
Abstract
Abstract
Background:
Surgical infections are a major cause of morbidity and mortality in low- and middle-income countries (LMICs). Inadequately reprocessed surgical instruments can be a vector for pathogens. Little has been published on the current state of surgical instrument reprocessing in LMICs.
Methods:
We performed a scoping review of English-language articles in PubMed, Web of Science, and Google Scholar databases describing current methods, policies, and barriers to surgical instrument reprocessing in LMICs. We conducted qualitative analysis of all studies to categorize existing practices and barriers to successful surgical instrument reprocessing. Barriers were non-exclusively categorized by theme: training/education, resource availability, environment, and policies/procedures. Studies associating surgical infections with existing practices were separately evaluated to assess this relationship.
Results:
Nine hundred seventy-two abstracts were identified. Forty studies met criteria for qualitative analysis and three studies associated patient outcomes with surgical instrument reprocessing. Most studies (n = 28, 70%) discussed institution-specific policies/procedures; half discussed shortcomings in staff training. Sterilization (n = 38, 95%), verification of sterilization (n = 19, 48%), and instrument cleaning and decontamination (n = 16, 40%) were the most common instrument reprocessing practices examined. Poor resource availability and the lack of effective education/training and appropriate policies/procedures were cited as the common barriers. Of the case series investigating surgical instrument reprocessing with patient outcomes, improperly cleaned and sterilized neurosurgical instruments and contaminated rinse water were linked to Pseudomonas aeruginosa ventriculitis and Mycobacterium port site infections, respectively.
Conclusions:
Large gaps exist between instrument reprocessing practices in LMICs and recommended policies/procedures. Identified areas for improvement include instrument cleaning and decontamination, sterilization aspects of instrument reprocessing, and verification of sterilization. Education and training of staff responsible for reprocessing instruments and realistic, defined policies and procedures are critical, and lend themselves to improvement interventions.
A
Standards for instrument reprocessing are defined in HICs, with well-established training systems for central sterile supply departments (CSSD) [9,10]. Numerous steps exist in the CSSD for instrument reprocessing, including a one-way flow for soiled items through cleaning and decontamination; inspection and packaging; sterilization and sterile storage. The end result of this process should be complete instrument sets terminally sterilized and ready for use during surgery. Final peri-operative verification of sterilization is compulsory in the World Health Organization (WHO) Surgical Safety Checklist [11] using proper physical, chemical, and biologic indicators [12,13]. Unfortunately, these confirmatory markers are often lacking in LMICs with potential for poor compliance given numerous consecutive steps that must occur in the CSSD for surgical instrument reprocessing [14]. Despite the importance, little is published on the current barriers to instrument reprocessing in LMICs, a fundamental component of safe surgical care. Providing sterile surgical instruments through reprocessing requires applicable guidelines and policies, relevant training, and ongoing monitoring to ensure compliance. Our study explores the current status of surgical instrument reprocessing in LMICs and categorizes documented barriers to proper implementation of current guidelines for safe practices. Our goal was to identify areas for further financial and human capacity investment.
Methods
We performed a scoping review of existing literature describing current methods, guidelines, and barriers to surgical instrument reprocessing in LMICs. A scoping review is a method to map the literature on a specific topic or research area to identify key concepts; knowledge gaps; and types and sources of evidence to inform practice, policymaking, and research [15]. This was ineligible for registration in the Prospero database because it is a scoping review, however, we used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines to direct the work. PubMed, Web of Science, and Google Scholar databases were searched for articles published in English using the keywords and search strategy described in Appendix 1 (Appendix 1 is available online at www.liebertpub.com/sur), with the countries included in the search terms recognized as low- or middle-income countries by standard criteria [16]. All studies published between January 1983 and September 2017, identified through our search criteria, were included for initial review to ensure capture of relevant studies.
Titles and abstracts from all three databases were screened for duplicates and reviewed for relevance prior to obtaining full text manuscripts. Eligible articles were independently reviewed by two reviewers (J.A.F. and B.L.P.), who evaluated study location, type of study, number of facilities or participants in study, a discussion of policy/procedure for instrument reprocessing, areas of CSSD discussed, barriers to CSSD, methods for surgical instrument reprocessing, enzymatic detergent availability, instrument repair/maintenance availability, distilled/purified water availability, biomedical engineering availability, and autoclave repair/maintenance availability. Additional recorded parameters included study duration, type of study, sample size, gender, age of patient, microbiologic profile, and morbidity and mortality of infection. Disagreement between reviewers was resolved through discussion with a third reviewer (J.D.F.). Exclusion criteria included abstracts without available full text, studies of reusable or explanted items or endoscopes, and those with no discussion of surgical instrument decontamination or sterilization. Additional studies were sought by examining the bibliographies of all studies identified during the search process.
Central sterile supply departments were divided into three areas: workforce, workspace, and reprocessing practices. Reprocessing practices were subdivided into eight components: infrastructure environment, cleaning and decontamination, inspection and assembly, packaging, sterilization, storage, transportation, and verification of sterilization. Barriers to performance in the areas of CSSD were independently categorized a priori non-exclusively by theme into groups (education/training, resource availability, environment, lack of policies/procedures, and other) for analysis by two of the authors, with differences resolved by discussion. For the quantitative analysis, we did not set a minimum sample size, because we did not expect to find a large number of articles. Microsoft Excel (Microsoft 2013, Redmond, WA) was used to calculate descriptive statistics. As all articles were publicly available, we did not submit this for Institutional Review Board (IRB) review.
Results
The initial database search identified 972 abstracts (Fig. 1). After screening, complete articles were obtained for 74 papers (8% of total). Of these, 34 were excluded for the following reasons: no inclusion of surgical instruments (n = 20), primary focus on re-use of explanted or single use devices (n = 8), primary focus on endoscopic equipment (n = 4), primary focus on an HIC (n = 2). Forty studies met inclusion and exclusion criteria and were included in the qualitative analysis (Table 1).
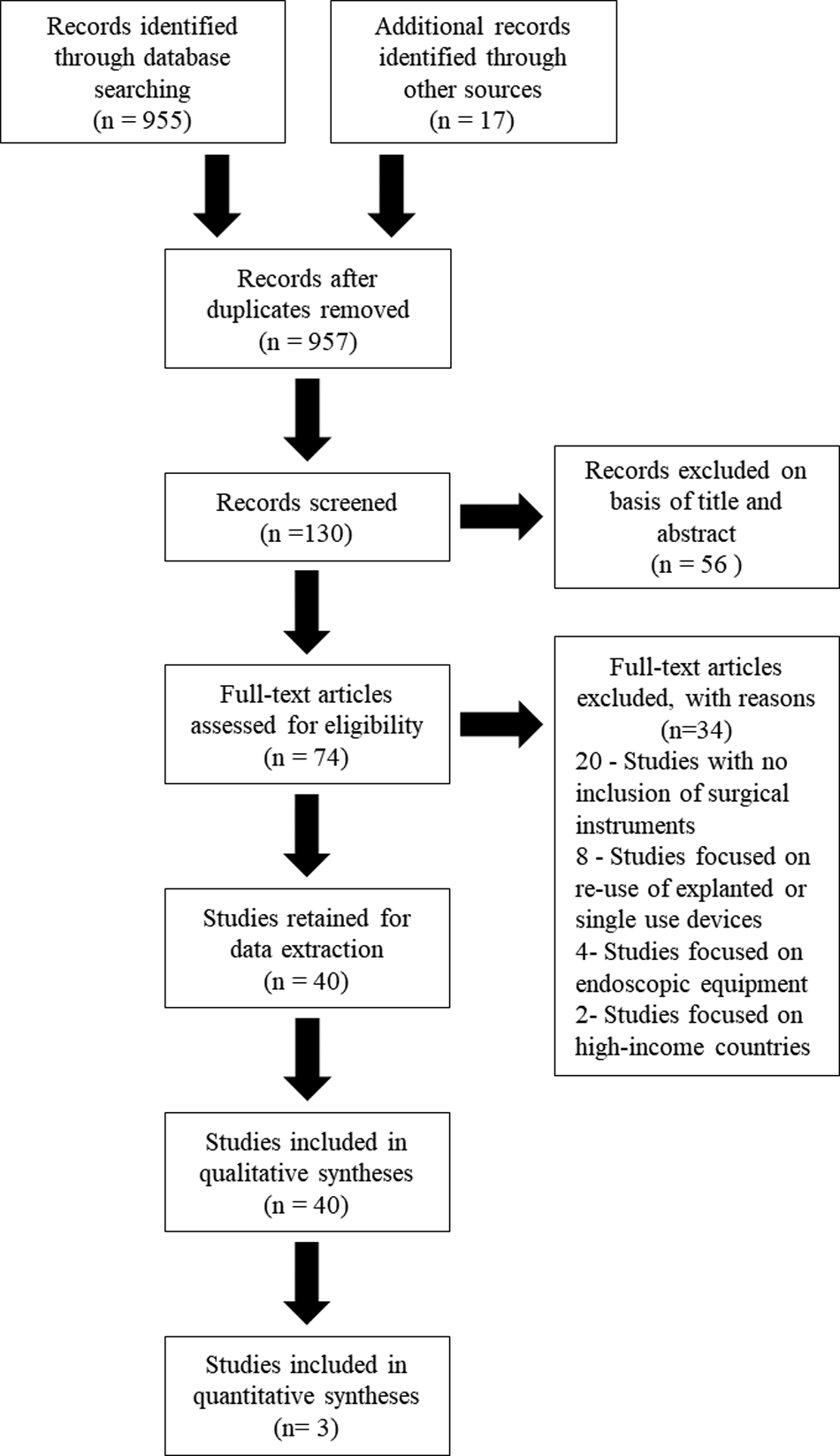
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flowsheet of article selection process.
WHO = World Health Organization.
The majority of included studies were cross-sectional (n = 15, 38%), editorials, opinions, or ideas (n = 12, 30%), and laboratory/field experiments (n = 8, 20%). Commonly represented WHO regions included Southeast Asian countries (n = 15, 38%), African countries (n = 6, 15%), and equal distribution across the Eastern Mediterranean, Americas, and a combination of regions (n = 5, 13% each). Six hundred forty-one hospitals were represented, with 13 (33%) articles reporting data from a single institution, 11 (28%) articles reporting data from multiple institutions.
Most studies (70%) discussed specific policies and procedures for surgical instrument reprocessing, noting shortfalls in either the trained workforce or existing workspace because of poor training/education, decrepit surgical environment, and a lack of resources (Table 2). The most common areas examined within reprocessing practices included instrument cleaning and decontamination, sterilization, and verification of sterilization. Of the 16 studies (40%) examining cleaning and decontamination, surgical instrument repair/maintenance (n = 3, 7.5%) was seldom discussed as was enzymatic detergent (n = 6, 15%). Sterilization was mentioned in 38 studies (95%) with common methods including steam-powered autoclaves in 37 studies (93%) and “other” in 23 studies (58%). Boiling of instruments (n = 9, 23%) represented the majority of the “other” category with ethylene oxide the next most common (n = 5, 13%). Distilled and/or purified water was discussed in nine studies (23%), autoclave repair or maintenance examined in seven studies (17.5%), and biomedical engineering mentioned in only one (2.5%). Of the 19 studies (48%) examining methods for verification of sterilization, biologic indicators (n = 17, 85%), chemical indicators (n = 17, 85%), and physical indicators (n = 14, 70%) were examined in similar proportions.
Non-exclusive.
Seventy-five separate barriers to reprocessing practices were discussed in 34 studies (85%; Table 2). The current infrastructural environment was cited by nine studies (23%) as presenting challenges to appropriate instrument reprocessing, citing the potential for cross-contamination because of poorly designed workflow and spatial congestion [17–21]. Within instrument reprocessing practices, cleaning and decontamination, sterilization, and verification of sterilization were three specific focus areas. Cleaning and decontamination barriers were largely attributed to poor existing training/education systems and lack of appropriate resources such as consumables, detergents, and lubricants. Barriers to sterilization included both poor resource availability, such as the lack of reliable electricity, running water, and functional donated equipment, as well as the lack of appropriate training/education. Barriers to verification of sterilization were largely credited to poor resource availability of consumables, such as proper sterile indicators, and poor existing training/education. Six studies (15%) revealed that the surgical providers' lack of appropriate knowledge-base on infection prevention was a substantial barrier [17,18,22–25].
Three (7.5%) of the 40 studies investigated surgical instrument reprocessing to patient outcomes (Table 3). All studies were case series, two of which described patients with post-operative infections attributed to inappropriate instrument reprocessing. The first of these described a series of five male patients with medulloblastoma post-operatively diagnosed with Pseudomonas aeruginosa ventriculitis (cerebrospinal fluid culture-positive) because of improperly cleaned and sterilized surgical aspirators, resulting in a 20% (n = 1) mortality rate. The other of these described a series of 145 laparoscopic port-site infections because of Mycobacterium chelonae in 35 patients undergoing laparoscopy, with the rinse water used for washing chemically disinfected instruments as the causative agent. All patients recovered with varying lengths of antimicrobial therapy (2–18 months). The third case series described the experience of a short-course (18 days) emergency orthopedic trauma surgical center in Nepal after an earthquake. Twenty-seven patients requiring 30 orthopedic operations were included. Surveillance was limited: seven patients were discharged (hospital length-of-stay: mean, 9 days [8–13 days]) and 20 patients were transferred to the government hospital by the end of their study period.
NA = not applicable.
Discussion
In our review of the past 35 years of literature on surgical instrument reprocessing in LMICs, only 40 studies had sufficient scope for qualitative analysis. Surgical instrument reprocessing is a complicated procedure and requires training, infrastructure, supplies, and strong organizational principles to be successful. Barriers in LMICs included poorly defined instrument reprocessing policies and procedures, inappropriate staff training, and limited resources. Some shortfalls such as with training and education may be feasibly addressed, others such as sterilization infrastructure may be more challenging. Yet these shortfalls need to be overcome, as failure place both the patient and healthcare workers at risk [26].
Achieving proper compliance with sterility requires a trained workforce in a functional and appropriate workspace, underpinned by robust and contextually-relevant policies and procedures. The workspace component of CSSD is addressed through standard recommendations, including the one-way flow using infrastructural layouts separating decontamination, sterilization, and sterile storage, ideally in separate rooms [27]. A trained workforce is established in HICs through extensive on-the-job training as well as ongoing certification to verify achievement of required skills [28,29]. Unfortunately, both the workspace and workforce are lacking in many LMICs, and few organizations exist to help improve the situation. One example is the Sterile Processing Education Charitable Trust [30], which provides staff training for surgical instrument reprocessing. Sterile Processing Education Charitable Trust (SPECT) emphasizes the crucial role that sterile processing staff play in supporting surgical capacity and safety through instruction on microbiology, infection prevention principles, effective cleaning and disinfection practices, surgical instrument inspection, aseptic packaging techniques, and sterilization methods. Along with classroom instruction, SPECT also works with sterile processing staff in their respective departments to ensure that contextual best practices are applied. In-country knowledge of existing resources are essential to adapt reprocessing principles into feasible, local, and sustainable solutions.
Cleaning instruments, killing residual microbes through sterilization, and verifying effective process completion are requisite for sterile surgical instrument provision. Cleaning and decontamination are vital upstream steps; if done properly, they can alone remove 99% of micro-organisms [14,19]. Typically, cleaning involves physical manual scrubbing with or without additional mechanized methods. To safely and efficiently remove gross biosoil, trained staff must use appropriate brushes, enzymatic detergents, and distilled/deionized water [31]. Enzymatic detergent is the gold standard as it contains varying combinations of amylases, proteases, lipases, and surfactant to remove the proteinaceous material remaining after surgery [32]. The instruments are then rinsed in distilled/deionized water to remove residual detergent, which can be corrosive [5]. The development of a detergent specifically made for cleaning surgical instruments, which could be manufactured in-country following instructions akin to the WHO alcohol-hand gel recipe [33], could potentially be a powerful method for providing a key missing resource in LMICs. To our knowledge, only one company in Madagascar has manufactured this type of detergent to date [19,34].
In LMICs, staff are frequently undertrained, and when training does occur, it can perpetuate implementation of outdated infection prevention guidelines [17,19,20,39,40]. The WHO recently updated its guidelines for surgical instrument reprocessing [9] and SSI prevention [5], recommending against the use of corrosive chlorine-containing agents, such as bleach, which historically has been used for decontamination. The reliance on bleach, inappropriate brushes, and infrequent use of proper detergents and distilled/deionized water can lead to accelerated instrument corrosion and potential inadequate pathogen destruction [19]. The lack of instrument maintenance and repair capabilities, combined with these resource and training limitations, can decrease the lifetime of surgical instruments, placing strains on functional inventory and likely surgical capacity. Implementing updated guidelines cognizant of these resource limitations through focused and frequent trainings on proper cleaning and decontamination may be high-yield, low-cost interventions for healthcare facilities in resource-constrained settings.
After cleaning, instruments are sterilized to kill any potentially remaining micro-organisms. In our review, sterilization was most frequently performed by electrically powered steam autoclaves but few studies made explicit mention of how frequently their devices were functioning. These autoclaves are dependent upon water for steam generation and electricity for powering, both of which are notably unreliable in LMICs [35–37]. Together with shortages of trained technicians to perform equipment maintenance [26], these resource issues can lead to functional machines becoming gradually unfit for use [38]. For example, distilled or deionized water is essential for steam supplied autoclaves to prevent corrosion of the autoclave, sediment clogged filters, and mineral deposition on surgical instruments [32]. Autoclaves, especially the donated variety used in many LMICs, are prone to breakdown and require regular upkeep. Distilled or deionized water was documented infrequently in the reviewed studies. The development of viable and low-cost method for generating distilled/deionized water may substantially decrease autoclave breakdown, in turn strengthening instrument sterilization processes.
Other methods of sterilization discussed less frequently included chemical and dry heat sterilization, boiling of instruments, and the use of ethylene oxide (ETO) gas. Whereas boiling is one method of high-level disinfection, it can only be used on certain instruments or materials without damaging them and does not destroy endospores [10]. The WHO explicitly states that boiling is an unacceptable sterilization method for instruments and should not be used [9]. Ethylene oxide is a useful but more expensive method of low-temperature sterilization, requiring sophisticated equipment with prolonged cycle times and well-trained staff [10]. These other sterilization methods examined in the literature are often utilized inappropriately and can lead to poor overall compliance.
Verification of sterilization is the confirmatory step in instrument reprocessing to ensure overall process compliance, yet it was examined by less than half of studies. Despite obvious resource limitations, a commonly reported barrier to verification was the lack of knowledge by surgical providers in LMICs on best practices. A comprehensive discussion on verification methods is beyond the scope of this review; however, it is prudent to discuss the applicable details to improve understanding and identify opportune areas for creative solutions.
Typically a series of indicators are used to verify whether instruments have been exposed to the correct parameters for killing pathogens [31]. Physical, chemical, and biologic indicators are used in steam sterilization to ensure adherence with defined minimums of temperature, pressure, and time [32]. Electronic tracking or logbooks can be used for recording compliance with the physical indicators of temperature and pressure. Chemical indicators are placed both outside and inside a package, each with different stringency to sterilization parameters indicated. A piece of chemical sterile indicator tape (class I) is placed on the outside of a package to visually indicate whether or not it has proceeded through the sterilization step [31]. These class I chemical indicators visually change after exposure to high temperatures alone. A different class of chemical indicators (class V) are placed inside every package, visually changing when exposed to the correct temperature and pressure for the mandatory time [31]. Verification of sterility by the internal indicator, as highlighted by the WHO Surgical Safety Checklist [11], occurs in the operating room after the package is opened and before using the instruments for surgery. Biological indicators contain spores of bacteria and are the gold standard for confirming functional sterilization in HICs [31]. They can be cultured or analyzed through advanced technology to demonstrate successful killing of the microbe when all correct parameters have been achieved following terminal sterilization [9].
In LMICs, verification of sterility is lacking with obvious resource gaps for proper indicators. Physical indicators, such as functioning gauges for temperature and pressure, can be missing or inaccurate [38] and biologic indicators are largely unobtainable. If available, chemical sterile indicator tape (class I) is generally the only existing potential method for verification in LMICs [19,41]. In a survey of 20 health facilities across India, only 65% had class I chemical indicators available [40]. Adherence to verification of sterilization processes must be improved. In lieu of large resource deficits, developing novel, affordable, or reusable sterilization indicators may be a useful addition to the sterilization armamentarium in LMICs.
Limitations
Most articles provided limited data on specific practice pattern shortfalls and many did not assess their association with patient outcomes. However, international guidelines for surgical instrument reprocessing are well-established [9,31] and small case series [42,43] emphasize that poor compliance can impact overall surgical quality. The generalizability of the findings could potentially be limited because of the majority of studies (67.5%) set in urban areas and only 18% of LMICs represented in the full-text articles. However, these findings provide an important baseline and thematic analysis to guide future work given the paucity of previous research on this aspect of essential surgical care. There may be selection bias represented by survey studies of provider practices: those providers with more limited instrument reprocessing procedures may opt out of responding to the surveys, skewing the results in a more favorable light.
Whereas innovative and affordable solutions may provide context-appropriate adaptations contributing to safer surgical delivery in the immediate term, they represent only interim solutions. Short-term surgical missions, such as that of Zheng et al. [63], demonstrate that even in high-risk environments iatrogenic infections from breaks in sterile technique can be minimized with careful planning and attention to detail. However, these limited engagements frequently do not reflect the existing surgical infrastructure in LMICs. Limitations on sterile processing will only be permanently solved by substantial investment in systematic infrastructural improvements and comprehensive staff training. Performance of a CSSD department within a health facility can serve as a benchmark for both assessing and strengthening service delivery. One example of a comprehensive CSSD in this scoping review was the Tata Medical Center, a specialized cancer hospital in Kolkata, India. Five studies [44–48] fitting the criteria for our review were published by the team there, offering a unique perspective into a facility that has invested in and sustained the implementation of, and advocacy for, proper instrument reprocessing practices.
Conclusion
Surgical instrument reprocessing is an essential service requisite for safe surgery that must be emphasized in the expansion of emergency and essential surgical services in LMICs. This scoping review found that the lack of contextually relevant guidelines, effective staff training, and appropriate resources created substantial barriers to appropriately reprocessing surgical instruments. Addressing key resource limitations through creative design, such as locally manufactured enzymatic detergent, onsite generation of distilled/deionized water, and reusable sterility indicators, are opportunities for potential disruptive innovation. Contextually relevant education and training of sterile processing staff and realistic, defined policies and procedures are critical, lending themselves to improvement interventions. Additional research and advocacy is needed for promoting surgical instrument reprocessing to strengthen the safety of surgery globally.
Footnotes
Acknowledgments
We want to acknowledge and thank Christopher Stave for his help generating the search terms and Chelsey Thomas for her expertise and guidance with surgical instrument reprocessing practices in high-resource settings.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.