
Abstract
Abstract
Background:
Although there are some commonalities between pediatric and adult sepsis, there are important differences in pathophysiology, clinical presentation, and therapeutic approaches. The recognition and diagnosis of sepsis is a significant challenge in pediatric patients as vital sign aberrations and examination findings are often subtle as compared to those observed in adults. Gaps in knowledge that have been studied in depth in adult sepsis are still being investigated in pediatric patients such as best practices in ventilation, invasive monitoring, and resuscitation.
Discussion:
In this review, we address key differences in the etiology, presentation, resuscitation, and outcomes of sepsis in children compared with adults.
T
Etiology
The causes of sepsis in the pediatric population are somewhat unique from those attributed to adult sepsis. Early-onset neonatal sepsis, within the first 72 hours of life, is most likely to result from group B streptococcus (GBS), Escherichia coli, Klebsiella spp., Enterobacter spp., and Listeria monocytogenes. The most common etiologies of late-onset neonatal sepsis, after the first 72 hours of life, include coagulase-negative staphylococci, gram-negative bacilli, Enterobacteriaceae, and both methicillin-sensitive and methicillin-resistant Staphylococcus aureus. In older children, the most common etiologies are Staphylococcus, Streptococcus, Pseudomonas, and Meningococcus [14]. Emergence of multi-drug–resistant organisms, especially in the intensive care unit (ICU), requires special attention and thoughtful antimicrobial choices [15]. Data suggest there is increased mortality with infections secondary to multi-drug–resistant organisms [16].
Presentation and Diagnosis of Pediatric Sepsis
The clinical presentation of sepsis in neonates and children can be subtle and may be difficult to identify. The definition of sepsis in the adult population was recently revised to include the presence of infection together with systemic manifestations of infection including hyperthermia or hypothermia, tachycardia, tachypnea, altered mental status, edema, hyperglycemia, leukocytosis, or leukopenia [17]. However, the definition of pediatric sepsis has remained constant since the International Consensus Conference on Pediatric Sepsis in 2005 [9]. Pediatric sepsis is currently defined as the triad of fever, tachycardia, and vasodilation in addition to a change in mental status or prolonged capillary refill greater than 2 seconds. The appropriate criteria were updated to delineate each of the following age groups: newborns (0 days to 1 week), neonates (1 week to 1 month), infants (1 month to 1 year), toddler/pre-schoolers (2–5 years), children (6–12 years), and adolescents (13–18 years; Table 1).
From Goldstein et al. [9].
NA = not applicable.
The systemic inflammatory response syndrome (SIRS) criteria in children are modified from adult criteria to include either fever or white blood count. This definition requires the presence of at least two of the following criteria, one of which must be abnormal temperature or leukocyte count: core temperature greater than 38.5°C or less than 36°C, tachycardia more than 2 standard deviations (SD) above normal for age group or bradycardia for children older than 1 year of age, mean respiratory rate greater than 2 SD above normal for age group or mechanical ventilation, and leukocyte count elevated or depressed for age or greater than 10% immature neutrophils (Table 1). Bradycardia is included as a sign of sepsis only in the newborn age group; older children do not exhibit bradycardia except as a near-terminal event in shock. Core temperature measured by rectal, bladder, oral, or central catheter is required, and it should be noted that elevated temperature may be caused by over-bundling in small infants and the temperature should be retaken after unwrapping [9].
As in adult care, sepsis is defined as SIRS in the presence of an infection [9], which may be viral, bacterial, fungal, or rickettsial in origin. Not all pathogens can be identified by standard culture and clinical or radiographic means of diagnosis are often required. Despite this limitation, Pediatric Advanced Life Support (PALS) guidelines recommend the administration of antibiotics in the first hour and urgent source control of the infection (Fig. 1). Pediatric severe sepsis is defined as sepsis plus one of the following: cardiovascular organ dysfunction, acute respiratory distress syndrome, or the presence of dysfunction in two or more other organs [9]. Scoring systems used in adults to measure organ dysfunction have not been validated in children for widespread use. Pediatric septic shock is defined as sepsis with cardiovascular organ dysfunction despite the administration of isotonic intravenous fluid bolus greater than 40 mL/kg in the first hour [9]. This diagnostic feature can be problematic in that children will often maintain a normal blood pressure until they progress to severe cardiovascular decompensation. Thus, the presence of hypotension is not needed to diagnose pediatric patients with septic shock as in adults. Therefore septic shock more aptly refers to tachycardia with signs of decreased perfusion such as decreased peripheral pulses, altered mental status, capillary refill more than 2 seconds, mottled extremities, or decreased urine output. Hypotension is a late and ominous sign of shock in children [7,18] (Table 2).
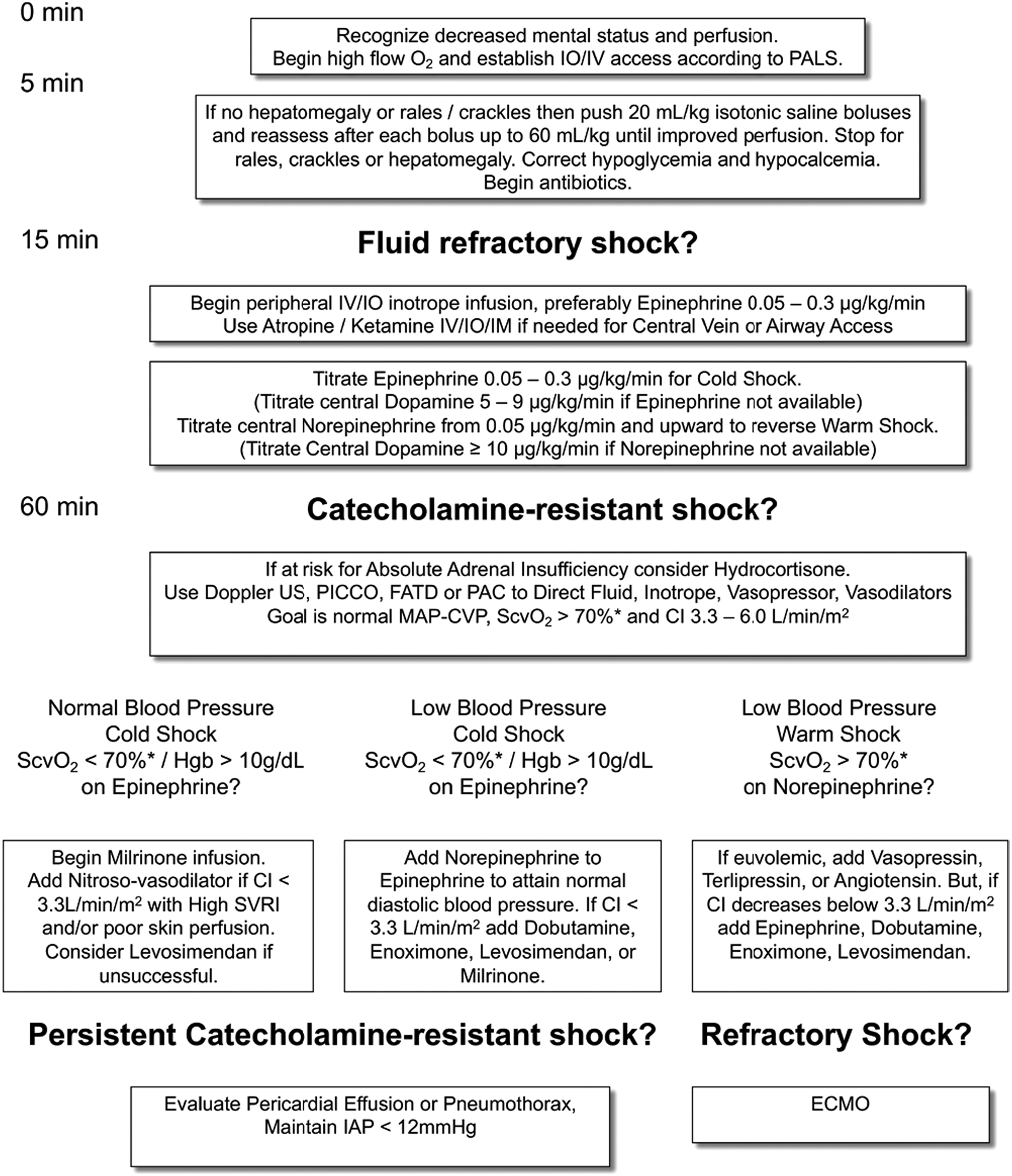
American College of Critical Care Medicine algorithm for time-sensitive, goal-directed stepwise management of hemodynamic support in infants and children. Proceed to next step if shock persists. (1) First-hour goals: Restore and maintain heart rate thresholds, capillary refill >2 seconds, and normal blood pressure in the first hour/emergency department. (2) Subsequent ICU goals: If shock not reversed proceed to restore and maintain normal perfusion pressure (MAP-CVP) for age, Scvo2 > 70% (*except congenital heart failure patients with mixing lesions), and cardiac index greater than 3.3 < 6.0 L/min/m2 in PICU [21]. Copyright permission granted from: Davis AL, Carcillo JA, Aneja RK, et al. American College of Critical Care Medicine Clinical Practice Parameters for Hemodynamic Support of Pediatric and Neonatal Septic Shock. Crit Care Med 2017;45:1061–1093.
SVV = stroke volume variation; CVP = central venous pressure.
Several key differences distinguish pediatric-onset septic shock from adult disease [12]. First, pediatric patients manifest a differential hemodynamic response to sepsis. In the neonate, the recognition and early treatment of septic shock can be complicated by the transition from fetal circulation. Increased pulmonary resistance and low pulmonary blood flow can prevent adequate gas exchange, resulting in hypoxemia. Acidosis and hypoxia can potentiate pulmonary vascular tone leading to pulmonary hypertension. This can result in increased right ventricular afterload and cardiac failure. Treatment with inhaled nitric oxide, oxygen, and phosphodiesterase III inhibitors may be required early on in management [19]. By contrast, there are no roles for these therapies in adults, and in fact, nitric oxide may contribute to hypotension and multiple organ failure [20].
Second, whereas adults with sepsis generally present with “warm” shock (decreased systemic vascular resistance, hypotension, and tachycardia), up to 50% of children will present with “cold” shock, characterized by elevated systemic vascular resistance, limited cardiac reserve, and clamped down extremities. Children also have limited cardiac reserve and may not benefit hemodynamically from increased heart rate in the same manner that adults do. Their resting heart rates are comparatively high and tachycardia may not allow for adequate diastolic filling. Therefore, children respond to decreased cardiac output by vasoconstriction. The resultant hypotension is a late and ominous sign of shock.
Pediatric Resuscitation
The primary goal of early management of pediatric sepsis is reversal of the shock state as assessed by close clinical observation of hemodynamic status, capillary refill, extremity perfusion, quality of pulses, urine output, and mental status to guide adjustments to therapy per the 2014 American College of Critical Care Medicine/Pediatric Advanced Life Support (ACCM/PALS) guidelines (Fig. 1). Continuous heart rate, respiratory rate, invasive blood pressure, and central venous pressure monitoring provide necessary data to help the provider adjust therapies as needed [21]. After the diagnosis of septic shock, adequate intravenous access and fluid resuscitation should begin immediately. In general, fluid resuscitation begins with intravenous administration of isotonic saline or colloid solutions at 20 mL/kg until perfusion improves or signs of fluid overload are observed. Delays in fluid resuscitation of up to 30 minutes after identification or under-resuscitation with less than 40 mL/kg in the first hour has been shown to be associated with increased risk of mortality in children over the age of 2 years [22]. As noted above, pediatric patients differ from adults in that they often require more fluid resuscitation in the immediate treatment phase for the shock state. Children are also much less susceptible to volume overload because of preserved cardiac and renal function. The ACCM/PALS guidelines recommend fluid replacement up to 40–60 mL/kg in the first hour to reverse shock as long as there are no clinical signs of fluid overload [21] (Fig. 1).
Treatment
Hemodynamic support
Hemodynamic support is often needed to ensure adequate global tissue oxygenation in the setting of fluid-refractory shock. Specific decisions regarding the institution of hemodynamic support will be largely dictated by presentation. Low cardiac output is associated with mortality in pediatric patients, therefore, recommendations for optimization of cardiac index between 3.3–6 L/min/m2 is suggested for pediatric septic shock. Dopamine, dobutamine, or epinephrine are some of the vasopressor therapies, especially in the presence of cold shock. Epinephrine is used more frequently as first-line therapy in children compared with adults and is used preferentially over the other inotropic medications by some providers [21]. A recent randomized trial has shown that use of dopamine was associated with increased mortality compared to management with epinephrine [23]. For the presentation of warm shock, the use of continuous norepinephrine would be warranted [21]. In children, no mortality benefit has been observed with the use vasopressin or terlipressin in refractory shock [24].
The ACCM/PALS guidelines recommend targeting superior vena cava oxygenation at 70% or more for goal-directed care in order to ensure adequate oxygen delivery [21]. In a randomized clinical trial, patients treated with goal-directed therapies to maintain these superior vena cava oxygenation goals had both reduction in development of new organ dysfunction and mortality [25,26]. With this goal in mind, fluid resuscitation should remain ongoing, provided that signs of fluid overload have not developed. Signs of hypovolemia include increased pulse variation. After the first hour of resuscitation one should try to measure cardiac output and systemic vascular resistance as well as intra-vascular volume status to guide inotropes, vasopressors, and fluids as well as fluid removal. In addition, the use of inotropes may be indicated to achieve this goal. For example, the presence of a normal blood pressure but low superior vena cava oxygenation would suggest the need for milrinone, whereas low blood pressure with a low superior vena cava oxygenation would suggest the need for epinephrine. Packed red blood cells should be administered to maintain hemoglobin concentrations greater than 10 g/dL [21,25].
Relative adrenal insufficiency has been shown in vasoactive-resistant pediatric shock states [27,28]. Administration of hydrocortisone either via intermittent or continuous administration for patients who have vasoactive-resistant shock is included in the ACCM/PALS algorithm as well as the Surviving Sepsis Campaign [17,21]. However, there are some studies that suggest that hydrocortisone administration is not associated with improved outcomes [29–31]. Patients who typically receive hydrocortisone have a higher degree of illness severity and thus have worse outcomes and higher rates of mortality [29,32]. Further understanding of the role of hydrocortisone in pediatric sepsis necessitates an appropriate randomized clinical trial.
In the scenario of fluid- and vasoactive-resistant hypotension and profound septic shock, extracorporeal membrane oxygenation (ECMO) support is recommended by ACCM/PALS [21]. In an evaluation of the pediatric health-care information system (PHIS) database, approximately 4% of patients with pediatric severe sepsis required ECMO support. Use of ECMO in pediatric severe sepsis has increased over time, specifically in patients with dysfunction of more than two organ systems. Mortality in cases of pediatric severe sepsis requiring ECMO support has been estimated at 47.8% [33].
Antibiotic administration
The ACCM/PALS guidelines state that antibiotics should be administered within the first hour of clinical presentation [21]. A delay in timely antibiotic administration after the recognition of sepsis has been shown to be associated with increased mortality [34,35]. Once hypotension has manifested, every subsequent hour delay in antibiotic administration increased risk of mortality [36].
Empiric antibiotic choices require knowledge of a patient's individual risk factors, immunization status, previous antibiotic exposure, history of prior infections or potential colonization, and previous history of drug-resistant organisms. In addition, understanding the prevalence of different organisms within the community and any associated antibiotic resistance is imperative. Certain populations, such as solid organ transplant, hematopoietic stem cell transplant, and oncologic patients are at inherent risk for infections give their immunosuppressed state.
Age is an important consideration in any pediatric sepsis case because a previously healthy neonate is at risk for infection from different organisms than a healthy child or adolescent as noted above. Empiric treatment with ampicillin and gentamicin is most common in early- and late-onset neonatal sepsis. However, cefotaxime is used in place of gentamicin if there is concern for meningitis. Empiric coverage in critically ill pediatric patients involves treatment for both gram-negative and gram-positive organisms [14]. In our tertiary care center, we recommend use of vancomycin and zosyn or cefipime. Antibiotics are subsequently narrowed upon identification of causative organism with susceptibilities. Expert consultation with pediatric infectious disease may be warranted to guide narrowing of antibiotic regimen or appropriate coverage for multi-drug–resistant organisms.
Monitoring of Laboratory Values
Serial measurement of lactate has been used to evaluate the burden of the disease as an indicator of poor tissue perfusion and end-organ damage. However, because hypotension is often a late sign in pediatric patients with sepsis, an elevation in lactate may be notably delayed, even in cases of severe sepsis. Therefore, a low lactate should not be reassuring to a provider and aggressive management to reverse clinical shock states should still be used. If there is an elevated lactate upon presentation, this has been correlated to worse disease states in many studies. An elevated lactate measurement upon presentation in the emergency department has been shown to be associated with an increased risk for intensive care unit admission, need for vasoactive support, and organ dysfunction [37–39]. Some studies have also shown that elevated lactate concentrations upon hospital admission are associated with increased mortality [40–42].
Numerous other sepsis biomarkers have been studied within the pediatric population in order to predict risk and outcomes. The Pediatric Sepsis Biomarker Risk Model (PERSEVERE) study has been developed by Wong et al. [43] using a combination of five different serum biomarkers to provide a mechanism for risk-stratification in regards to mortality and illness severity. Both the breadth and importance of biomarker use for diagnostic and predictive indications in pediatric sepsis is understated as it is outside the scope of this review.
Illness Severity Scoring
There are several different severity of illness scores that can help providers understand the degree of presentation and assess risk for mortality based on values associated with respiratory, cardiovascular, metabolic and neurological presentation within the first hour of admission [41]. Pediatric Risk of Mortality (PRISM) and Pediatric Index of Mortality (PIM) scores have been used to predict overall severity of illness and risk for mortality. The Pediatric Logistic Organ Dysfunction (PELOD) score estimates the risk for multiple organ dysfunction syndrome (MODS) [44].
Multiple Organ Dysfunction Syndrome
Any organ can demonstrate dysfunction in pediatric severe sepsis and appropriate supportive therapies should be provided. Criteria for pediatric MODS remains ill-defined. In general, definitions for MODS involve dysfunction of two or more organ systems. Sepsis is estimated to be the most common cause of pediatric MODS. Studies estimate that upwards of 73% of children with pediatric sepsis have MODS and the risk for MODS is higher in neonates and infant. Overall, presence of MODS increases risk for mortality [45]. The presentation, pathophysiology, and treatment for specific end organ effects is beyond the scope of this article. However, it should be mentioned that several different adjunctive therapies, including the use of extracorporeal therapies, may be utilized to address the presence of organ dysfunction. For example, renal replacement therapy is common management for renal dysfunction and significant fluid overload. Thrombocytopenia associated multiple organ failure is another manifestation of pediatric sepsis not observed commonly in adults. It is a thrombotic microangiopathic syndrome with thrombocytopenia and multiple organ failure. Plasma exchange can remove ultra large von Willebrand factor multimers that attract platelets and fibrin forming microthrombin [33,46–50]. Extracorporeal membrane oxygenation support was higher in patients with MODS (approximately 10% of patients) [33].
Bundles and Triage Protocols
Patients managed within the guideline recommendations have decreased length of stay and mortality, however, there are inconsistencies with recognition of sepsis and guideline implementation [51–53]. Therefore, pediatric emergency department providers have developed triage tools based on age-specific clinical criteria to facilitate early identification of pediatric sepsis. Such protocols have demonstrated an increase in guideline compliance resulting in more timely initial fluid administration and early antibiotic administration [54–56]. Likewise, implementation of pediatric sepsis pathways have been developed for inpatient medical and surgical floors in order to facilitate earlier identification and evaluation of potential septic patients [57].
The ACCM/PALS 2014 guidelines proposed a set of “bundles” to assist in the early recognition and management of pediatric sepsis patients. These include separate recognition, resuscitation, stabilization, and management bundles. The recognition bundle focuses on the need for various screening tools that allow for rapid identification of sepsis. The resuscitation bundle focuses on establishment of early intravenous access, beginning fluid resuscitation within the first 30 minutes, administration of antibiotic agents within the first hour, and initiation of inotropes in states of fluid-refractory shock within the first hour. A focus on monitoring, goal-directed therapies and source control occurs within the stabilization bundle. Finally, the performance bundle suggests the use of quality improvement measures in order to assess adherence to guidelines and identify barriers to successful implementation [21].
Guidelines for early recognition and treatment in sepsis have been the focus of many recent health care policy initiatives. However, there are several reservations about these mandates because they may not allow for adjustments to guidelines based on new scientific findings and do not allow for use of physician judgment when necessary to deviate from protocols. More studies are needed to focus on the implications of health policies as they relate to such guidelines [58].
Outcomes
The need for early recognition and rapid initiation of treatment is well documented for both adult and pediatric patients. Adult sepsis mortality rates are reduced from 50% to 10% when resuscitation and antibiotic administration was completed in 90 minutes instead of 3 hours [59,60]. Similarly, in pediatrics, every hour that passes without adequate resuscitation increases mortality by 40% [22,34]. Children with either prolonged capillary refill or hypotension experience a 5%–7% mortality, and mortality increases to 30% when both are present [61]. If the shock state can be reversed in the emergency department, the mortality reduces two-fold, whereas early goal-directed therapy over the first 72 hours has reduced mortality in children from 40% to 12% [25]. Overall, mortality for severe sepsis in pediatric patients remains significantly lower than that observed in adult patients (10%–20% vs. 35%–50%, respectively) [3,12].
Transfer to a Pediatric Tertiary Care Center
Most pediatric patients with sepsis will first present to adult care facilities. Because early recognition and the initiation of adequate resuscitation and antibiotic therapy is so crucial to survival, widespread appreciation for the subtleties of pediatric disease is crucial. For children who necessitate vasoactive medications or have evidence of multi-system involvement, early and rapid transfer to a tertiary care center staffed with pediatric critical care medicine physicians should be initiated. In addition, early transfer of patients with significant comorbidities, e.g., immunosuppression, long-term disability, congenital heart disease, or chronic lung disease, should be considered for early transfer because of unique aspects of their care and greater risk for poor outcomes.
Conclusion
Sepsis is the leading cause of death worldwide for children. Overall incidence continues to increase, however, mortality has dramatically decreased in recent years with increased recognition and adherence to best practice sepsis guidelines focused on early recognition and initiation of resuscitation. Children with evolving sepsis present unique physiologic challenges for caregivers, especially with regard to hemodynamic support compared with adults. The first hour of care is crucial to survival and subsequent transfer to a tertiary pediatric center is recommended for higher level of management. Further research is still needed to refine the definition of sepsis and optimize hemodynamic and multiple organ failure support.
Footnotes
Author Disclosure Statement
No competing financial interests exist.