
Abstract
Abstract
Aim:
To evaluate the efficacy of ultrasound-guided (USG) fine-needle aspiration cytology examination (FNAC) of the omentum in the diagnosis of abdominal tuberculosis (TB).
Methods:
Retrospective review was conducted of data from patients who presented with clinically suspected peritoneal TB between June 2016 and April 2018. We included patients in whom imaging showed omental thickening with or without ascites. Additional features that were assessed on imaging included ascites, the presence of mesenteric or retroperitoneal adenopathy, ileocecal thickening, and involvement of solid abdominal organs. Ultrasound-guided FNAC of the omentum was performed using a 22-gauge needle. The cytologic assessment was done for granulomatous inflammation, bacilli on Zeihl-Neelson stain, and for other pathology if any.
Results:
During the study period, 35 omental FNACs were done. Of these patients, malignancy was reported in eight (22.8%). Of the remaining 27 patients, positive results for TB were reported in 19 patients (70.4%). In these 19 patients with positive FNAC, the median age was 33 years (range 10–63 years), with eight males (42.1%). Ascites was present in 14 (73.7%), abdominal lymphadenopathy was present in 9 (47.4%), ileocecal thickening and involvement of solid abdominal organs were reported in 3 (15.8%) and 4 (21%) patients, respectively. Granulomatous inflammation was reported in 17 (89.5%) and acid-fast bacilli in 10 (57.6%) patients. The Genexpert analysis was done in two patients, with a positive result in one patient.
Conclusion:
Ultrasound-guided FNAC of the omentum is helpful to diagnose abdominal TB in patients having omental thickening with or without other abnormal findings.
T
The lung is the primary site of involvement for TB. The percentage of patients with extrapulmonary TB (EPTB) in tertiary-care centers in India was between 30% and 53%, whereas that estimated by the national control program in India for human immunodeficiency virus-negative adults is between 15% and 20% [6]. There is a paucity of data from clinical trials in EPTB, so most of the information regarding diagnosis and management is extrapolated from pulmonary TB [7]. Abdominal involvement occurs in about 11%–12% of patients with extrapulmonary TB [8–10]. Abdominal lymphadenopathy is the most common manifestation of abdominal TB [11, 12]. In the gastrointestinal tract, the ileocecal region is the site most commonly involved. Peritoneal involvement may result from lesions of lymph nodes, intestine, or adnexa (in females). Abdominal lymph node and peritoneal involvement may occur in the absence of gastrointestinal involvement in as many as one third of cases.
Timely diagnosis of TB is of paramount importance for treatment. Because TB is a great mimicker of other diseases both radiologically and clinically, especially in the abdomen, tissue sampling is needed for histopathology analysis as well as bacteriological examination. In the past, this could be achieved only by open surgical biopsy. During recent times, fine-needle aspiration cytology (FNAC) has been shown to be a safe, reliable, and cost-effective method for tissue sampling. Non-guided FNACs have been used for palpable lumps in abdominal TB in past; however, only 40% of patients have a palpable lump at the time of diagnosis [13]. For both palpable and non-palpable lesions, ultrasound-guided (USG) FNAC is a safe, less invasive, and effective method wherein the radiologist plays an important role. The role of FNAC in the diagnosis of abdominal TB has been studied, but the sites of FNAC have been variable, and omental sampling has not been studied specifically [14–16]. To the best of our knowledge, the present study is the first to evaluate the role of USG omental FNAC in the diagnosis of abdominal TB.
Patients and Methods
This was a retrospective study of patients who presented to us with clinically suspected peritoneal TB between June 2016 and April 2018. We included those patients in whom imaging showed omental thickening with or without ascites (Fig. 1A). Additional features that were assessed on imaging were ascites, the presence of mesenteric or retroperitoneal adenopathy, ileocecal thickening, and involvement of solid abdominal organs.
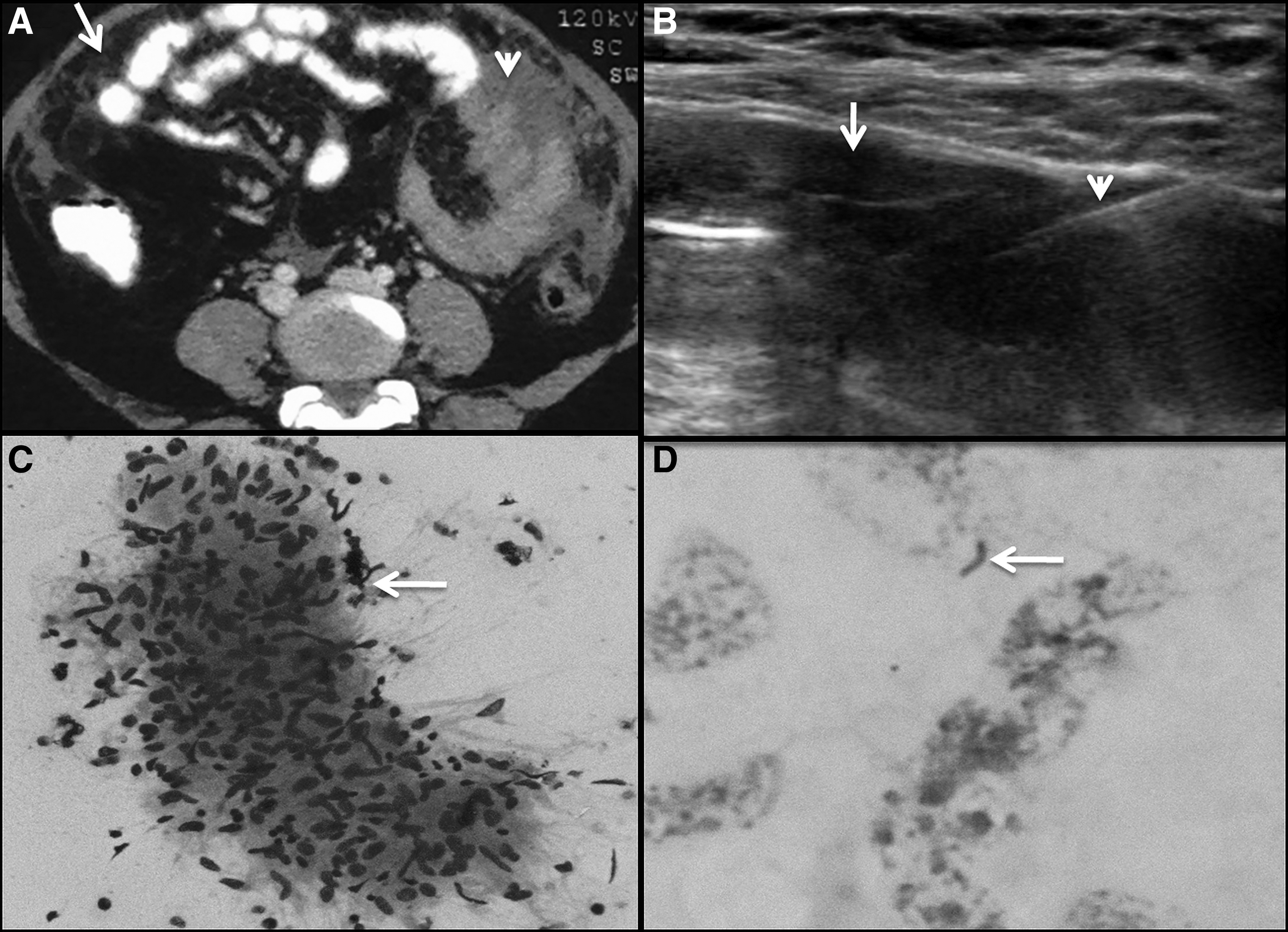
Omental images of case. (
Ultrasound scanning was performed in all these patients to document omental thickening using a linear probe (bandwidth 6–15 MHz; LOGIQ S8, General Electric, Chicago, IL, USA) (Fig. 1B). Informed written consent was obtained prior to FNAC. All patients underwent blood investigations to before the procedure to rule out bleeding disorders. The FNAC was done on an outpatient basis. It was performed from omental thickening using a 22-gauge needle. Under real-time USG, using aseptic precautions, the needle was introduced using the freehand technique. Aspiration was carried out moving the needle forward and backward but making sure that tip remained within the abnormal omentum during aspiration. On-site assessment of the adequacy of the sample was done by the cytopathologist. One or two passes were made in each patient depending on the adequacy of the material recovered. Multiple smears were prepared. May-Grunwald-Giemsa and Zeihl-Neelson (ZN) stains were carried out in all cases. The cytologic assessment was done for granulomatous inflammation, bacilli on ZN stain, and other pathology if any (Fig. 1C, D). Wherever requested by clinicians, GeneXpert was done. A positive result (for TB) was defined by the presence of granulomatous inflammation, detection of acid-fast bacilli on ZN stain, or positive GeneXpert results.
We also divided the cases of TB into confirmed (AFB or Xpert positive) or clinically diagnosed (presence of granulomatous inflammation). Variables are reported as median and percentages. The difference in the yield of FNAC in patients with omental thickening with ascites compared with those without it was assessed using the χ2 test.
Results
During the study period, 35 omental FNACs were done. Salient findings are shown in Table 1. Malignancy was reported in eight patients (22.8%), and these cases were excluded from the study. Of the remaining 27 patients, positive results consistent with the diagnosis of TB were reported in 19 (70.4%); in the others, FNAC examination was inconclusive. The 19 patients with TB-consistent findings were included in our analysis.
Salient Findings in 19 Patients with Positive Omental Fine-Needle Aspiration Results
Abbreviations: AFB = acid-fast bacteria; IC = ileocecal.
Of the 19 patients with positive FNAC findings, the median age was 33 years (range 10–63 years), with eight males (42.1%). Ascites was present in 14 (73.7%), abdominal lymphadenopathy in nine (47.4%), and ileocecal thickening and involvement of solid abdominal organs in three (15.8%) and four (21%) patients, respectively. The abdominal organs involved were the ovaries (n = 3) and spleen (n = 1).
Among positive FNAC results, granulomatous inflammation was reported in 17 patients (89.5%) and AFB in 10 (57.6%). GeneXpert analysis was done in two patients with a positive result in one. In this last patient, neither granulomatous inflammation nor AFB could be detected. In one patient, AFB were detected in the absence of granulomatous inflammation. Therefore, 12 patients (63%) had a confirmed diagnosis of omental TB, whereas seven (37%) had clinically diagnosed TB.
Of the 27 patients included in the study, there was no statistically significant difference in the yield of FNAC between patients with omental thickening and ascites and those without.
Discussion
India has one of the highest TB burdens [4, 5]. Tuberculosis is one of the greatest disease mimickers, and abdominal TB is difficult to diagnose clinically, requiring a high index of suspicion. Because peritoneal TB is the commonest presentation of abdominal TB, evaluation for peritoneal involvement in suspected cases is important for early diagnosis [11, 12].
Peritoneal involvement in TB (tuberculous peritonitis) is subdivided into three main types; i.e., wet, fibrotic, and dry [17]. Considerable overlap may be seen in these presentations [18]. Wet peritonitis is the most common, in which patients present with a large volume of ascites with or without loculations. The ascites is exudative, and there can be smooth and diffuse peritoneal thickening. Fibrotic peritonitis describes large omental and mesenteric masses and remarkable omental thickening with clumping of bowel loops. Dry peritonitis presents with fibrous adhesions and mesenteric and peritoneal thickening with caseous nodules. A relatively rare entity, abdominal cocoon or sclerosing encapsulating peritonitis, also has been reported with abdominal TB, which usually presents as intestinal obstruction [18].
In the past, non-guided FNACs have been used for sampling tissues from palpable abdominal lumps for the diagnosis of TB; however, only a few patients will have a palpable mass at the time of presentation [13]. These masses usually represent matted and thickened bowel loops, mesenteric lymphadenopathy, thickened omentum, or loculated ascites [13]. Image-guided FNAC is recommended in preference to non-guided FNAC as the lesion, as well as the needle, can be visualized to ensure accurate needle placement. Ultrasound guidance is widely accepted for FNAC of abdominal lesions [14], as the method is simple, safe, and effective for both palpable and non-palpable lesions. In a study by Das and Pant, USG helped in obtaining an adequate tissue sample in a significantly higher percentage of bowel lesions (84.6%) than did non-guided FNACs (61.5%) [15].
There is limited literature regarding the role of USG FNAC in the diagnosis of peritoneal TB. In the study by Suri et al. [14], describing the role of USG FNAC in abdominal TB, 58% of patients had confirmed TB with the remainder showing either necrosis or negative results. However, the sites of FNACs included abdominal lymph nodes (n = 14), thickened bowel loops in the ileocecal region (n = 7), and focal splenic (n = 8) and liver (n = 2) lesions, some of which might be difficult to locate to sample. Our aim was to determine the feasibility and effectiveness of omental FNA. Omentum, being relatively superficial, can be targeted easily under imaging guidance.
In our study, 19 patients had positive results, of which 17 had granulomatous inflammation. Granulomatous inflammation without caseous necrosis also can be seen in other diseases such as mycosis or sarcoidosis. However, in countries such as India, the finding of granulomatous inflammation in omentum is considered attributable to TB unless proved, otherwise, given the high burden of this infection. We did not find a statistically significant difference between the yield of FNACs in patients with and without ascites.
As far as GeneXpert is concerned, only a small number of patients were tested in the present series, and further studies may determine the utility of this test in omental FNAC samples. The test is a rapid, automated, molecular test for TB, which diagnoses the infection by detecting the presence of Mycobacterium tuberculosis, as well as testing for its resistance to drugs. We hope to incorporate this test in the future.
Our study has a few limitations. We had a small patient cohort. Also, correlation with culture results, ascitic fluid analysis, and ascitic fluid adenosine deaminase was not done. The final diagnosis in inconclusive cases thus was not known.
In conclusion, USG FNAC of omentum is an effective method to diagnose abdominal TB in patients having omental thickening with or without other findings. We believe our results will stimulate further research in this area of importance, especially in the developing world.
Footnotes
Author Disclosure Statement
The authors have no conflicts of interest or financial disclosures related to this manuscript.