
Abstract
Abstract
Background and Purpose:
For patients at high risk, such as those with lower-gastrointestinal perforations, it is important to establish a preventive method that reduces the incidence of surgical site infections (SSIs) significantly. We applied negative-pressure wound therapy (NPWT) as part of a delayed primary closure approach to prevent SSIs. This study evaluated the value of this technique.
Methods:
We included prospectively 28 patients undergoing abdominal surgery for peritonitis caused by a lower-gastrointestinal perforation between May 2014 and November 2015. Historical controls comprised retrospective data on 19 patients who had undergone primary suturing for managing peritonitis incisions for a lower-gastrointestinal perforation from January to December 2013.
Results:
We found a significant association between the SSI incidence and the type of incision management (10.7% with NPWT and delayed closure vs. 63.2% with primary suturing; p < 0.001). There was no significant difference between the groups in the length of the hospital stay (22 days for NPWT and delayed closure vs. 27 days for primary suturing; p = 0.45). No severe adverse events were observed related to NPWT.
Conclusion:
The use of NPWT and delayed primary closure was an effective measure for preventing SSI in patients undergoing abdominal surgery for peritonitis caused by lower-gastrointestinal perforation.
C
Surgical site infections are responsible for increasing morbidity in patients who undergo abdominal surgery. Moreover, SSIs incur additional hospital care costs through longer stays, which amount to more than US$1.5 billion in excess cost in the United States [6]. These infections also are associated with a higher risk of incisional hernia [7,8]. Although several risk factors for SSIs have been described and are being corrected, the incidence remains disturbingly high [9,10]. Therefore, particularly for patients at high risk, such as those with lower-gastrointestinal perforations, it is important to establish a preventive method that can reduce the SSI incidence significantly.
Delayed primary closure (DPC) is a commonly used method for treating dirty incisions. The method is applicable to either contaminated or dirty sites; it allows soft tissue fluids to drain from the open areas, and the skin is closed a few days later. Although a previous meta-analysis failed to provide definitive evidence of DPC efficacy [11], some randomized studies on contaminated abdominal incisions showed that DPC reduced the SSI incidence compared with conventional primary closure (PC) [4,12]. Additionally, negative-pressure wound therapy (NPWT) has been used for managing open abdominal incisions [13,14] and treating infected abdominal walls [15].
Several recent studies have reported that, compared with conventional incision dressings, NPWT reduced the risk of SSI in patients with a primary closed abdominal surgical incision after a high-risk repair [16-18]. However, the quality of the evidence was low in those observational studies. Moreover, the World Health Organization emphasized that the devices used for NPWT are expensive, and prioritization should be considered carefully [18].
Therefore, we focused on peritonitis surgery, with the infection resulting from lower-gastrointestinal perforations. This scenario is characterized by a particularly high SSI rate. In our institution, NPWT has been applied as part of the DPC approach to create an optimal incision-healing environment. This prospective cohort study was performed to evaluate the effect of NPWT on the rate of SSIs after abdominal surgery for peritonitis secondary to lower-gastrointestinal perforation. We hypothesized that the application of NPWT as part of the DPC approach would reduce the incidence of SSIs.
Patients and Methods
Study design and patient treatment
This prospective cohort study included all patients who underwent abdominal surgery for a lower-gastrointestinal perforation in our hospital between May 2014 and November 2015. Starting in May 2014, we implemented the NPWT treatment (described below) for all patients as a basic policy, and prospective data were recorded. The extent of peritonitis was identified by surgeons at the time of surgery. We targeted patients with peritonitis for NPWT, and any patient with a localized abdominal abscess was excluded. For the NPWT procedure, the peritoneum, muscle, and fascia were closed in one layer with polydiaxanone sutures, but the skin and subcutaneous tissue incisions remained open. Open subcutaneous tissues were packed with gauze soaked in normal saline. All NPWT placements of black GranuFoam dressing (V.A.C.® Therapy, Kinetic Concepts Inc. [KCI], San Antonio, TX) were initiated within three days of surgery, and treatment continued for five to seven days. Dressing changes were performed every 48 to 72 hours no fewer than three times per week. Negative pressure was set at 100 mm Hg, with continuous suction. When detectable wound granulation had formed, and the wound appeared clean, it was closed with a vertical mattress suture under local anesthesia in the patient's room (DPC). All patients received peri-operative intravenous antibiotics with anaerobic coverage until they achieved normalizations of body temperature, white blood cell count, and gastrointestinal function. Patients were excluded when naked blood vessels were present in the wound or a fistula was found in the abdominal cavity; when an uncontrolled organ-space SSI was present; when they exhibited any contraindications to the V.A.C.® therapy device [19]; or when they were judged unsuitable for this therapy by an attending physician.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study was approved by the Institutional Review Board of Osaka General Medical Center (approval no. 29-S0901). For this type of study (retrospective), informed consent is not required.
Demographics
The following data were collected for all patients: Age, sex, body mass index, bacteria cultured from ascites fluid, time to epithelialization (time to achieve complete wound closure), NPWT device application time, length of post-operative hospital stay (LOS), and the presence of SSIs. We also recorded underlying medical conditions that could contribute to infectious complications, including diabetes mellitus, obesity, malnutrition, steroid use, and the presence of a stoma.
Epithelialization was defined as a state in which the wound was covered with the epithelium, no wound exudate was present, and gauze or wound dressings were unnecessary. Surgical site infections were defined according to the National Nosocomial Infectious Surveillance System of the CDC [2]. Treatment-related adverse events (AEs) were evaluated according to the Common Terminology Criteria for Adverse Events (CTCAE) version 4.0.
Historical controls
We assessed whether NPWT reduced the SSI incidence, shortened the time to epithelialization, and lowered the LOS compared with conventional PC. For controls, we retrieved historical records of patients who underwent conventional PCs to manage peritonitis incisions occasioned by lower-gastrointestinal perforations from January to December 2013. During that year, all patients who underwent abdominal surgery for lower-gastrointestinal perforations in our hospital had conventional PCs. All patients received peri-operative intravenous antibiotics with anaerobic coverage until they achieved normalizations of body temperature, white blood cell count, and gastrointestinal function.
Statistical analysis
Continuous data are presented as the median and range; categorical data are presented as the frequency and percentage. The χ2 or Fisher exact tests and the non-parametric Mann–Whitney U test were used to compare demographic or clinical characteristics between groups. A two-sided p value <0.05 was considered statistically significant. JMP® 10 (SAS Institute Inc., Cary, NC, USA) was used for all statistical analyses.
Results
From May 2014 to November 2015 (19 months), 47 patients underwent surgery for peritonitis secondary to a lower-gastrointestinal perforation at Osaka General Medical Center. Of these patients, 40 were found to have peritonitis, but 11 were ineligible for the study (Fig. 1). Of those 11 patients, four had contraindications to the V.A.C. therapy device, and seven were judged unsuitable for this therapy by an attending physician. One had a mental disorder; six could not start NPWT because of insufficient preparation of the equipment. Of the remaining 29 patients, one was excluded by a protocol violation. Thus, we compared 28 patients who received NPWT+DPC with 19 patients who received PC. These groups were not significantly different with regard to age, sex, Body Mass Index, risk factors, or stoma formation (Table 1).
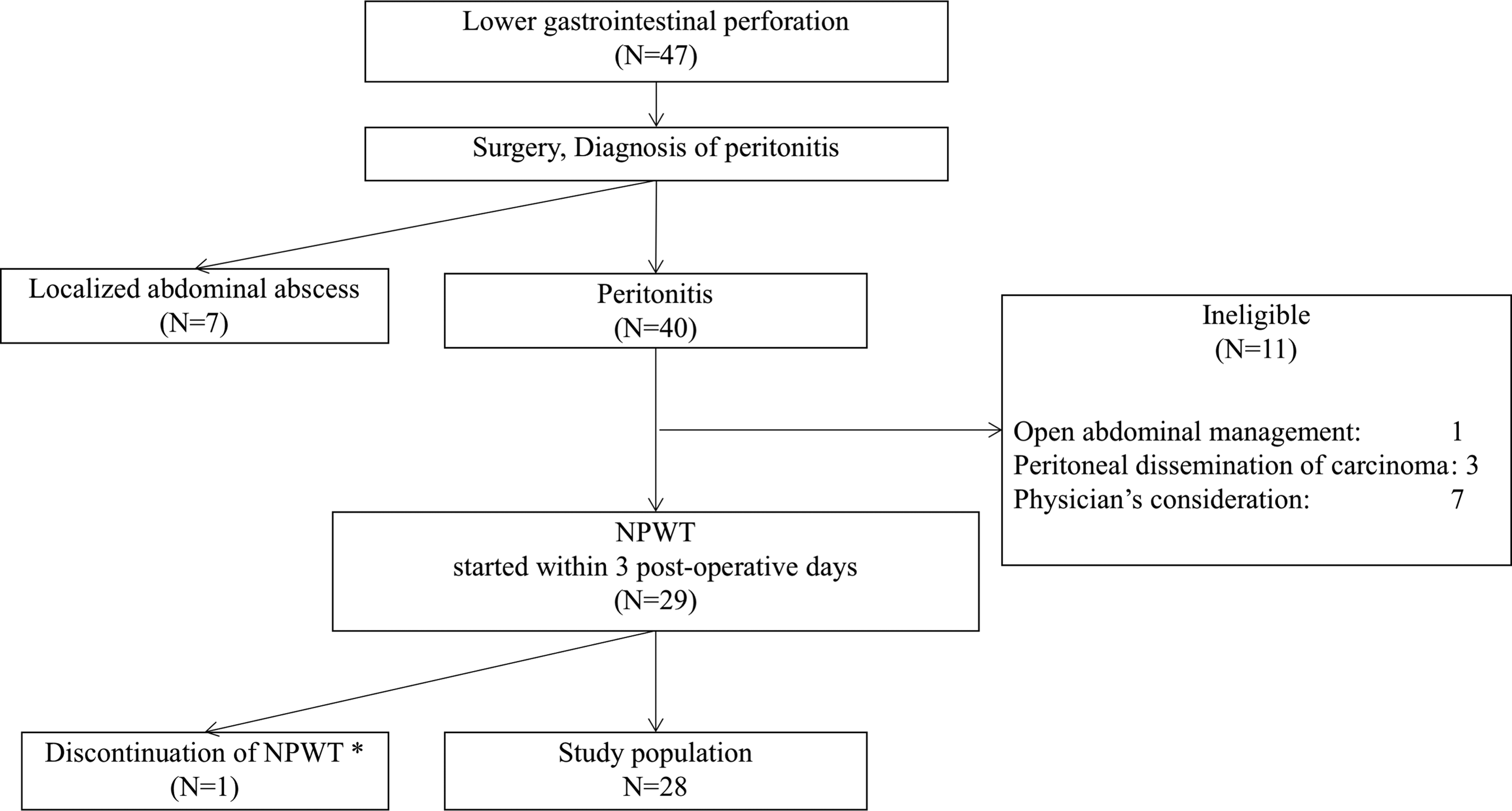
Flow chart of patient selection procedure. *Discontinuation because of protocol violation. NPWT = negative-pressure wound therapy.
NPWT, negative pressure wound therapy; DPC, delayed primary closure; PC, primary closure
Bacterial cultures from the ascites fluid were positive in 39 patients (83.0%). Bacteroides spp., which are anaerobic organisms, were identified in 19 patients (40.4%). The most common organisms cultured were Bacteroides, Escherichia coli, and various Enterococcus spp. (Table 2). There were three SSIs in the NPWT+DPC group (10.7%). In addition, two patients with incisions unsuitable for suture failed to complete the DPC. Their incisions were repaired by the formation of granulation tissue. Consequently, a total of five patients developed SSIs or failed the DPC (17.9%).
DPC = delayed primary closure; NPWT = negative-pressure wound therapy; PC = primary closure.
The PC group had 12 incision infections (63.2%). There was a significant association between the incidence of SSIs and the type of incision management (NPWT+DPC: 10.7% vs. PC: 63.2%; p < 0.001). However, the mean hospital stay was not significantly different, although the LOS of the patients having NPWT tended to be shorter (NPWT+DPC: 22 days vs. PC: 27 days; p = 0.45). Moreover, there was no significant difference between the groups in the time to epithelialization (Table 3).
DPC = delayed primary closure; NPWT = negative-pressure wound therapy; PC = primary closure.
The incidence of treatment-related AEs from the time of therapy initiation is shown in Table 4. No severe AEs related to NPWT were observed. Two patients exhibited bleeding at the time of changing the foam that was stopped with simple compression. Two patients experienced pain that did not require analgesics. On the other hand, two patients exhibited abdominal wall hematomas after the DPC, and both developed SSIs.
CTCAE = Common Terminology Criteria for Adverse Events; DPC = delayed primary closure.
Discussion
Negative-pressure wound therapy is a novel approach in site-healing management in gastrointestinal surgery, with several benefits that may contribute to healing. In particular, open drainage evacuates interstitial fluids and cellular debris continuously, which increases local tissue blood perfusion and vascularization and stimulates the formation of granulation tissue [20].
Moreover, incision tissues are deformed by the porous open-cell sponge used in V.A.C. therapy. This stretching of individual cells promotes cell proliferation in the incision microenvironment [21]. In other words, it is important for the porous open-cell sponge to maintain contact with the site surface. Several authors have recently reported that NPWT reduced the incidence of SSIs in patients with primarily closed abdominal incisions that were thought to be at high risk of infection [16,18]. In contrast, a review of previous NPWT treatments showed no benefit in patients with complicated contaminated hernias [22]. That finding might indicate that the effectiveness of this intervention is limited in highly contaminated surgical incisions. However, the present study reported preliminary results from a case series that comprised patients with incisions created during lower-gastrointestinal perforation surgery, which are highly contaminated, being class III/IV according to the surgical incision classifications described in the CDC guidelines [3]. Because of the highly contaminated nature of these sites, we considered it inappropriate to apply the NPWT in closed incisions. Moreover, in Japan, the Pharmaceuticals and Medical Devices Agency approved NPWT in November 2009 only for the treatment of non-healing open sites. Since then, the indications have not been expanded. Therefore, the use of a NPWT device in closed incisions would be considered off-label use.
To our knowledge, this study is the first to evaluate the application of NPWT to incisions associated with lower-gastrointestinal perforation surgery for the prevention of SSIs. The emergency status of the patients in this study indicated that this group was at extremely high risk of SSIs; thus, the efficacy of NPWT could be assessed most easily in this group. Our comparison of the two study groups confirmed that the NPWT was an effective preventive measure against SSIs in patients undergoing abdominal surgery for peritonitis resulting from lower-gastrointestinal perforation.
One limitation of this study was the difficulty in analyzing whether the NPWT provided benefit in addition to the DPC in preventing SSIs. Bacterial contamination of the incision during surgery is the major risk factor in the development of SSIs. In the present study, we obtained bacterial cultures of the ascites fluid of 39 patients (83.0%; Table 2). The benefits of NPWT were most likely attributable to the constant drainage of contaminated wound effluent, which can interfere with incision healing.
Extended hospital stays, considered an indirect predictor of the overall cost of treatment, were reported to be an economic concern associated with the DPC method [23]. We assumed that the time required to install the NPWT device and then close the skin definitively might be offset by the reduction in SSI incidence. However, the LOS and the time to epithelialization were not significantly different in the two groups (Table 4). Many patients in the NPWT group exhibited shortened times to epithelialization, but because of the small number of patients in this study, the difference between groups was not statistically significant (Fig. 2).

Time to epithelialization for patients with peritonitis treated with negative-pressure wound therapy (NPWT) and delayed primary closure (DPC) or with conventional primary closure (PC).
We also showed that NPWT was associated with only a few AEs. In several cases, skin itching, pain, and minor bleeding were noted at the site of application. However, these AEs resolved rapidly with local treatment and temporary device discontinuance. Moreover, NPWT was convenient, because the incision dressing required replacement only two or three times per week.
This study had some limitations. The decision of whether to apply the NPWT was at the discretion of the attending physician, and not all attending physicians in the study accepted NPWT. Although it was possible that the NPWT might have been used in patients at lower risk of SSIs, in fact, all cases were considered to be at very high risk in this situation. In one case, the hesitation in introducing the NPWT was attributable to the patient's mental disorder. In all other cases, the reasons for avoiding NPWT were related to the arrangement or technical problems with this instrument. Other limitations of this study were those inherent in its non-randomized nature, its single-center small cohort design, and the comparison with historical controls. A randomized study would strengthen the analysis, but the randomized design is not always feasible in an emergency surgical setting because of ethical concerns. Currently, we are planning to conduct a prospective multi-center cohort study, which is expected to provide further information. To date, we have enrolled some patients, and we have registered the trial in the University Hospital Medical Information Network (UMIN) system (UMIN ID: 000020391)
In conclusion, our data support the use of NPWT as part of the DPC approach. We showed that NPWT prevented SSIs in most patients undergoing abdominal surgery for peritonitis secondary to a lower-gastrointestinal perforation.
Footnotes
Author Disclosure Statement
No competing financial interests exist.