
Abstract
Abstract
Background:
We sought to evaluate the practice of double gloving among surgeons and to determine the factors that affect compliance with such practice at King Abdulaziz University Hospital (KAUH).
Methods:
A survey was conducted among surgeons in active training from all departments at KAUH through the use of a questionnaire from May through July 2017.
Results:
Of the 220 surgeons who worked at KAUH, 183 agreed to participate in the study for a response rate of 83.2%. Less than half of the respondents (44.3%) stated that they wear double gloves. The main reason for wearing them was “self-protection” (63%), whereas the main reason for not wearing them was that they “think it is required only for special cases” (62.7%). The association between wearing double gloves and the subspecialty was significant (p = 0.033), the highest rate being found among orthopedic surgeons. Among those who usually double glove 84% of needle-prick injuries occurred when they were not double gloved. Eighty percent of needle-prick injuries occurred while surgeons were wearing single gloves.
Conclusions:
Less than half of the respondents practice double gloving, the main reason being self-protection. The most common reason for not wearing them was that they are required only for special cases. There was notable association between wearing double gloves and orthopedic surgery. Most needle-prick injuries occurred while wearing single gloves. We believe increasing awareness of the benefits of double gloving might change the practice.
S
To decrease the potential of acquiring infections, surgeons should wear sterilized gloves in the operating room even after performing hand scrubbing. Glove perforations can, however, compromise these efforts by transmitting harmful pathogens such as hepatitis B (HPB), hepatitis C (HPC), and human immunodeficiency virus (HIV) through blood contamination. Glove perforations are common and have been studied in different types of surgeries [2–4]. A randomized study of 66 consecutive surgical procedures showed that most glove perforations (83.3%) went unnoticed [5]. The Cochrane Review found that during standard double gloving, glove wearers detect only 25% of glove perforations while 74% of perforations are detected when wearing glove indication systems [6]. In addition, exposure to needle-prick injuries has been associated with a high economic burden, some studies reporting a cost of approximately $600 U.S. per needle-prick injury for follow-up after exposure and of approximately $3,000 U.S. for prophylactic treatment [7,8].
Many studies have recently tested double-gloving protection, showing that double versus single gloving during surgery decreases perforations and blood contact with the skin, thus reducing needle-prick injuries [3]. A randomized controlled trial provided evidence that suggested a protective effect with double gloving of more than 90% for both patients and surgeons [4].
Although double-gloving effectiveness has been documented and adopted by a number of health care authorities worldwide and many studies have been done on the subject, surgeons' compliance with this practice is still limited [9]. A study performed in two teaching hospitals (Western Ontario University and McMaster University Hospitals) reported that less than half of the surgeons and residents wore double gloves as routine practice to protect themselves from the harm of needle-prick injuries [9]. The lack of compliance by surgeons working in university hospitals may be transmitted to future generations, as medical students consider surgeons and residents to be role models with a powerful effect on their careers. Thus, surgical faculty members should pay attention to their influence on these students [10].
Because few studies have explored the factors that affect surgeons' practice of double gloving, we sought to evaluate this practice among surgeons and to determine the factors that affect compliance with this practice at King Abdulaziz University Hospital (KAUH), Jeddah, Saudi Arabia.
Methods
This cross-sectional study was conducted among surgical consultants, specialists, and residents in training at KAUH in all surgical departments from May through July 2017. An anonymous voluntary self-reported questionnaire was distributed to surgeons in operating rooms, wards, and clinics to cover most surgical staff in all subspecialties.
Before administering the survey, we pilot tested the questionnaire among five team members to assess the face validity, clarity, and sequence of items. The demographics and data collected on the questionnaire, which took up to three minutes to complete, included position, subspecialty, age, gender, number of operating room cases done per week, practice and frequency of double gloving, factors that affected compliance, and history of needle-prick injury.
Approval for the study was received from the KAUH ethics review committees. Statistical analysis included descriptive analysis and χ2 tests with the use of SPSS software (version 23, IBM, Armonk, NY).
Results
Of the 220 surgeons working at our institution, 183 agreed to participate in the survey and filled out the questionnaire completely, resulting in a response rate of 83.2%. Among these participants, 72.1% were male, 40.4% were younger than 30 years of age, and 30.6% were between 30 and 40 years. Half of them were residents. More than one quarter (26.8%) were from general surgery, followed by gynecology (21.3%) and orthopedics (13.1%). Forty percent of respondents reported performing surgery on three to five patients per week and 24.6% on five to 10 patients per week (Table 1).
Data are presented as number (%).
Less than half (44.3%) reported wearing double gloves. The main reasons for double gloving being “self-protection” (63%), “I am aware of double gloving recommendations” (53.1%), “protection of the patient” (23.5%), and “previous needle prick injury” (17.3%). On the other hand, the main reasons for not double gloving were as follows: “I think it is required only for special cases” (62.7%); “I feel uncomfortable” (44.1%); and “It impairs my sensation” (41.2%) (Figs. 1 and 2).

The reasons for wearing double gloves among surgeons at King Abdulaziz University Hospital.
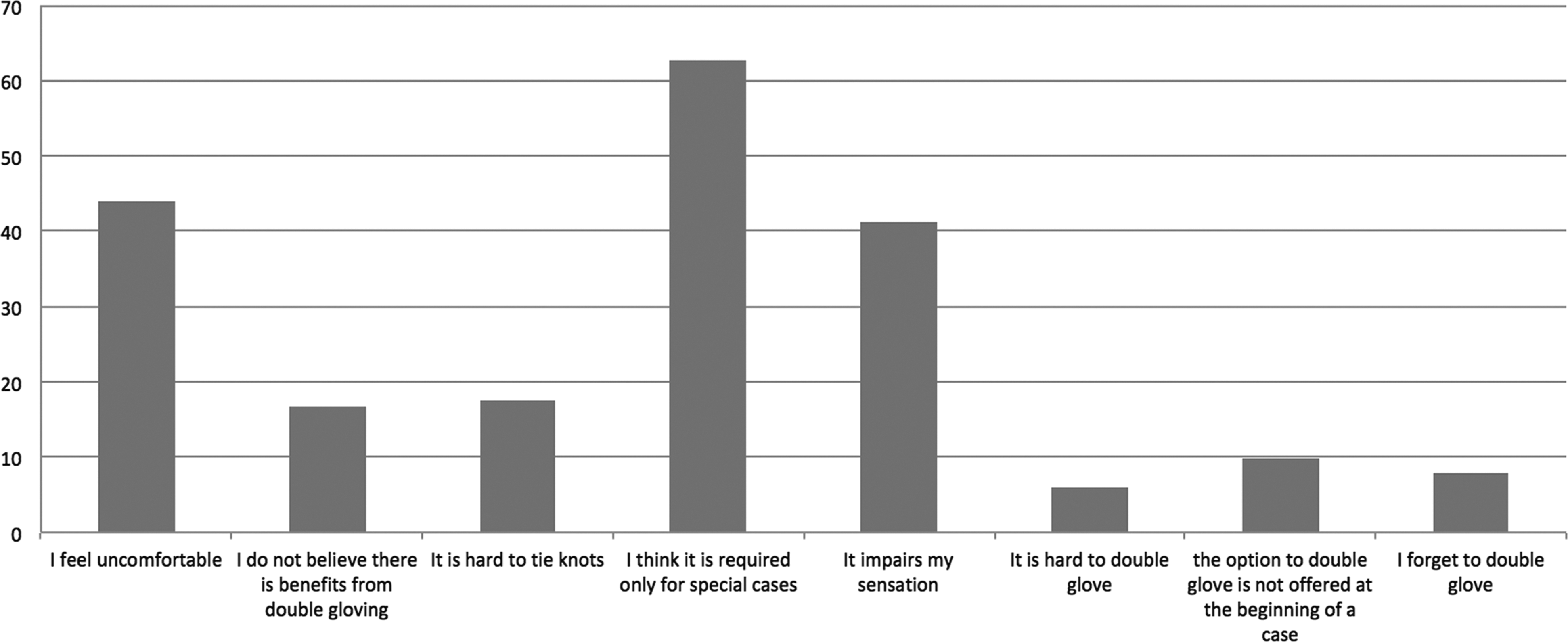
The reasons for not wearing double gloves among surgeons at King Abdulaziz University Hospital.
Among the respondents, 79.2% reported a history of needle-prick injury, whereas 44.2% reported a needle-prick injury either in themselves or in others. Most needle-prick injuries occurred during residency (68.8%) and most (80%) occurred while the surgeon wore single gloves (Table 2).
More than one response.
The results showed a significant association (p = 0.033) between wearing double gloves and subspecialties. Orthopedic surgeons had the highest percentage of double gloving at 95.8%, but only 15% of otorhinolaryngology-head and neck surgeons wore double gloves (Table 3).
More than one response.
Statistically significant, p < 0.05.
Among people who usually double glove 84% of needle-prick injuries occurred when they were not double gloved. Among the 102 surgeons who never double glove, 75.5% had a history of needle-prick injuries. Among the 68 surgeons who wear double gloves, 57% had a needle-prick injury while wearing single gloves and 43% while wearing double gloves.
Discussion
Less than half of the respondents (44.3%) in the current study reported double gloving, 43.2% of them doing so only occasionally. This compliance rate is consistent with that of another study in which double gloving was tested in two teaching hospitals (University of Western Ontario and McMaster University) and showed 43% compliance [9]. Other surveys showed that less than 30% of surgeons follow the recommendations of the American College of Surgeons for double gloving [11].
The main reason for wearing double gloves in the current study was “self-protection” (63%), which was also the most common reason given in a similar study in 2010. The investigators in that study reported that 77% of respondents selected a “decrease in the infection risk for themselves” most frequently. This is likely because of the evidence provided by several studies about the significant risk for blood-borne diseases after needle-prick injury for HBV (30%), for HBC (1.5%–3%), and for HIV (0.3%) [11,12].
The main reason for not wearing double gloves, as stated by 62.7% of the respondents in our study, was “I think it is required only for special cases.” This ideology conflicts with the concept of universal precautions in which all human blood and body fluid is treated as if infectious for HIV, HBV, and other blood-borne pathogens. The problem, however, is that not all patients are screened for blood-borne pathogens before surgery.
These diseases, in particular HBV, are common in Saudi Arabia, as the incidence in 2015 was 12.93 per 100,000. The World Health Organization recommends double gloving in countries with a high prevalence of HBV, in particular if the operation is moe than 30 minutes long [13,14]. Because of the high incidence of these infections, as well as their long-term associated disabilities, we emphasize the importance of double gloving in all cases.
The second most common reason for not wearing double gloves, namely “I feel uncomfortable,” could be easily solved by wearing gloves that are a half size larger. Consistent with the results of a previous study, the third reason (impairment of sensation) was also common [12]. This impairment of sensation felt by the surgeons when they double glove for the first time would likely be overcome with sensory cortical remapping or cortical retraining. Cortical retraining means persevering with double gloving while the brain readjusts to the new sensation. This may take as long as four months of continuous practice [15].
When a surgeon starts to double glove, it is recommended that he or she tries different glove combinations until a comfortable fit is found. It has been found that 31% preferred a larger glove inside, 35% preferred a smaller glove inside, and 31% preferred same size gloves [16].
The current study showed a significant association between wearing double gloves and subspecialty, the highest rate occurring among orthopedic surgeons. This may be because of the exposure of orthopedic surgeons to sharp injuries, which one study reported to be as much as 90% in a 10-year period from needle-prick injuries, bone spikes, and the use of sharp orthopedic instruments [17]. The lowest rate (15%) occurred among otolaryngologic surgeons, which could be because of the minor procedures they perform, with less use of prostheses but the need for tactile sensation in delicate otologic operations.
In a randomized controlled study in 2016 that evaluated the efficacy of double gloving, gloves were collected and evaluated for perforations. The perforation rate was 15.2% in single gloves and 14.4% in double gloves. However, for the double gloves, only six of 512 inner gloves perforated, a rate of 1.17%. Thus, double gloves were highly protective, with 98.83% of inner gloves remaining intact (χ2 = 280.9, p < 0.0001), despite the outer gloves being perforated [4].
Despite the fact that our study was limited to a single center, we were able to conduct anonymous surveys with a response rate of 83.2%, which reduces bias. We could not find other similar studies done in Saudi Arabia to evaluate surgeons' practice of double gloving and to determine the main factors affecting their compliance.
In conclusion, we found that less than half of respondents practice double gloving, the main reason being self-protection. The most frequently chosen reason for not wearing double gloves was that “it was required only for special cases.” There was a significant association between wearing double gloves and the surgeon's subspecialty, orthopedic surgeons showing the highest percentage of wearing double gloves among the subspecialties. Another significant association was found between wearing double gloves and previous experience with needle-prick injuries while wearing single gloves. Last, most needle-prick injuries occurred while surgeons were wearing single gloves.
Our findings are crucial for understanding surgeons' compliance with double gloving at KAUH and for determining the main factors affecting their attitude. These results may be of great value in enhancing the sterile environment recommended for surgical practice in operating rooms.
We suggest modifying the barriers to wearing double gloves by raising surgeons' awareness of its routine practice. We propose that the hospital develop awareness programs, provide double-gloving sessions, put up posters in operating rooms and for maximal compliance the hospital should enforce the double gloves as part of the operative uniform. Using a glove perforation indication system could improve the perforation detection during surgery. Considering that the risks of needle-prick injuries are part of the job, they should be brought to the attention of surgeons.
Footnotes
Author Disclosure Statement
No competing financial interests exist.