
Abstract
Abstract
Background:
Chronic osteomyelitis associated with a stage IV decubitus ulcer is a challenging condition to manage, characterized by frequent relapses and need for long-term anti-microbial therapy. Although gram-positive cocci are the most common causes, fungal infections have been reported, usually in immunocompromised hosts. We present a case of Cladophialophora osteomyelitis in a patient without known immunocompromised that was managed with a Girdlestone pseudoarthroplasty.
Case Report:
A 70-year-old male presented to our emergency room with fever, right hip pain, and purulent drainage from a right greater trochanter stage IV decubitus ulcer. His medical history was significant for T10 paraplegia secondary to spinal ependymomas and multiple spinal procedures, as well as significant recent weight loss. Past operations included multiple spinal procedures and repair of a right intertrochanteric femoral fracture with a plate and lateral compression screws. This led to post-operative decubitus ulcer formation over the right greater trochanter, requiring a gracilis flap. The flap remained intact for three years, then re-ulcerated. He subsequently developed femoral head osteomyelitis. To facilitate the treatment, the hardware was removed three weeks prior to presentation. With evidence of worsening osteomyelitis and a new soft-tissue infection, a Girdlestone procedure was performed. Intra-operatively, he was noted to have a pathological intertrochanteric fracture. Soft-tissue cultures yielded Pseudomonas aeruginosa; bone cultures grew Streptococcus dysgalactiae and Cladophialophora spp. Post-operatively, his wound was managed with negative pressure wound therapy with instillation and dwell (NPWTi-d). Delayed primary closure over a drain and topical negative pressure was done four days later. His course was uneventful, and he was discharged six days later. At his four-month follow-up, the wound was completely healed.
Conclusion:
Invasive fungal infections are rare in immunocompetent individuals. Cladophialophora osteomyelitis has been found in immunocompromised individuals with concomitant cerebral abscesses. To our knowledge, this is the first case of osteomyelitis without previously known immunocompromise.
O
The most common pathogens involved in osteomyelitis are the Staphylococcus species and gram-negative bacteria such as Pseudomonas and Salmonella, although the latter are found more often in specific populations [1]. Fungal causes of osteomyelitis are rare, generally appearing in the setting of immunodeficiency or immunosuppression. Candida and Aspergillus are the most common organisms and usually require aggressive surgical and medical management [3].
Rare fungi, such as Cladophialophora, also can cause osteomyelitis. However, these infections have been documented only in patients with known immunosuppression, such as renal transplant recipients, and have required aggressive surgical debridement and even amputation, along with intensive anti-fungal therapy [4]. Although fungal osteomyelitis has been reported in immunocompetent patients, Cladophialophora osteomyelitis has not.
We present the first identified case of Cladophialophora osteomyelitis in a patient without any previously known immunocompromise that was managed with a Girdlestone pseudoarthroplasty.
Case Report
A 70-year-old male with a history of T10 paraplegia secondary to multiple spinal procedures for spinal ependymomas and a right hip fracture repaired with lateral plate fixation and dynamic compression screws presented to our service with a chronic wound caused by decubitus ulcers over his right greater trochanter. This wound had been treated multiple times over 2014–2017 without success. The last attempt was a right gracilis flap; although this lasted for three years, he eventually developed ulcerations over the greater trochanter that worsened over a period of months. Subsequently, the patient developed osteomyelitis of the femoral head. His right hip hardware was removed three weeks prior to admission revealing evident progression of his infection. He also had a weight loss of 11 kg over two years, resulting in a body mass index of 18 kg/m2. He denied any history of sickle-cell anemia, diabetes, recent trauma, known immunocompromise, or use of immunosuppressant drugs.
On presentation to the emergency department, he was febrile (39°C) and tachycardic (approximately 120 beats/min). His serum lactate concentration was normal. Computed tomography (CT) showed phlegmonous changes in the right thigh raising concern about necrotizing muscular infection and chronic necrotic bone in the right femur (Fig. 1). Given the concern about sepsis, he was started on intravenous (IV) cefazolin, IV vancomycin, IV cefepime, and IV metronidazole, which were changed to IV metronidazole, IV vancomycin, and IV piperacillin/tazobactam on the day of admission. Blood cultures showed no growth. Because of his failure to improve, it was decided to take him to the operating room for a Girdlestone pseudoarthroplasty to remove his necrotic bone completely and drain his acetabulum.
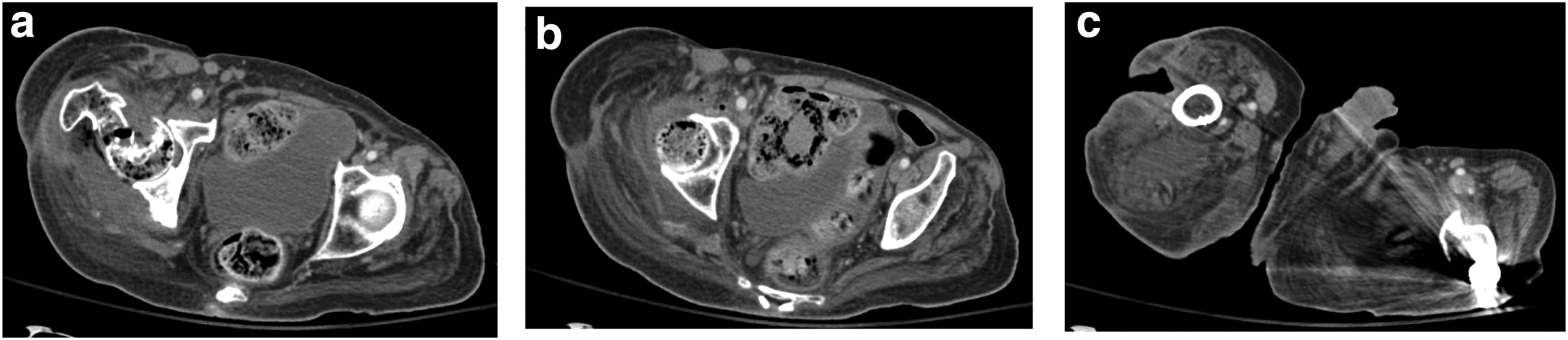
Computed tomography images showing (
Intra-operatively, he was found to have a right intertrochanteric femoral-neck fracture with grossly necrotic and purulent bone. His femoral head was then removed at the fracture site. The wound was debrided of surrounding necrotic tissue and cleaned with chlorhexidine and dilute hydrogen peroxide. Negative-pressure wound therapy with instillation and dwell (NPWTi-d) was applied post-operatively. His sacral wound was dressed with Dakin's solutions-imbued dressings. Intra-operative bone culture yielded S. dysgalactiae and Cladophialophora spp., and his sacral wound grew Pseudomonas aeruginosa. On post-operative day 4, his wound was closed over a 19F Blake drain with an incisional negative-pressure wound device applied. He remained in the hospital for a further three days on fluconazole and vancomycin therapy, at which point, he was placed on fluconazole and ertapenem. He was discharged to a skilled nursing facility 10 days after his initial Girdlestone procedure.
The patient continued his fluconazole therapy until his two-week follow-up and continued on his ertapenem until his one-month follow-up. His wounds made slow but encouraging progress throughout his post-operative course. At his four-month follow-up, the wound was healed (Fig. 2).

Healing of wound.
Discussion
Osteomyelitis is a severe infectious process that normally needs long-term antibiotic administration and potential debridement. This is most commonly a bacterial infection; fungal infections generally are seen only in the immunocompromised patient. Most osteomyelitis requires intensive IV medication. Some patients may need surgical debridement. To prevent serious complications such as pathologic fractures, cancers, and sepsis, early recognition and prompt intervention are critical [2, 5]. Pathogens such as Pseudomonas or fungi usually are considered only in patients with risk factors such as known immunocompromise, including iatrogenic causes, infections, and diabetes.
The fungal infection in this patient was caused by Cladophialophora, a black yeast-like fungus found in soil, wood, and decomposing plant debris, especially in tropical and subtropical environments. It can cause infections ranging from a mild skin infection to severe sinusitis and fatal encephalitis, including chromoblastomycosis [6]. Rarely, it causes osteomyelitis and endocarditis, but data discussing these instances are limited. Generally, Cladophialophora infections are managed with aggressive anti-fungal therapy and surgical debridement, if possible. Unfortunately, guidelines for the management of this and other fungal infections are lacking [7].
Although no formal guidelines exist for the management of fungal osteomyelitis, general principles used in management of these types of infections include aggressive surgical debridement to achieve source control, which remains the single most important step, and anti-fungal coverage [3]. Any associated hardware should be removed, as foreign bodies are niduses of joint infections. Some patients require amputation as well as intensive anti-fungal therapy.
In this patient, source control was achieved with the Girdlestone procedure, originally developed for septic arthritis of the hip caused by Mycobacterium tuberculosis [8] and maintained with negative-pressure therapy combined with instillation, which serves as an adjunct to surgery in removing devitalized tissue and improves rates of granulation [9,10]. This allowed delayed primary wound closure. Importantly, this patient did not require any dedicated anti-fungal therapy per the recommendation from the infectious diseases team and has been healing appropriately.
The question of why this patient had the Cladophialophora infection remains. He had no known immunocompromise, which is the main risk factor for this infection. We hypothesize that his immune system, although intact, did not function at full strength because of malnutrition. Poor nutrition is known to worsen immune function. A lack of appropriate protein and energy diminishes the competence of cell-mediated immunity, especially T–cell-mediated cytokine production [11,12]. As T-cells are the main defense against fungal infections, a weakened T-cell response could allow Cladophialophora osteomyelitis. The presence of the intertrochanteric hardware coupled with the ulceration of the ischium on the same side as the osteomyelitis likely played a role as well. Although this patient likely had multiple causes for his weight loss, his chronic infection probably contributed. Because of his persistently elevated immune response, this patient probably was in a hypercatabolic state, leading to malnutrition and poor immune function, which impaired T-cell function and predisposed him to this fungal infection.
In conclusion, we present the first case to our knowledge of Cladophialophora osteomyelitis in a patient without known immunocompromise. This infection was well managed with the Girdlestone procedure and negative-pressure and instillation therapy with delayed primary closure and closed drainage, requiring only minimal anti-fungal drugs. Although this infection has been seen previously only in immunocompromised patients, we hypothesize that the chronic osteomyelitis in this patient, which caused weight loss and a low BMI, as well as a prior injury with hardware and decubitus ulceration, could have led to an impaired immune system predisposing him to this infection.
Footnotes
Author Disclosure Statement
The authors of this manuscript have nothing to disclose.