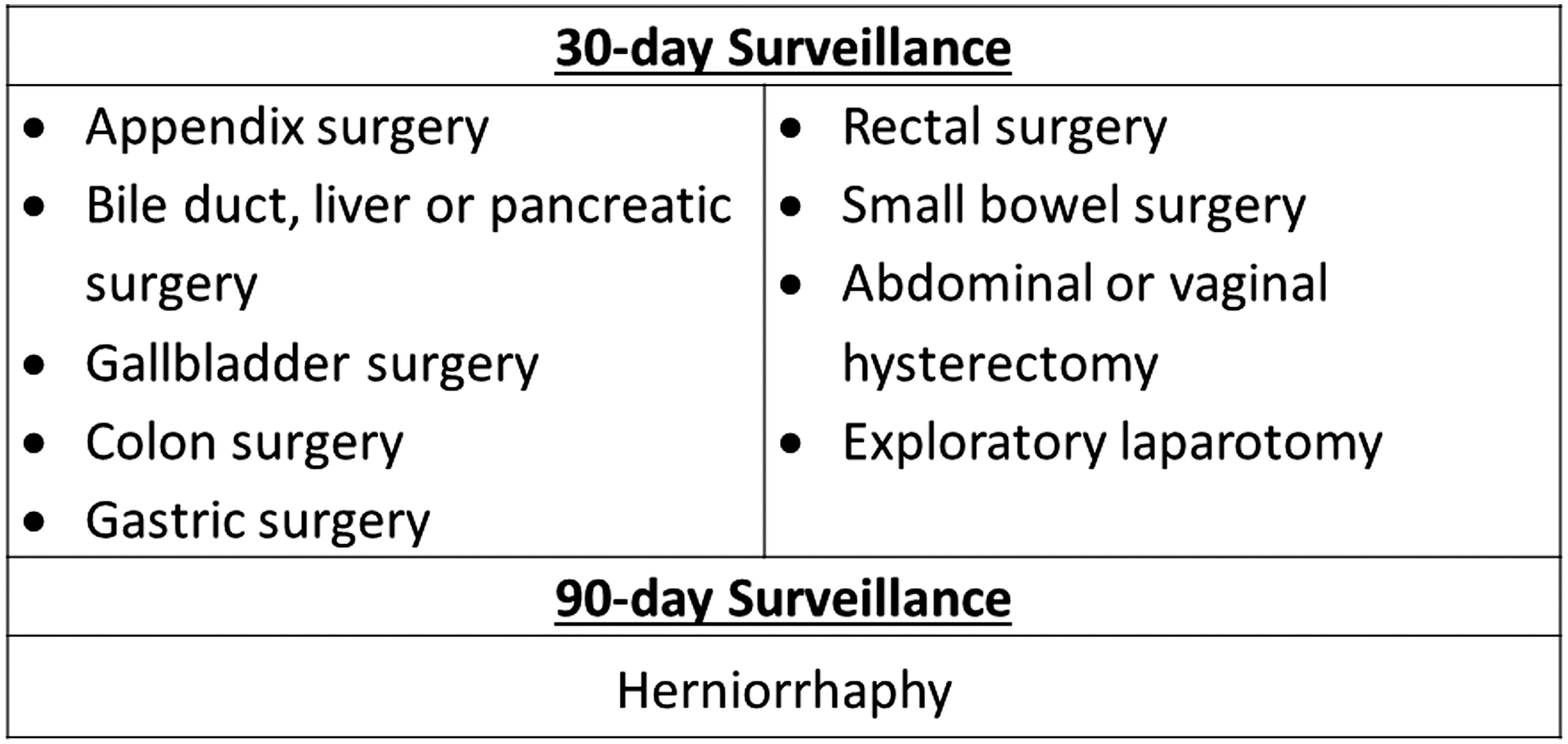
Included procedures utilizing cefotetan or cefoxitin prophylaxis requiring 30- and 90-day surveillance. For herniorrhaphy, deep and organ/space infections undergo 90-day surveillance. For superficial infections after herniorrhaphy, the surveillance period is 30 days. Herniorrhaphy procedures included ventral/incisional, umbilical, epigastric, and para-esophageal hernia repairs.
Surgical site infection was defined as superficial incisional, deep incisional, or organ/space as per U.S. Centers for Disease Control and Protection National Healthcare Safety Network (CDC-NHSN) SSI surveillance definitions [8]. All cases of SSI and any cases with ambiguity were reviewed and confirmed by an infection preventionist experienced in SSI surveillance. The presence of the following SSI risk factors was determined for all patients: pre-existing diabetes mellitus (defined as a current diagnosis noted in the medical chart), post-operative blood glucose higher than 180 mg/dL, tobacco use at the time of surgery, recent surgical procedure within 90 days, pre-operative hospitalization longer than seven days, blood loss greater than 1,500 mL, and immunosuppression. Immunosuppression was defined as presence of any of the following: hematologic malignancy; bone marrow or solid organ transplant; human immunodeficiency virus (HIV; with CD4 count <200 cells/mm3); receipt of corticosteroids (2 mg/kg of body weight or a total of 20 mg/d of prednisone or equivalent for greater than or equal to two weeks in the preceding 3 months); active chemotherapy in the past six months; receipt of medications that target immunophilins, immune-suppressing interferons, or monoclonal antibodies; and receipt of mycophenolate or azathioprine. Appropriate initial dosing of cefotetan or cefoxitin was defined as administration of these agents within one hour prior to surgical incision. Appropriate re-dosing of cefotetan or cefoxitin was defined according to institutional guidelines; patients with a creatinine clearance (CrCl) >60 mL/min are re-dosed with cefotetan every six hours and for every 1,500 mL of blood loss and with cefoxitin every two hours. Patients with a CrCl <60 mL/min are re-dosed less frequently (every 12 h with cefotetan and every 4 or 6 h with cefoxitin), and patients with a CrCl <10 mL/min or on hemodialysis do not require intra-operative re-dosing with these agents.
The primary outcome of the study was the difference in proportion of SSI between the two groups. Secondary outcomes were study drug-related adverse events and re-admissions attributed to SSI. Compliance with institutional dosing guidelines was also assessed.
For the purpose of these analyses, cefotetan and cefoxitin were combined and the 2-g versus 3-g dosing strategies were compared. Comparison of demographic data, procedure type, and primary and secondary end points were conducted utilizing relative risk calculations. The 95% confidence interval and p values were reported for each comparison. The a priori level of significance was set at 0.05. A univariable analysis was conducted to analyze the association between potential SSI risk factors and the proportion of procedures resulting in a SSI. Any significant variables in the univariable analysis would be included in a multivariable analysis. The data analysis and statistical software tool, Stata (version 13.1, StataCorp, College Station, TX) was used to perform statistical functions.
Results
One hundred sixty-nine patients who had undergone 175 procedures were included in the study (Fig. 2). Baseline demographics between the two groups were generally similar (Table 1), however, there were more patients with diabetes mellitus in the 2-g dosing group (RR 2.56, 0.98–6.68; p = 0.03; Table 2). When further categorized by weight, 69% of patients in the 3-g group weighed greater than 130 kg compared with 51% of patients in the 2-g group (RR 1.36, 1.01–1.76; p = 0.041). Cefotetan was used in 81% (141/175) of procedures. The 3-g dosing strategy was utilized in 20% (35/175) of all procedures. The majority of patients underwent colon (22%) followed by bile duct, liver, or pancreatic surgeries (25%; Table 1).

Study flowchart showing reasons for exclusion. Procedures for patients who weighed 120 kg or more, undergoing an intra-abdominal procedure (listed in Fig. 1), who had received 2 or 3 g of cefotetan or cefoxitin as surgical prophylaxis between July 2012 and August 2015 were screened. SSI = surgical site infection.
BMI unavailable for 6 patients.
IQR = interquartile range; BMI = body mass index.
SSI = surgical site infection.
There was no difference in the proportion of patients who developed SSI between the two dosing groups: 20.7% received 2 g versus 22.9% received 3 g (RR 1.10, 0.55–2.20; p = 0.78). The depth of infection was not substantially different between two dosing groups (Table 3). In a univariate analysis, diabetes mellitus, post-operative blood glucose higher than 180 mg/dL, current tobacco use, recent surgical procedure within 90 days, immunosuppression, 2-g dosing, receipt of cefoxitin, and doses and re-doses administered inappropriately, were not associated with an increased risk of SSI (Table 4). We did not perform a multivariable analysis because there were no differences between groups on univariate analysis. In the subset of patients undergoing colorectal procedures after implementation of the ERAS protocol, the SSI rate was 17.6% (3/17) compared with 29.6% (8/27) in patients prior to protocol implementation (p = 0.39).
SSI = surgical site infection
SSI = surgical site infection.
In the cohort, the overall compliance rate with the timing of an initial dose was 94.4% and appropriate administration of an intra-operative re-dose was 85.3%. No differences were observed for administration within the 60-minute time window for 3-g compared with 2-g doses (88.9% vs. 95.8%; p = 0.237). There was no significant difference between the 2-g and 3-g dosing groups regarding the number of procedures for which re-dosing occurred at the appropriate time for patients meeting criteria (re-dose given for patient meeting criteria 81.1% vs. 95.5% for 2 g vs. 3 g, respectively, p = 0.11).
Five patients (2.9%) experienced drug-related adverse events. Three patients developed immediate or accelerated penicillin reactions (one patient in the 2-g group and two patients in the 3-g group) and two patients developed Clostridium difficile diarrhea within 30 days (one patient in each group). Thirty-day re-admissions because of SSI were not significantly different between the two dosing groups (7.9% in the 2-g group vs. 17.1% in the 3-g group; p = 0.11).
Discussion
Rates of SSI in this extremely obese population undergoing intra-abdominal procedures at our institution were high, which is consistent with previously published studies [2,9,10]. However, we did not demonstrate a significant difference in the proportion of SSI between patients weighing 120 kg or more who received 2 g versus 3 g of cefotetan or cefoxitin as surgical prophylaxis. Our clinicians used 3-g dosing in patients weighing 120 kg or more in only 20% of patients and were more likely to use higher doses if patients weighed 130 kg or more, which may have limited our ability to evaluate whether higher doses are more effective in preventing SSI. Importantly, there was no statistically significant difference in adverse events between the two groups suggesting that 3-g doses of cefotetan and cefoxitin can be administered safely for surgical prophylaxis.
Pharmacokinetic data suggest that higher doses of cefotetan and cefoxitin may be needed to prevent SSIs in obese patients. In the aforementioned study by Itani et al. [2], cefotetan 2 g was compared with ertapenem 1 g in a randomized double-blind study of 650 patients undergoing elective colorectal surgery. In the sub-group of patients with a BMI >30 kg/m2, a higher proportion of patients in the cefotetan group experienced an SSI compared with the ertapenem group (41.9% vs. 26.7%, respectively), suggesting that cefotetan at a 2-g dose was potentially sub-optimal or that broader coverage with ertapenem was needed. Toma et al. [11] analyzed plasma and tissue concentrations of 2 g of cefoxitin in 14 obese patients (BMI 43 kg/m2) undergoing abdominal and pelvic surgery as compared to 13 normal-weight patients (BMI 20 kg/m2) receiving 1 g of cefoxitin [11]. The tissue penetration was substantially lower in the obese patients compared with normal-weight patients (0.08 vs. 0.37, p < 0.05), with adipose tissue concentrations below the minimum inhibitory concentrations for aerobic and anaerobic micro-organisms. Despite pharmacokinetic data suggesting potential under-dosing with 2 g of cefazolin, cefotetan, or cefoxitin in obese patients, similar to our findings, studies have yet to demonstrate a reduction in SSI with 3-g doses. Cefazolin 2 g was compared with 3 g administered as surgical prophylaxis in pregnant women weighing 104 kg or more undergoing cesarean delivery, but there was no difference in the proportion of SSI among women who received either dose (13% vs. 13%, p = 0.996) [12]. Furthermore, cefazolin 4 g was compared with 2 g in 20 patients with a BMI >35 kg/m2 who underwent cesarean delivery in a randomized controlled trial [13]. The investigators found that 4 g of cefazolin resulted in significantly higher subcutaneous incision site tissue concentrations (40.11 mcg/g vs. 18.36 mcg/g, p = 0.0005), but both dosing groups achieved tissue concentrations that were above the target of 4 mcg/g and no patients developed an SSI [13]. However, studies such as these are lacking in higher risk procedures such as colon, where there may truly be a benefit for higher doses.
Previous published studies are subject to limitations. There is no standard approach used to define SSI, therefore it is challenging to compare outcomes and findings from different studies. In addition, many published studies report all obese patients together, rather than stratifying by BMI; those with BMI >40 are likely have higher SSI rates than those with lower BMI. Wick et al. [9] found a substantially higher rate of SSI (as defined by the National Surgical Quality Improvement Program) in obese (defined as a BMI ≥30 kg/m2 and/or an ICD-9-CM diagnosis of obesity) patients undergoing colorectal surgery compared with non-obese patients (14.5% vs. 9.5%, respectively; p < 0.001) although BMI was not stratified to show rates for extreme BMI. In a meta-analysis assessing the association between obesity and SSI after elective colorectal surgery, the odds of SSI in patients with a BMI ≥30 kg/m2 was 1.6 times that of patients with BMI <30 kg/m2 (pooled odds ratio [OR] 1.60; 95% CI 1.34, 1.86; p < 0.001) [10]. The majority of patients in our study were extremely obese (median BMI of 42 kg/m2), which may account for the higher proportion of SSIs observed compared with other studies.
Surgical site infections are complex and usually multi-factorial in etiology. Previous studies have identified surgical strategy (e.g., open operation vs. laparoscopic approach), blood loss, and diabetes mellitus as independent risk factors for SSI [11–14]. Our study did not analyze incision closure, transfusion, or open versus laparoscopic procedure. We did not find an association between blood loss greater than 1,500 mL or diabetes mellitus and the proportion of SSI. Procedure type is also an independent risk factor for development of an SSI. Forty-seven percent of the procedures in our study were colon or bile duct, liver, or pancreatic procedures, which are high-risk for SSI according to the NHSN criteria [8]. The large number of high-risk procedures, coupled with our inclusion of only patients weighing 120 kg or more likely explains the high SSI rate we found. Another factor that may be related to the higher rates of SSI observed in this study includes the choice of cefotetan or cefoxitin for surgical prophylaxis. Although these are still recommended by the Clinical Practice Guidelines for Antimicrobial Prophylaxis in Surgery, some studies suggest these may be less effective agents than other prophylactic antimicrobials [15,16].
Another dosing strategy that warrants further study is continuous infusion, as this has recently been shown to be beneficial with cefazolin. Anlicoara et al. [17] analyzed the concentration of cefazolin in adipose tissue of 18 patients undergoing bariatric surgery with a BMI of 35 to 50 kg/m2 who received an initial dose of cefazolin 2 g followed by a continuous infusion of cefazolin 1 g administered over two hours. No patients in this study developed an SSI. Another prospective, cross-sectional study evaluated the rates of SSI in 896 patients undergoing Roux-en-Y gastric bypass procedures and compared the following three groups: (1) patients who received two 3-g doses of ampicillin/sulbactam; (2) patients who received a 1-g dose of ertapenem; and (3) patients who received a 2-g dose of cefazolin followed by a continuous infusion of 1 g of cefazolin. The rates of SSI were lowest in the continuous infusion cefazolin group [18]. Further research is needed to determine whether continuous infusion of cefoxitin or cefotetan is a safe and effective strategy for optimizing surgical prophylaxis.
There are several limitations to our study. Uptake of the 3-g dosing strategy by our clinicians for patients weighing 120 kg or more was low, making it difficult to assess a true impact of 3-g dosing. Additionally, doses in excess of 3 g were not used, and it is possible given our cohort with median BMI of 42 kg/m2, even higher doses would be needed to demonstrate improvement. Although we used an objective, validated, standard definition for surgical site infection (CDC-NHSN), as with any retrospective study, determination of SSIs and adverse events were dependent upon documentation in the medical record. Additionally, we were unable to capture development of SSI for patients who were lost to follow-up or may have sought care outside of our institution.
Conclusion
For adult patients weighing 120 kg or more with a median BMI of 42 kg/m2, in this retrospective observational study, there was no significant difference in the proportion of SSI in those receiving 2 g versus 3 g (cefotetan or cefoxitin) for surgical prophylaxis. Importantly, there was no increase in adverse events or re-admissions in the 3-g group. Obesity, particularly extreme obesity, is a known risk factor for SSI; further larger prospective studies are needed to examine this and other dosing strategies to reduce SSI in this population.
Footnotes
Acknowledgment
Preliminary results of this study were presented as a podium presentation at the 35th Annual Eastern States Conference for Pharmacy Residents and Preceptors on May 4, 2016 in Hershey, Pennsylvania.
Author Disclosure Statement
No competing financial interests exist.